Spontaneous Fractures in Ruminants
Amanda K. Hartnack
■ Definition and Etiology Spontaneous fractures occur when a pathologic bone lesion weakens bone to the extent that fracture occurs secondary to normal forces.
These are also referred to as pathologic fractures. Causes include resorption of bone, reduction of bone mass, insufficient production of bone, or local bone destruction.■ Clinical Signs and Differential Diagnoses Clinical signs depend on the affected bones and may include lameness, swelling, postural changes, and angular limb deformity. Physical examination may reveal additional fractures. Commonly affected bones in ruminants include long bones, vertebrae, ribs, and mandible. Differential diagnoses include fractures of normal bones secondary to abnormal forces, septic arthritis or physitis, and osteomyelitis. Diagnosis is confirmed radiographically.
■ Pathophysiology, Epidemiology, and Clinical Pathology In ruminants, the underlying conditions that can lead to weakening of the bone's composite structure and subsequent fracture include bony destruction secondary to osteomyelitis or neoplasia, osteodystrophy associated with rickets in young animals, osteomalacia associated with nutritional imbalances in adults, and osteoporosis associated with copper deficiency.
Neoplasia and osteomyelitis weaken bone by dissolution of the mineral matrix, resulting in spontaneous fractures of affected bone. A variety of tumor types, including lymphosarcoma, hemangiosarcoma, liposarcoma, osteogenic sarcoma, and osteoma have been reported to cause spontaneous bone fractures in ruminants.1-5 Radiographically, lesions may have an osteolytic, osteoblastic, osteoporotic, or mixed appearance depending on the tumor or infectious agent involved.6,7 Localized bone infection can be traumatic or hematogenous in origin and may occur secondary to septic arthritis in calves.7 Reported cases include vertebral body abscessation, osteomyelitis of the sternum, distal sesamoid bone, mandible, and third phalanx.7-11 Trueperella pyogenes is the most common bacterial isolate,5,6 although osteomyelitis secondary to infection with Actinomyces bovis is also commonly reported in cattle.
Nutritional deficiencies or imbalances can lead to development of osteodystrophy, osteomalacia, and/or osteoporosis. These conditions can lead to spontaneous fracture, particularly of long bones and vertebrae, in some animals. Nutritional deficiencies can be classified as primary or secondary, with primary deficiencies involving inadequate intake and secondary deficiencies involving reduced nutrient absorption. Secondary deficiencies often occur when increased consumption of certain minerals such as iron, manganese, magnesium, zinc, sulfur, and molybdenum impede absorption of other nutrients. Clinically important bone diseases in ruminants are most commonly caused by deficiencies of minerals such as calcium, phosphorus, copper, and vitamin D (1,25-dihydroxycholecalciferol) due to their role in bone mineralization and collagen crosslinking.
In both young and adult animals, development of rickets due to phosphorus or vitamin D deficiency can occasionally result in spontaneous bone fracture.13 In young animals, rickets affects the developing skeleton, resulting in abnormal endochondral ossification and defective bone formation. In adults, the pathogenesis of osteomalacia-associated disease is similar, although only bone formed during remodeling is affected, and osteoporosis can also be seen.14 Clinical signs of phosphorus deficiency include loss of body condition, lameness, abnormal stance, spontaneous fractures, reproductive failure, and hypophosphatemia. Primary phosphorus deficiency can occur in ruminants when low levels of phosphorus are available in forage, and secondary phosphorus deficiency can result when significant imbalance exists between calcium and phosphorus concentrations in the ration.13 Serum phosphorus levels may not reflect the severity of the disease process.14,15 Gross postmortem findings may include brittle, porous bone and bony callus indicative of healed fractures on the ribs.
Copper deficiency has also been reported as a cause of osteoporosis leading to pathologic fracture in ruminants.16,17 Although copper deficiency may be caused by low copper levels in the diet (primary deficiency), it is more commonly a result of high dietary molybdemum or sulfur.
Deficiency occurs when molybdenum and sulfate form indigestible compounds called thiomolybdates, which bind copper.18 In addition to spontaneous fractures secondary to osteoporosis, clinical signs of copper deficiency include lameness, achromotrichia, diarrhea, anemia, and poor growth.19 In cattle, hepatic copper levels are considered the gold standard, with levels lower than 10 μg∕g commonly considered deficient. Low plasma copper (changes that race training induces, as the MCIII increases in size, density, and strength.3-5 Slower gaits or speeds result in tensile strains on the dorsal aspect of the MCIII.6 According to Wolff's law, the bone initially undergoes modeling and remodeling in response to these changes, resulting in periosteal fibrous bone on the dorsal cortices of the MCIII.5,7 At faster race speeds, the strain on the dorsal and dorsolateral MCIII rotate, becoming compressive instead of tensile.6,8 The bone, adapted for tensile forces, incurs microdamage that leads to pain, inflammation, lameness, and in some cases stress fracture.2,5■ Clinical Signs and Differential Diagnosis Dorsal metacarpal disease occurs in 2- and 3-year-olds that have recently begun race training, typically after the introduction of work at race speeds.6,7 History is important, as the disease rarely occurs in the nonracing horse and can occur in older racehorses that are changing training surfaces or beginning their career at a later age.2,9 Affected horses demonstrate inconsistent short-strided lameness, heat, and focal pain over the dorsal cortex of the metacarpus with or without swelling.2,9 Periosteal swelling can occur anywhere on the dorsal aspect of either limb, but generally both forelimbs or only the left MCIII demonstrate clinical signs.9,10 Lameness often resolves with rest and NSAIDs. The lameness can be ameliorated with local analgesia such as a high ring block over the proximal dorsal MCIII.
Radiographs at early onset may be inconclusive, whereas more chronic cases may have increased dorsal cortical thickness and linear lucencies parallel to the cortex (Fig. 38.40). Nuclear scintigraphic examination yields increased radionucleotide uptake on the dorsal cortex of the MCIII, which must be differentiated from normal uptake in an actively training horse.11 Dorsal cortical stress fracture of the MCIII has similar presenting signs as bucked shins. Initially there may be lameness after racing or speed work that subsides with rest. There may be focal pain on palpation with variable amounts of swelling or hard periosteal callus. Radiographic signs include periosteal and endosteal proliferation and a 30- to 45-degree oblique linear lucency in the dorsolateral cortex of MCIII, most obvious on the dorsomedial-palmarolateral oblique or
FIG. 38.40 Dorsomedial-palmarolateral oblique radiographic projection of the left third metacarpus on a 2-year-old Thoroughbred racehorse with chronically affected bucked shins. White arrows indicate periosteal bone proliferation. Black arrows indicate linear lucency parallel to the periosteal and endosteal surface.
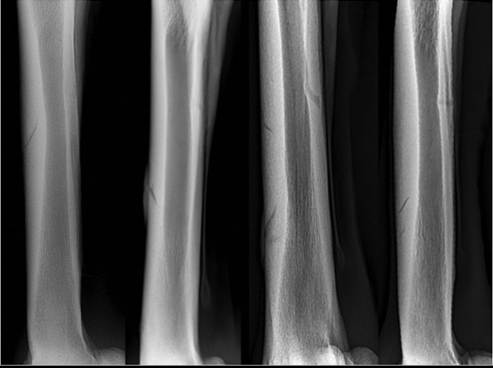
FIG. 38.41 Differing incomplete dorsal cortical stress fracture of third metacarpus configurations. From left to right, fracture line distal to proximal, proximal to distal, saucer type, and multiple fracture lines.
the lateral to medial projections.12 The fracture line can be oriented from the outer cortex, distal to proximal, proximal to distal, in a true saucer configuration, or on occasion more than one fracture can be present (Fig. 38.41). Nuclear scintigraphy of dorsal cortical stress fracture of the MCIII coincides with moderate to intense focal radionucleotide uptake.11
Differential diagnoses include trauma to the dorsal MCIII, exostoses of the second or fourth metatarsal bones, cellulitis, or osteomyelitis.
Signalment, a good history of the exercise program, careful physical examination, and radiographic evaluation can readily differentiate dorsal metacarpal disease from other causes of metacarpal swelling.■ Pathophysiology The musculoskeletal system of the 2-year-old racehorse undergoes significant changes in response to race training, with measurable changes in the size and geometry of the MCIII, compared to untrained horses.3,5,13 During training the dorsal cortex of MCIII undergoes fatigue, or repetitive loading, primarily in tension.2,6 Subsequently the bone adapts by modeling and remodeling, increasing the size of the MCΠI through fibrous periosteal bone deposition.2,6,7,14,15 As training continues with race speed work, the MCIII is subjected to compressive strains in a region adapted to tension, resulting in the clinical signs associated with dorsal metacarpal disease.2,5,6,16 The primary histologic lesions consist of focal remodeling and periosteal/endosteal bone proliferation with edema in the subcutaneous tissues.7 After resolution of the clinical signs of bucked shins, horses reenter training. Fibrous bone is weaker than lamellar bone, the dorsal MCIII is poorly adapted for compressive strains, and as with other fatigue fractures, microdamage accumulates under cyclic repetitive loading.14 Microdamage and microcrack formation occur faster than the ability of the skeletal system to repair the damage through remodeling.14,15 Microcracks increase in size, and macrocracks form and coalesce, leading to failure or dorsal cortical stress fracture.14,15
■ Epidemiology Dorsal metacarpal disease has been reported to affect up to 70% of juvenile Thoroughbreds at the start of training, 5% to 50% of Quarter Horses, and much less commonly the Standardbred.1,2,9,17 It has been estimated that between 10% and 12% of horses that develop bucked shins will develop a dorsal cortical stress fracture.2,9 Catastrophic failure of the diaphysis of the MCIII accounts for 10% of racetrack fatalities.2 Horses trained on softer surfaces have a delayed incidence of dorsal metacarpal disease.1,2,10 Standard- breds do not suffer from dorsal metacarpal disease nearly as frequently as Thoroughbreds, which may be related to gait and frequent training at race speeds.2 Differences in the mechanical properties of the MCIIIs of the two breeds were not observed in vitro.18 Dorsal cortical stress fractures occur primarily in 3-year-old Thoroughbred horses that have a history of bucked shins in their 2-year-old season.12,19
■ Treatment and Prognosis Treatment for dorsal metacarpal disease involves rest, antiinflammatories, and an altered training schedule.2,9 The rest period is contingent on resolution of the clinical signs of heat, pain, and swelling.
After clinical signs resolve, horses are slowly reintroduced to training. Based on previous research, the training schedule should be changed to incorporate more frequent, shorter, higher speed work and decreased galloping in an attempt to induce remodeling and adaptation of the MCIII for race speeds.2,20 If clinical signs return, horses are again rested and reevaluated, and training is altered again. Counterirritation (thermocautery, cryotherapy, blistering, and periosteal scraping) and infiltration with antiinflammatories or other products are often applied in conjunction with altered training, although the majority of evidence is from clinical experience, with a paucity of research on efficacy. Extracorporeal shockwave therapy in conjunction with a modulated training regime is also reported to have with a high success rate.21 There has been some concern that shockwave therapy will induce analgesia and mask pain, predisposing horses to fracture, although current research has not shown significant reduction in pain.21-24 Other therapies include local and systemic bisphosphonate therapy, although neither of the current products licensed for horses by the U.S. Food and Drug Administration are approved for animals under the age of 5 and therefore cannot be recommended. Although uncommon, if the horse fails to respond appropriately, it should be removed from training for a minimum of 60 days. Surgical intervention is the treatment of choice for mid-diaphyseal dorsal cortical stress fractures. Conservative therapy can be successful but may require a significant amount of time off, and the recurrence rate is thought to be high. Fractures that are very proximal or very distal on the MCIII do not require surgery and typically heal well. Surgical procedures described include cortical drilling (osteostixis), cortical drilling with12192526 unicortical position screw, or unicortical lag screw.12,,25, Fracture healing has been hypothesized to be promoted through the exposure of the damaged bone to medullary constituents, invoking the regional acceleratory phenomenon, or the induction of stress risers leading to osteonal repair.12,19,2',28 Drilling alone can be performed standing, as there have been some reports of catastrophic failure after general anesthesia with this technique.19 Methods involving screw placement performed standing require removal of the implant after 60 days.12,26 All procedures have a similar success rate of greater than 89%, and similar fracture recurrence rates of 4% to 9%.12,19,26 Screw placement techniques may yield a more predictable convalescence, although there have been no prospective comparative
12 studies to date.12
■ Prevention Current research has demonstrated that the biomechanical properties and structure of the MCIII in the young training racehorse are influenced by training method and that prevention of the disease is possible through alteration of classical training methods.2,5,10,20 Recommendations include jogging only for the purposes of warming up the horse, limiting long-distance sub-race speed gallops, and implementing more frequent short-distance breezes several times weekly.2 The full training program has been published and implemented with a lower incidence of dorsal metacarpal disease.2 Unfortunately,
many trainers are reluctant to alter their methods.29 Consequently, early identification and intervention are paramount in preventing poor performance and injury.30 Recently, a prospective study evaluating juvenile Thoroughbred horses found that prophylactic shin scraping, while it did not prevent dorsal metacarpal disease from occurring, decreased the incidence and significantly delayed the onset of bucked shins in treated horses.29 Future directions in decreasing the incidence of dorsal metacarpal disease should focus on the education and adoption of alternative training programs to allow the MCIII to adapt to racing speeds and pursuing interventions to lessen risk in classically trained horses.