Fluid Therapy for Horses With Gastrointestinal Diseases
Tiffany L. Hall
Most horses with acute gastrointestinal disturbances require fluid therapy to address decreased intake or excessive loss of fluids and to correct any alterations in acid-base and electrolyte balance.
Conditions such as high-volume diarrhea and gastric reflux necessitate aggressive fluid therapy to correct hypovolemia, whereas other conditions (including intraluminal impactions) may necessitate a more conservative approach to maintain appropriate hydration. Assessment of hydration status and acidbase balance in horses presenting with gastrointestinal disease, as well as an understanding of the primary gastrointestinal condition, is critical for developing a fluid therapy plan. This section focuses on fluid therapy in horses with gastrointestinal disease. (For a more in-depth discussion of critical care and fluid therapy for horses, including selection of fluid types, monitoring and assessing fluid resuscitation, and complications associated with fluid therapy, see Fluid Therapy for Horses With Gastrointestinal Diseases section and Chapter 44.)■ Identifying Patients Requiring Fluid Therapy Clinical assessment begins with distinguishing hypovolemia from dehydration (Fig. 32.75). Hypovolemia is an emergency caused by an acute decrease in circulating blood volume that results in decreased tissue perfusion, anaerobic metabolism, organic acidosis, and ultimately shock. Clinical diagnosis of hypovolemia is based on altered perfusion parameters, including increased jugular refill time, prolonged capillary refill, tachycardia, poor peripheral pulse quality, decreased extremity temperature, decreased urine production, altered mentation, or a combination of these. Dehydration, on the other hand, is associated with a more insidious decrease in total body water and is reflected by clinical signs such as decreased skin turgor, decreased tear film, sunken eyes, and tacky mucous membranes.
Laboratory parameters are beneficial for evaluating hydration status, developing a fluid plan, and monitoring response to therapy. PCV and measurement of plasma total solids are commonly used to assess hypovolemia; however, these are neither sensitive nor specific. Splenic contraction and protein loss are two conditions common in horses with acute abdomen that affect the clinical utility of PCV/total solid values alone in assessing hydration. PCV/total solid values are most useful when greatly increased or when measured serially to monitor the response to fluid therapy.
An increase in the concentration of blood lactate serves as an indicator of decreased tissue perfusion. The most common causes of increased lactate in horses with gastrointestinal disease are hypovolemia, sepsis, and intestinal ischemia secondary to strangulation. Lactate can be measured in the field on whole blood with handheld analyzers. Increased blood lactate concentrations were associated with worse outcomes in equine colic1 and should be suspected in cases of metabolic acidosis (decreased pH, negative base excess) in the absence of hyperchloremia or hyponatremia.2
Plasma or serum creatinine concentrations are useful for assessing hydration status in the absence of renal dysfunction. Creatinine concentrations up to 3.5 mg/dL (310 pmol/L) are common with moderate to severe hypovolemia and can be as high as 5 mg/dL (450 μmol/^ with prolonged or
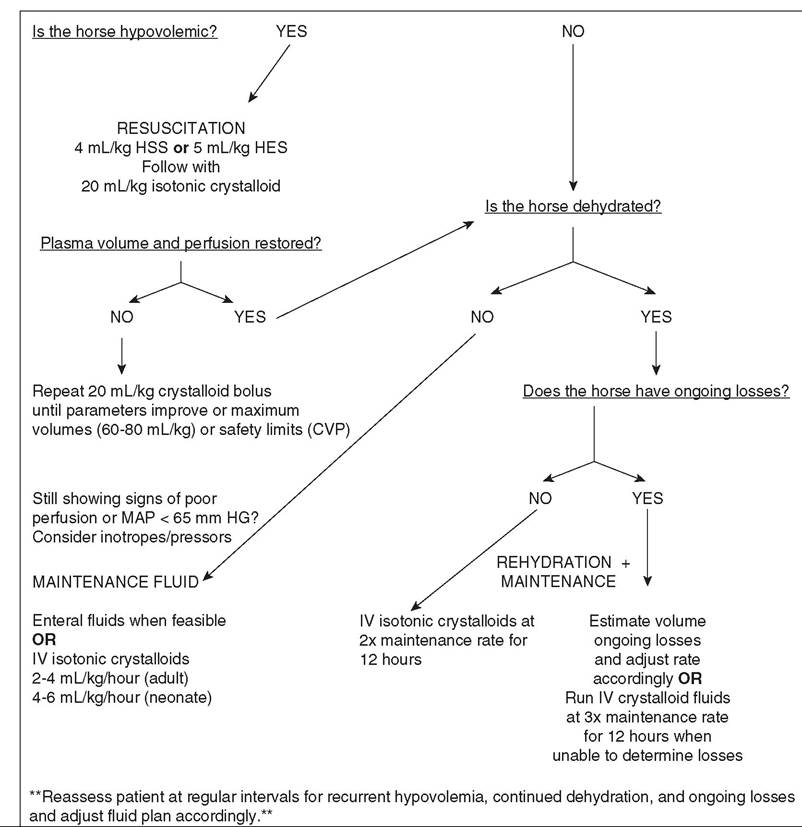
FIG. 32.75 Clinical assessment of perfusion parameters and hydration status. CVP, Central venous pressure; HES, hydroxyethyl starch solution; HSS, hypertonic saline solution; MAP, mean arterial pressure.
marked hypovolemia. Even in severe hypovolemia, the creatinine concentration does not increase by much more than 2.3 mg/dL (200 pmol/L) per day.3
Urine specific gravity provides valuable information regarding renal function and hydration status.
High urine specific gravity (>1.040) indicates probable dehydration and normal renal function. Isosthenuria (levels of 1.010 to 1.015) indicates possible renal damage or a recent high fluid load. Urine specific gravity is especially useful in monitoring hydration status of neonates, inasmuch as neonates are normally hyposthenuric (therapy are to increase cardiac output, by increasing and then maintaining cardiac preload; improve oxygen delivery; and correct electrolyte and acid-base disturbances. The plan for fluid therapy consists of four overlapping phases: (1) resuscitation, (2) rehydration, (3) maintenance, and (4) ongoing loss replenishment. Frequent monitoring of the patient and adjustment of the fluid plan are also important to a successful outcome. The fluid plan should be based on the clinical status of the affected horse, an understanding of the primary disease process, and any laboratory information available.RESUSCITATION. Rapid fluid resuscitation is indicated in horses with clinical signs of hypovolemia. Reversal of hypovolemia is associated with improved outcome in human medicine and is shown to improve cardiovascular parameters in horses.5-7 Balanced polyionic, isotonic crystalloid solutions are frequently used to restore circulating volume in hypovolemic equine patients; however, the use of colloids or hypertonic crystalloid solutions, or both, may provide more rapid results when available and indicated.
Small-volume resuscitation with hypertonic crystalloid or colloid solutions, or both, has been promoted to rapidly restore plasma volume in horses presenting with signs of hypovolemia.8 The administration of hypertonic saline solution (HSS) was found to restore plasma volume and induce urination more rapidly than administration of an equal volume of isotonic crystalloids.9 Hetastarch has been shown to increase circulating blood volume and improve tissue perfusion, as evidenced by decreases in heart rate and urine concentration after administration of hetastarch (10 mL/kg) with concurrent isotonic saline (10 mL/kg) to horses with colic.10 Moreover, in horses undergoing exploratory laparotomy, cardiovascular indices were significantly improved after preoperative administration of 10% pentastarch (4 mL/kg), in comparison with 7.2% saline (4 mL/ kg).11 The administration of HSS is associated with development of an inorganic acidosis and hypokalemia, and the plasma expansion effects of small-volume resuscitation are short-lived; thus fluid therapy with hypertonic or colloid solutions should include concurrent administration or immediate follow-up with polyionic, isotonic crystalloid solutions.8,9
During resuscitation, isotonic crystalloid solutions are administered at doses of 20 to 40 mL/kg in adult horses (10 to 20 mL/kg in neonates) as rapid boluses.
After each 20-mL/kg bolus, clinical evaluation of the patient, including evaluation of perfusion parameters, is performed in order to assess the need for repeat boluses. If perfusion parameters and blood pressure have not normalized on obtaining a normal CVP or at the completion of a total maximum “shock dose” of 60 to 80 mL/kg crystalloids, then inotropes and pressors are often incorporated in treatment, and the fluid rate is adjusted to maintenance rates. In horses and foals presenting for gastrointestinal disorders, alterations in vascular permeability and decreases in protein concentrations must be considered in determining the volume of crystalloid to be administered.REHYDRATION. In horses that do not present with signs of hypovolemia or in whom hypovolemia has been reversed, dehydration is corrected over the first 12 to 24 hours of hospitalization. To rehydrate patients, isotonic crystalloids are administered at rates in excess of ongoing losses plus maintenance requirements. Clinically, this is accomplished in most patients with gastrointestinal disease by administration of isotonic crystalloid fluids at two to three times the maintenance rate. Once dehydration is corrected, according to clinical parameters such as PCV/total solids and urine specific gravity, this rate is slowed to that needed to maintain hydration. Horses with urine specific gravities below 1.020, and foals with urine specific gravities below 1.010, are unlikely to be dehydrated.
MAINTENANCE. Depending on the gastrointestinal disease, free-choice feed and water may be withheld from horses with acute abdomen for a period of time, during which fluid requirements must be supplemented to maintain hydration. The mean daily water intake (including the water content of feed) of normal resting adult horses is 57 to 64 mL/kg/day at ambient temperatures of 5° C to 25° C (41° F to 77° F). Mares restricted to 40 mL/kg/day demonstrated significant dehydration.12 Maintenance fluid rates for adult horses (2 to 4 mL/kg/h) and neonatal foals (4 to 6 mL/kg/h) can be met through enteral administration when appropriate for the diagnosis and when gastrointestinal function is normal.
When enteral administration is contraindicated, polyionic, isotonic crystalloids are most frequently used in the parenteral administration of fluids.Electrolyte concentrations and hydration status should be monitored frequently as part of the maintenance fluid plan. Replacement crystalloid solutions higher in electrolyte concentrations are usually administered over maintenance crystalloid solutions according to the size of equine patients, the volume of fluids required, and availability. (See Chapter 44 for a comparison of commercially available fluid solutions.) Some patients, particularly neonates or those losing large volumes of fluid, are at risk for developing a free water deficit and subsequent inorganic acidosis when maintained on isotonic, replacement, crystalloid solutions. Monitoring of electrolytes, particularly sodium and chloride, helps identify such patients. In adult horses, physical examination and monitoring of body weight, PCV/total solids, creatinine concentrations, and urine specific gravity are useful in evaluating the efficacy of a fluid treatment plan. Overhydration in adults with normal renal function may be indicated by frequent urination, urine specific gravity lower than 1.013, and development of dependent edema. In neonates, body weight, urine production, urine specific gravity, and perfusion parameters are evaluated to monitor hydration status; detection of excessive fluid supplementation can be difficult because nursing neonates normally produce hyposthenuric urine. Development of preputial or stifle edema is an indication of overhydration in neonates. It is important that the volume of all intravenous solutions and enteral feedings be accounted for when fluid rates in neonates are calculated to prevent volume overload.
ONGOING LOSS REPLENISHMENT. Horses that present with gastrointestinal conditions that result in excessive fluid losses such as gastric reflux and diarrhea require supplementation in excess of maintenance fluid rates.
Calculating the volume of fluid lost is the most accurate method of determining how much fluid will need to be replaced. Whereas the volume of nasogastric reflux can be tracked, determining the volume of fluid lost in adults and ambulatory foals with diarrhea is not possible; therefore frequent assessment of the patient by clinical examination and determination of relevant laboratory parameters are useful in evaluating the fluid plan to prevent continued dehydration or recurrence of hypovolemia.■ Special Considerations in the Fluid Therapy Plan The selection of fluids to be administered, rate and route of administration, parameters to be monitored, and frequency of monitoring are based on thorough individual case assessment. In addition to the various phases of fluid therapy, special circumstances encountered in horses with gastrointestinal disease must also be considered in the fluid therapy plan. These include commonly observed electrolyte disturbances, acidemia, hypoproteinemia, and endotoxemia. Table 32.11 lists common fluid choices and additives for conditions observed in horses with gastrointestinal disease.
■ Enteral Fluid Administration Enteral fluid therapy may be sufficient to correct and maintain hydration in horses with gastrointestinal disease that have mild dehydration and normal small intestinal function.13 In horses with gastrointestinal disease but no apparent dehydration, administration of an electrolyte paste and provision of fresh drinking water may be sufficient to supplement water and electrolytes.14 However, enteral fluid therapy is contraindicated in horses with small intestinal obstruction or ileus and is not sufficient to treat hypovolemia.
Enteral fluids are often included in the treatment of impaction colic. Nasogastric administration of a balanced electrolyte solution (5.27 g NaCl + 0.37 g KCl + 3.78 g NaHCO3 per L water) at 5 L/h is superior to enteral administration of magnesium sulfate, sodium sulfate, or magnesium sulfate with IV crystalloids in promoting hydration of colonic contents, and
■ TABLE 32.11
Fluids and Additives for Electrolyte Disturbances in Horses
| Metabolic Disturbance | Recommended Fluid | Dosage |
| Lactic acidosis Hyponatremia • With hypochloremia | Polyionic crystalloids with or without small-volume resuscitation (HSS/HES) Isotonic crystalloids Polyionic crystalloids or sodium chloride | Up to 60 mL/kg/h Sodium level should be corrected no faster than 1 mEq/L/h |
| • Without hypochloremia | Sodium bicarbonate | |
| Hypernatremia Hypochloremia Hyperchloremia • With hypernatremia • Without hypernatremia Hypokalemia | 5% Dextrose or 2.5% dextrose/0.45% sodium chloride Polyionic crystalloids or sodium chloride Increased free water intake or administration Polyionic maintenance crystalloid or 5% dextrose Sodium bicarbonate Potassium chloride | Sodium level should be corrected no faster than 0.5 mEq/L/h 0.9% or 7.5%, to effect Sodium level should be lowered no faster than 0.5 mEq/L/h 5%, slowly, to effect 10 to 40 mEq/L or 0.5 mEq/kg/h Maximum 1 mEq/kg/h |
| Hyperkalemia | ||
| • With clinical signs • Potassium concentration >7 mEq/L • Without clinical signs Hypocalcemia Hypercalcemia Hypomagnesemia Hypermagnesemia Hypoalbuminemia | Calcium gluconate Sodium bicarbonate 5% Dextrose in polyionic crystalloids Calcium gluconate Polyionic crystalloids (without calcium) Magnesium sulfate Magnesium sulfate IV Calcium gluconate Fresh or fresh-frozen equine plasma HSS/HES | 1 mL/kg IV over 10 min 250 mL/1 L sodium chloride 1 to 2 mEq/L IV over 15 min 2 mL/kg IV over 5 min 250 to 500 mL of 23% solution/5 L 4 to 16 mg/kg as an initial dose 10 mL/5 L (maximum, 50 mg/kg) 4 to 16 mg/kg as an initial dose 250 to 500 mL of 23% solution To effect, not to exceed 10 mL/kg 5 to 10 mL/kg to increase COP |
All disturbances present must be taken into account before treatment begins.
COP, Colloid oncotic pressure; HSS/HES, hypertonic saline solution/hydroxyethyl starch solution (hetastarch); IV, intravenously; PO, by mouth.
it does not alter plasma electrolyte concentrations.15,16 An isotonic solution for enteral administration can be made without the use of weight scales by measuring salt crystals in the barrel of a syringe (15 mL of Lite salt and 15 mL of table salt added to 4 L of water).17 In a prospective clinical trial, 8 to 10 L of enteral fluids administered every 2 hours was successful in the treatment of 99% of colonic impactions and 83% of left-sided colon displacements.18 Because enteral fluids are significantly less costly than commercially available intravenous fluids, this is an ideal treatment in some gastrointestinal conditions.
■ Electrolyte Disturbances In many horses with gastrointestinal disturbances, plasma electrolyte concentrations are altered, which may need to be addressed during fluid therapy. Portable equipment for measuring blood gases and electrolytes allows the field veterinarian to easily obtain information necessary to guide electrolyte supplementation and selection of appropriate fluids. Without case-specific determination of electrolyte concentrations, maintenance phase fluids in gastrointestinal disease should be limited to administration of isotonic, polyionic crystalloid fluids supplemented with 10 to 20 mEq/L of potassium chloride.
Generalized changes in electrolytes among horses with gastrointestinal disease are related to decreased feed intake, increased loss, and sequestration. Decreased sodium and chloride concentrations may be observed in cases of acute colitis, peritonitis, or intestinal torsion.19 Hypochloremia without hyponatremia is also observed in proximal enteritis and grass sickness associated with loss of hydrochloric acid in gastric reflux.20 Hypokalemia is common in horses after colic surgery because of decreased feed intake, enhanced mineralocorticoid release, and kaliuresis associated with administration of sodium-containing fluids. Hypokalemia also occurs with colitis and metabolic alkalosis. Potassium is primarily an intracellular ion, and decreases in whole body potassium may not be detected through plasma measurements; therefore it is common to add supplemental potassium to maintenance fluids. Hypocalcemia is commonly observed in horses presenting with gastrointestinal disorders, including those with surgical colic, colitis, functional disorders of the small intestine, organic acidosis, and endotoxemia.21 Plasma ionized calcium provides a better indicator of physiologic calcium status, inasmuch as hypoalbuminemia occurs in many gastrointestinal conditions. In one report, 44% of horses with gastrointestinal disease had low plasma magnesium concentrations.22 Hypomagnesemia may be associated with refractory hypocalcemia and hypokalemia; thus supplemental magnesium may be beneficial in those situations. Hypophosphatemia has been reported in horses with strangulating intestinal lesions or intestinal ileus.
ACIDOSIS. Inorganic and organic metabolic acidoses occur frequently in horses with gastrointestinal disorders. Inorganic acidosis occurs with hyponatremia (colitis, peritonitis, intestinal torsion) and relative or absolute hyperchloremia (colitis, free water deficit). Many affected patients have a normal anion gap. Organic acidosis in horses with gastrointestinal disease is common, secondary to elevated lactate concentrations and associated with an increased anion gap. Increased blood or plasma lactate concentrations in these cases are usually a result of poor tissue perfusion or inappropriate anaerobic metabolism in endotoxemia.
Metabolic acidosis in horses with gastrointestinal disease usually resolves with correction of hypovolemia and restoration of tissue perfusion. In the case of inorganic acidosis, electrolyte abnormalities are occasionally severe enough to necessitate selection of a particular commercially available fluid. Administration of sodium bicarbonate to correct acidemia is reserved for cases in which the blood pH falls below 7.2 or for cases of severe hyponatremia with relative hyperchloremia, and only in patients with normal respiratory function.
Less frequently observed acid-base disorders in horses with gastrointestinal disorders include inorganic metabolic alkalosis (hypochloremia or hypoalbuminemia), respiratory alkalosis (hyperventilation associated with pain), and respiratory acidosis (hypoventilation caused by extreme abdominal distention or respiratory center depression).2
■ Hypoproteinemia Hypoalbuminemia occurs in horses with moderate to severe compromise of the colon, parasitism, intestinal malabsorption, or third spacing (peritonitis). Endotoxin exposure and ischemia-reperfusion injury induce capillary damage that allows plasma albumin to leak out into the interstitium. Clinical signs of hypoalbuminemia are peripheral, tissue, and organ edema, which lead to reduced oxygen uptake by cells and, in severe cases, organ failure. Albumin is a weak acid; thus severe hypoalbuminemia may contribute to metabolic alkalosis or mask concurrent metabolic acidosis.2 Determination of the colloid oncotic pressure (COP) of the plasma is most useful in guiding colloidal fluid therapy, particularly when synthetic colloids have previously been administered.23 COP and total protein concentrations were found to decrease over the course of anesthesia in horses undergoing colic surgery.24
Hypoalbuminemia and decreased COP should be treated when acute or if there are clinical signs. Options for colloidal support in horses include plasma transfusion and synthetic colloid solutions, such as hetastarch. Approximately 6 to 8 L of fresh-frozen plasma is necessary to effectively treat significant hypoproteinemia in adult horses, which makes plasma cost prohibitive in the treatment of decreased COP.25 However, plasma has a role in treatment of SIRS by providing AT-III and other cofactors. The administration of 6% hetastarch at 8 to 10 mL/kg to conscious hypoproteinemic horses significantly improved COP for 6 hours after infusion and maintained an oncotic effect for 24 hours; however, administration of 2.5 mL/ kg 6% hetastarch did not alleviate the decrease in COP observed in healthy horses receiving crystalloid during general anesthesia.26,27 Hetastarch should be used with caution in patients with conditions of decreased renal perfusion, systemic inflammation/ sepsis, or underlying renal insufficiency because it has been associated with development of acute kidney injury in humans.
■ Endotoxemia Horses with gastrointestinal disorders, particularly ischemic lesions and conditions involving inflammation of the bowel, are at risk of exposure to endotoxin as damage to the intestinal mucosa allows intraluminal bacteria to gain systemic access. During endotoxemia, capillary damage leads to increased vascular permeability, altering fluid dynamics and contributing to tissue edema. HSS has been shown to reduce the capillary endothelial swelling associated with SIRS and to improve tissue microcirculation and oxygen delivery.28
Studies of the effects of HSS in horses with experimentally induced endotoxemia have yielded mixed results. One study in conscious horses found that administration of 5 mL/kg HSS after administration of a low dose of endotoxin (1.64 ± 0.22 μg/ kg) improved cardiac output and decreased peripheral vascular resistance in comparison with isotonic saline.29 These findings were not supported by those of another study in anesthetized horses that received higher doses of endotoxin. In that second study, administration of combined 5 mL/kg HSS and 10 mL/ kg hetastarch to horses with hyperdynamic shock induced by administration of 50 μgZI(medial incisors) appears at 24 to 30 months of age. At 3 years of age, the third pair of incisors (lateral incisors) erupt. Between 3.5 and 4 years of age, the fourth pair of incisors (corner teeth) erupt.4,5 Consequently, cattle have a complete set of permanent teeth at 4 years of age. Cattle have a shallow alveolar socket and associated tooth root. This may lead to dental attrition more readily than in horses. The formula for the permanent teeth in cattle is as follows: 2(incisors 0/4, premolars 3/3, molars 3/3) = 32.
The deciduous and permanent dental formulas of the sheep and goat are identical to those of cattle.4 In sheep and goats, the periods of eruption are as follows: The incisors are present at birth or within the first 4 weeks. The premolars erupt 2 to 6 weeks after birth. The first pair of permanent central incisors replaces the deciduous pair at 12 to 18 months of age. The second pair erupts at 18 to 24 months of age; the third pair erupts at 30 to 36 months of age; and the fourth pair appears at 3.5 to 4 years of age. The three permanent premolars erupt at 18 and 24 months of age; the first molar, at 3 months of age; the second molar, at 9 to 12 months of age; and the last molar, at 18 to 24 months of age.4

FIG. 32.77 Photograph of a 2-year-old Holstein cow, with a Hau'Sman mouth gag in place to allow an oral examination. The cow was sedated with a “ketamine stun” (butorphanol, 0.05 mg/kg; xylazine, 0.025 mg/kg; ketamine, 0.1 mg/kg intramuscularly). The cow tolerated the gag and the examination well. (Courtesy Sylvain Nichols, Universite de Montreal.)
Examination of Teeth
Dental disease in ruminants should be considered first on a flock or herd basis.6,7 Determining dental health is particularly useful when unconventional feeds are incorporated into the herd nutritional program.8,9 The clinical manifestations of dental diseases include inadequate food intake, inadequate calf development, weight loss, unthriftiness, low body condition score, quidding, low pregnancy rate in replacement heifers, decreased milk production, and mandibular or maxillary swellings or draining tracts.4,7-10 Dental examination is especially of concern when animals are grazing on short grass. Examination of the herd should then be followed by dental examination of individual animals. For examination of the premolars and molars, the tongue should be withdrawn from the mouth and held at the commissure of the mouth opposite the teeth being examined. Use of a headlight or flashlight helps with performing a good oral examination. A small dose of xylazine (0.03 to 0.05 mg/ kg IV) or a “ketamine stun” (butorphanol 0.05 mg/kg, xylazine 0.025 mg/kg, ketamine 0.1 mg/kg IV) and the use of a mouth gag allows for much a more thorough dental examination, including manual palpation in cattle (Fig. 32.77). A rigid endoscope is useful for evaluating the crown and the occlusal surfaces of the cheek teeth. Radiographic examination can also be important in certain cases. Oblique views are mandatory to evaluate the roots of each cheek tooth completely.
The incisors have a sharp edge in front and are used for gripping and cutting herbage.4,7 The incisors should be aligned closely with little space between them.4,7 In sheep, the periodontium of the incisor allows a movement of up to 2 mm rostrocaudal to accommodate rotating or turning forces during grazing.10 This makes the sheep incisor very prone to loss after periodontal damage. The length of the premolar and molar teeth and their firm placement in the alveolar bone means that they are lost less often than the incisors.2,3,7