Fractures
Tamara M. Swor
Large animal fracture repair resulting in a successful outcome depends largely on a rapid and correct diagnosis, appropriate first-aid treatment and stabilization of the injured limb, and safe transportation to a referral surgical center.
Great advances in large animal orthopedic surgery and anesthesia have allowed successful treatment of several fracture types, but some injuries still retain a poor prognosis for survival. Emergency treatment and stabilization administered by a veterinarian in the field is crucial to preserve the most treatment options and enhance the prognosis. Accurate knowledge of viable surgical and medical possibilities, and the prognosis for various fracture types, is critical during discussions with clients. The referral surgeon should be contacted early in the process by the field veterinarian and involved in decisions regarding limb stabilization, transportation, and owner financial commitments. Various medical and surgical treatment options are discussed in this section; details of specific surgical principles related to fracture repair can be found in surgical textbooks.■ Definition and Etiology Afracture is defined as a break, crack, or rupture of a bone. In large animals, fractures are usually classified as complete or incomplete; articular or nonarticular; displaced or nondisplaced; open or closed; simple or comminuted; and transverse, oblique, or spiral. Classification by location is also common and includes terms such as physeal, metaphyseal, and diaphyseal.
Fractures in large animals are often associated with an acute traumatic event followed by sudden severe lameness. Horses may have a history of falling or running into a solid object, receiving a kick from another horse, being hit by a car, or flipping over backward (typically young animals). In another common scenario, the owner hears a loud pop or cracking sound while the horse is being lunged or is participating in an athletic activity.
Stress fractures also may occur and are often a result of cyclic loading over time, with corresponding fatigue leading to bone microfracture. Intensive training schedules create a high number of loading cycles with insufficient time to remodel and repair local areas of stressed bone (e.g., racehorse training). Specific locations of stress fractures include the distal end of the scapular spine, caudoproximal humeral head, craniodistomedial aspect of the humerus, medial humeral diaphysis, caudal aspect of the radius, dorsal mid-diaphyseal and distodorsolateral third metacarpal, caudal border of the ilial wing and adjacent to the pubic symphysis, proximolateral tibia, and caudal diaphysis of the tibia.1
Less common causes of large animal fractures include nutritional deficiencies, neoplasia, and infectious causes leading to pathologic fractures. Fractures related to difficult parturition events are seen in neonatal foals and calves.
■ ClinicalSignsandDifferentialDiagnosis An animal with a long bone fracture typically will present with an acute non-weight-bearing lameness of the affected limb. Moderate to severe soft tissue swelling and inability to control the limb often accompany other clinical signs of distress, agitation, shock, and pain. Because of the horse's “fight or flight” reaction to traumatic situations, the patient will often continue attempts to place weight on the fractured limb. Fractures in locations with limited soft tissue coverage are often open (e.g., third metacarpal). Severe hemorrhage or laceration of large vessels is uncommon but may occur (e.g., pelvis).
Complete catastrophic fractures are often easily identified based on limb instability and soft tissue trauma or swelling. Proximal limb fractures may be difficult to palpate but have adjacent severe soft tissue inflammation and edema, crepitus, and difficulties in limb function. Nondisplaced or incomplete fractures may be associated with a wound or may be painful to manual palpation.
Focal pain on palpation, a corresponding lameness, and a history of trauma or being kicked by another animal warrants radiographic evaluation in search of an incomplete fracture. An unrecognized incomplete fracture may progress to a complete fracture with time and movement or exercise. Physeal fractures should be considered in young animals.Stress fractures often present with a history of acute severe lameness followed by a rapid decrease in the degree of lameness. There may also be reports of intermittent lameness that improves with stall rest. Palpation of the limb often reveals a focal area of pain, heat, and/or swelling. The horse may resist manipulation and movement of the limb.
Differential diagnoses should include hoof and sole abscesses, joint subluxation, joint luxation, nerve damage, soft tissue injury, and septic synovial structures.
■ Clinical Evaluation A complete physical examination should be performed on initial evaluation. Animals that are not immediately identified as having a fractured limb may be in need of systemic support. Fluid therapy, pain control, antiinflammatory medications, and antimicrobials should be used as necessary.
Definitive diagnosis is made by taking multiple radiographic views; nuclear scintigraphy, ultrasonography, CT, and MRI may also be used (Figs. 38.37, 38.38, and 38.39). Information from imaging studies will provide fracture configuration details essential for determining prognosis. The bone involved, degree of comminution, articular involvement, physeal involvement, risk of infection, and condition of the bone fragments all affect potential repair attempts and long-term prognosis. Incomplete

FIG. 38.37 Lateral radiographic projection of middle phalanx fracture in the left hindlimb. Several fracture lines appear to be present. (Courtesy Dr. Dane Tatarniuk.)
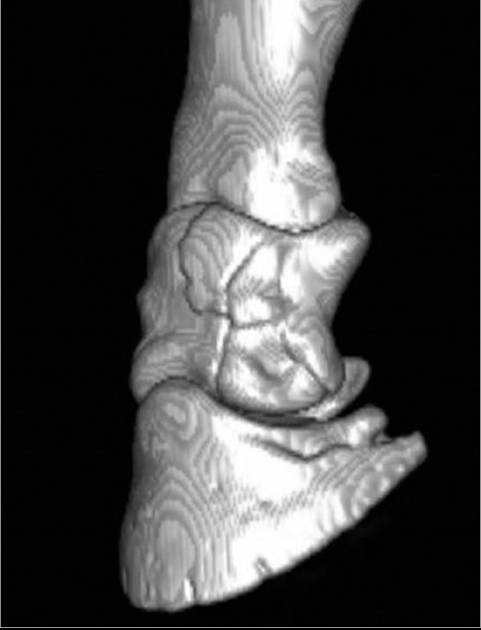
FIG.
38.39 Three-dimensional reconstruction of computed tomography images of middle phalanx fracture in the left hindlimb. This type of imaging allows the fracture to be assessed from all angles. (Courtesy Dr. Dane Tatarniuk.)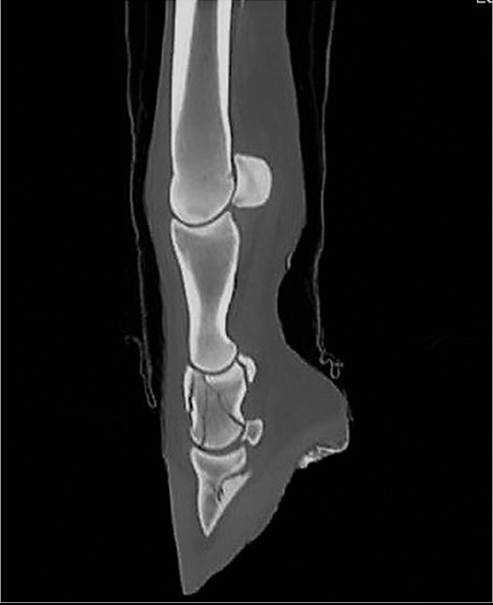
FIG. 38.38 Sagittal computed tomography image of middle phalanx fracture in the left hindlimb. Additional fracture lines are evident compared to those visualized on the radiographic projection in Fig. 38.37. (Courtesy Dr. Dane Tatarniuk.)
fractures may not be readily identified at the time of injury, and radiographs should be repeated in 10 to 14 days if a fracture is suspected.
Stress fractures are also commonly diagnosed using radiographic evaluation and may be identified as an incomplete cortical fracture, endosteal sclerosis, or periosteal callus.1 As with incomplete fractures, it may be difficult to identify a stress fracture by conventional radiography in the acute stages. Radiographs should be repeated in 10 to 14 days if a fracture is suspected. Other imaging modalities, especially nuclear scintigraphy or MRI/CT, may be useful in stress fracture identification.
■ Emergency Treatment The goals of emergency treatment include preventing further soft tissue damage, stabilizing the injured limb to decrease the patient's anxiety, minimizing further damage to the fractured bone ends, keeping the fracture closed, and preventing further injury and stretching to the surrounding vessels and nerves.2 A large animal with a fractured limb should be immediately restrained and calmed. Sedatives and tranquilizers should be used with caution, however, because the desired result may be difficult to achieve if the animal is agitated or in shock. The goal of sedation should be to allow manipulation of the limb and placement of external coaptation while keeping the animal standing. Common sedatives should be used with caution to avoid creating additional ataxia; butorphanol should not be used if the horse has sustained a front limb fracture because it will make the horse lean on the forehand.
If the animal is in systemic shock, an intravenous catheter should be placed and intravenous fluid support initiated. If a soft tissue wound is present, the veterinarian should assume■ TABLE 38.4
Emergency Splinting Techniques for Fractures in Large Domestic Animals
| Location | Species/Age | Splint |
| Distal phalanx Middle phalanx Proximal phalanx | Horses, foals Cattle, calves Horses, foals Horses, foals | No splint needed Bandage with dorsal (front limb) or plantar (rear limb) splint to proximal metacarpal/tarsal 3 and cast material, Kimzey splinta Bandage with dorsal (front limb) or plantar (rear limb) splint to proximal metacarpal/tarsal 3 and cast material, Kimzey splinta |
| Cattle, calves | No splint needed | |
| Distal sesamoid (navicular) Proximal sesamoids Metacarpal/tarsal 3 Metacarpal/tarsal 3 and 4 Metacarpal/tarsal 2 and 4 Olecranon/ulna Radius | Horses, foals Horses, foals Horses, foals Cattle, calves Horses, foals Horses, foals Horses, foals | No splint needed Bandage with dorsal (front limb) or plantar (rear limb) splint and cast material, Kimzey splinta Bandage with dorsal (front limb) or plantar (rear limb) splint and cast material, Kimzey splinta if fracture distal Bandage with dorsal (front limb) or plantar (hindlimb) splint and cast, cast No splint needed Robert Jones-type bandage with caudal splint to lock carpus in extension Robert Jones-type bandage with lateral splint to withers, second caudal splint if needed |
| Cattle calves | ||
| Humerus Scapula Tibia Femur | Horses, foals Cattle, calves Horses, foals Cattle, calves Horses, foals Horses foals | No splint needed No splint needed Robert Jones-type bandage with lateral splint to tuber coxae No splint needed |
| Cattle calves | ||
| Pelvis | Horses, foals Cattle, calves | No splint needed |
aLeg-Saver splint (Kimzey Inc., Woodland, Calif.).
that the fracture is open.
The wound should be cleaned, topical antimicrobials used, a bandage placed to prevent further contamination, and the animal started on systemic antimicrobials. Antiinflammatory medications (e.g., phenylbutazone) should be used as necessary. If the prognosis for survival is grave, euthanasia may be suggested to the owner and might be in the animal's best interest prior to attempting transportation.Appropriate external coaptation and stabilization of the fracture for transport can greatly influence the options available for fracture repair and the prognosis for success. Table 38.4 outlines specific emergency splints for different fractures in large animals.2,3 Splinting techniques are designed to be placed on the standing horse and attempt to neutralize forces acting on the fractured limb. Splints should be made of a strong, lightweight material like PVC pipe or wooden boards. Bandages over fractures should be placed tightly over the injured area to decrease soft tissue swelling and minimize slippage. A layer of cotton padding should be followed by a layer of gauze or a self-adhering bandage. Multiple layers can be placed if needed (e.g., Robert Jones-type bandage). A recent study suggested that bending forces were equally neutralized with a splint over a small bandage, compared to a Robert Jones-type bandage and splint.4 The splint should not end at the level of the fracture, should immobilize the joint above and below the fracture when possible, and should have enough padding so that no iatrogenic trauma occurs to the limb. In general, splinting techniques can be divided into categories based on fracture location.
DISTAL LIMB FRACTURES (PHALANGES, DISTAL METACARPUS/ METATARSUS). A light cotton bandage should be placed on the affected limb from the carpus to the ground. A splint is then positioned on the dorsal aspect of a forelimb or the plantar aspect of a hindlimb. The toe is pointed toward the ground to align the dorsal cortices and minimize stretching of the palmar/plantar vascular and nerve structures. A second splint should be placed on the medial or lateral side of the limb if any instability is present in those directions. The splint should be secured with inelastic tape. For additional stability, several rolls of fiberglass casting tape should be placed around the entire bandage and splint structure, incorporating the hoof into the cast.
MIDLIMB FRACTURES (MIDMETACARPUS TO DISTAL RADIUS, MIDMETATARSUS TO PROXIMAL METATARSUS). A Robert Jones-type bandage should be placed on the limb from the ground to the elbow in a forelimb or from the ground to the calcaneal tuber in a hindlimb. The bandage should be less extensive in the hindlimb to facilitate splint placement. In the forelimb, splints should be placed on the lateral and caudal aspects of the limb from the ground to the elbow. In the hindlimb, splints should be placed on the lateral and caudal aspects of the limb from the ground to the calcaneal tuber. The splints are secured using inelastic tape followed by several rolls of fiberglass casting tape around the entire structure.
UPPER LIMB FRACTURES (MIDDLE AND PROXIMAL RADIUS, TARSUS, TIBIA). A Robert Jones-type bandage should be placed on the limb from the ground and extend as far proximal as possible. In the forelimb, a splint should be placed on the lateral aspect of the limb from the ground to the withers. For increased stability, a second splint may be placed on the caudal or cranial side from the ground to the proximal forearm if necessary. Horses with olecranon fractures that disable the triceps muscle benefit from placement of a caudal splint to reestablish carpal extension. In the hindlimb, a splint should be placed on the lateral aspect from the ground to the tuber coxae. Splints placed high in this fashion will help minimize abduction of the limb.
HIGH LIMB FRACTURES (PROXIMAL TO ELBOW JOINT, FEMUR). Fractures in these locations are covered by extensive muscle, and attempts at splinting are usually unsuccessful and unhelpful to the animal. If triceps muscle function is disabled, a splint on the caudal aspect of the carpus, locking it into extension, is beneficial.
TRANSPORT. Transportation of adult horses or ruminants with long bone fractures can be difficult. They should be trailered in a manner that allows them to lean on dividers for support and be tied loosely to prevent them from turning around in the trailer but still be able to use their heads for balance. When possible, horses with forelimb fractures should be transported with the head facing the rear of the trailer, and those with hindlimb fractures should be transported with the head facing the front of the trailer. These positions allow the horse to control its weight most easily with the uninjured limbs during deceleration of the trailer. Foals and calves will often elect to lie down during transport and should be allowed to do so safely in a compartment next to the mare or cow.
■ Pathophysiology of Bone Healing Healing of a fracture terminates in the return of the injured bone to its original form. The process of fracture healing involves several biological steps that overlap and interact with each other. Typically, three phases are recognized: inflammatory, reparative, and remodeling.5,6 The acute inflammatory phase occurs in the initial 7 days after bone fracture, and chemical mediators cause chemotaxis, migration of leukocytes, and vasodilation to the injured area. These mediators protect the injury from infection and stimulate angiogenic factors. Cytokines from platelets aid in angiogenesis and mesenchymal cell growth.5 Granulocytes and macrophages destroy invading bacteria and stimulate cell repair through the release of growth and angiogenic factors. If the inflammatory phase is impaired, fracture healing may be compromised.5
The reparative phase overlaps with the inflammatory phase and may last for up to 12 months. This phase attempts to reestablish bone union. Interfragmentary stabilization by periosteal and endosteal callus formation begins if the fractured ends are not immobilized.6 Bony union develops as a result of endochondral and intramembranous ossification.5,6 In the reparative phase, interfragmentary motion may greatly influence fracture healing.
The remodeling phase takes place both during and after the reparative phase. Osteonal remodeling allows for replacement of necrotic regions of bone. When the bone is loaded, the negatively charged concave surface will attract osteoblasts to add new bone, and the positively charged convex surface will attract osteoclasts to remove bone.5,6 The result is the ability of a fractured bone to straighten itself by creating new bone formation on the concave surface and removing bone from the convex surface.
Repair of a fractured bone with the use of rigid internal fixation will inhibit naturally occurring callus formation and encourage bone to heal through haversian remodeling. Haversian remodeling requires that a fracture be rigidly fixed, have adequate reduction, and have an adequate blood supply.5,6 Haversian remodeling then functions to revascularize necrotic bone at the fragmented ends of the fracture and bridge interfragmentary gaps. This form of remodeling begins 2 to 3 months after injury.
Fractured bones are often described as healing by primary (direct) or secondary (indirect) intention.5,6 Primary bone healing occurs only with complete anatomic reduction and rigid stability. In large animal fracture repair, this is difficult to achieve because of the size of the animal and micromotion at the repair site. Secondary bone healing (most common in large animals) uses endosteal and periosteal callus formation, and new bone formed at the fracture site develops after initial formation of fibrous tissue or fibrocartilage.5,6
The rate of bone healing may be decreased if blood supply is inadequate, infection is present, soft tissue damage is extensive, or stability of the bone fragments is inadequate.
■ Treatment and Prognosis Treatment options for fractures in large animals include conservative therapy with stall rest and external coaptation (casts, splints), and surgical stabilization with open reduction and internal fixation. It is important to recognize incomplete and stress fractures and manage them appropriately with conservative therapy, preventing progression to a catastrophic fracture. In cases of incomplete fracture, the adult horse may need to be tied so that it does not cause additional stress to the fracture region by lying down and getting up repeatedly. The majority of fractures require some form of stabilization for the best chance of a successful outcome. Most horses require surgical stabilization for successful fracture repair. Ruminants are more amenable to successful fracture repair with nonsurgical options.
Conservative therapy with stall rest and external coaptation may be successful in some foals, calves, and small ruminants with complete nondisplaced fractures. Young animals have a greater and faster ability to heal bone in a reasonable amount of time, and their body weight is much less than that of a mature animal. In foals and calves, fracture configurations tend to be simpler, and the surgical implants available for repair are of a suitable strength for the animal's size. Unique complications in young animals include premature closure of physes with fractures in these areas, systemic and local infections related to failure of antibody passive transfer, and angular limb deformities from overuse of the contralateral limb. One report described treatment using external coaptation (modified Thomas splint-cast combination) in small equids (median 127 kg) successfully as a salvage procedure.7
Irreparable fractures are more common in adult animals because of the greater force required for bone breakage. Proximal limb fractures in adult horses often defy successful treatment because of the severe bone comminution that occurs and because available implants are not strong enough to support the bone until it is healed, adult horses are less likely to protect the limb than foals, and laminitis formation in the contralateral limb results in overuse of the repaired limb. Stall rest with external coaptation alone is rarely associated with a good outcome; most horses need some form of internal fixation for success. Horses are often required to be athletes, and fracture repair resulting in survival but not soundness may be unacceptable. In general, ruminants have a better prognosis for survival than horses because with their less excitable temperament they protect the limb better, and complete soundness is often unnecessary for a positive outcome. In ruminants, external fixation may be a more successful option than just external coaptation because it provides increased stability but costs less than internal fixation. Open fractures in horses greatly decrease the prognosis for survival and may delay the ability to perform internal fixation. In ruminants, open fractures are less common but also carry a poorer prognosis for survival.
Implants used for surgical open reduction and internal fixation methods vary based on the specific bone involved, the animal's age, the strength of the bone fragments used in the repair, and the surgeon's preference. Common implants used in large animals include intramedullary interlocking nails, dynamic compression plates (DCPs), locking compression plates (LCPs), limited-contact DCPs, screws, wires, pins, and dynamic condylar screw plates. Table 38.5 lists specific treatment options and prognoses.
■ TABLE 38.5
Treatment and Prognoses for Large Animal Fractures
| Fracture Location | Fracture Type | Treatment | Prognosis |
| Distal phalanx | Articular | Medical/surgical | Guarded |
| Nonarticular | Medical | Good | |
| Middle phalanx | Comminuted | Surgical | Guarded |
| Proximal phalanx | Comminuted | Surgical | Guarded |
| Noncomminuted | Medical/surgical | Good | |
| Distal sesamoid | Fragmented | Medical/surgical | Poor to guarded |
| Proximal sesamoids | Articular | Medical/surgical | Poor to guarded |
| Metacarpal/tarsal 3 | Nonarticular | Medical/surgical | Fair to good |
| Lateral condyle | Nondisplaced | Surgical | Good |
| Displaced | Surgical | Guarded | |
| Medial condyle | Articular | Surgical | Guarded |
| Diaphyseal | Comminuted | Surgical | Guarded |
| Metacarpal/tarsal 3 and 4 | Diaphyseal | Medical/surgical | Guarded to good |
| Metacarpal/tarsal 2 and 4 | Distal | Medical/surgical | Good to excellent |
| Proximal | Surgical | bgcolor=white>Guarded to good||
| Olecranon/ulna | Articular | Surgical | Good |
| Nonarticular | Medical/surgical | Good | |
| Radius | Complete | Surgical | Poor |
| Completea | Surgical | Guarded to good | |
| Incomplete | Medical | Good | |
| Humerus | Complete | Medical | Poor |
| Completea | Surgical | Guarded to good | |
| Scapula | Complete | Surgical | Poor to fair |
| Tibia | Complete | Surgical | Poor |
| Completea | Surgical | Guarded to good | |
| Femur | Complete | Medical | Poor |
| Completea | Surgical | Guarded to good | |
| Pelvis | Articular | Medical | Guarded |
| Nonarticular | Medical | Guarded to good |
aFoals, calves, and small ruminants.
SCAPULA. Fractures of the scapula occur most frequently in horses 2 years of age or younger and often involve the supraglenoid tubercle. Surgical removal of the fragment or repair using lag screws, tension band wires, or DCP/LCPs has resulted in limited success. Recently, distal femoral locking plates and transverse LCPs have been used with success in a small number of horses.8,9 Fractures involving the body of the scapula are often successfully managed conservatively in cattle.10
HUMERUS. The humeral fracture is often in a spiral or long oblique configuration. In ruminant and equine species, both conservative and surgical treatments have been used. In foals, surgical repair may include the use of intramedullary interlocking nails, DCP/LCPs, or intramedullary nails. Prognosis for a closed fracture in a foal is fair to good and depends on configuration, age, and weight.11,12 Humeral fractures in adult horses are not reparable at this time. Recent reports of horses with deltoid tuberosity or greater tubercle fractures of the humerus indicate some successful treatment results.13,14 Conservative treatment may be successful in adult horses with nondisplaced fractures and has been used in small ruminants and foals with acceptable outcomes. Ruminants have a better prognosis in general than equine species, and calves have been treated successfully using external fixation.15
RADIUS. The survival rate for ruminants with radial fractures repaired by external or internal fixation has been reported as 87.5%.16 Radial fractures in foals and young horses (casts or the Nunamaker external skeletal fixator.37 Fractures of the distal phalanx in horses may be successfully treated with surgical fixation, hoof casts, or modification in shoeing, depending on fracture configuration. One study found that 77% of horses had a successful outcome but did not find that immobilization of the hoof influenced results.38
SUMMARY. Animals identified as having incomplete fractures should be treated conservatively with stall rest and tied to prevent them from lying down if the fracture is at risk of becoming complete (e.g., radius). Animals with stress fractures should be treated conservatively with stall rest and a careful rehabilitation program, with ongoing radiographic evaluation.
Many fractures in large animals can be repaired and allow survival of the animal. Despite recent advances in orthopedic surgery and anesthesia, some fractures in large animals are still not able to be repaired. In general, prognosis for survival is improved if the animal is young, weighs 500 pounds (225 kg) or less, the fracture is closed, appropriate emergency stabilization is implemented quickly, and prompt reduction and internal stabilization are performed.