Gait
Gait should be evaluated by moving the animal in a straight line, moving it in a tight circle, backing up, and moving it over obstacles such as a curb. Having the patient walk up and down a slope with varying steepness and with the head elevated may reveal subtler abnormalities.
The examination may need to be modified depending on the species of the patient, amenability to handling, and consideration of safety concerns.Quadrupeds begin walking by protracting the pelvic limb, followed by the thoracic limb of the same side, then the opposite pelvic limb, and finally the opposite thoracic limb. Gait on a level surface requires integrity of the musculature, motor and sensory components of the peripheral nerves, local spinal reflexes, ascending and descending pathways in the spinal cord, and centers within the brainstem. Dysfunction of ascending pathways (spinocerebellar tracts) results in mild to severe proprioceptive disturbances when standing or walking, which are exacerbated by turning the animal in a circle or stepping it on and off a curb. Animals with cerebral disease are usually able to perform simple motor activities such as walking along a straight path without obvious deficits but may exhibit decreased proprioception when they are required to perform complex motor activities such as walking on slopes or negotiating obstacles such as curbs or ground poles.
Subtle gait deficits may be elicited by walking and then trotting the patient or by walking or trotting the patient briskly and then stopping suddenly. While a helper is walking the animal in a straight line on a level surface, the examiner should take hold of the tail on the same side and pull the animal firmly to one side during the stance phase of the stride. The normal animal will move toward the pull but should not stumble or fall. If the tension on the tail is maintained, strength can be assessed.
Animals with lesions anywhere within the ascending or descending pathways controlling gait may be weak and/or show decreased proprioception in the form of stumbling, tripping, or crossing the limbs. The same test can be performed in the patient at rest. Resistance to lateral pressure at rest is provided by the antigravity myotatic reflex. Because this reflex uses peripheral nerves and spinal cord segments of the lumbosacral intumescence, inability to resist the tail-pull test at rest is suggestive of lower motor neuron (spinal cord gray matter, nerve roots, or peripheral nerves) of the L3 to S2 spinal cord segments on the side being tested. Circling the patient in a wide circle and then a tight circle also may elicit deficits, such as knuckling, stumbling, interference between feet, pivoting on one foot, or wide movements in the outside limb (circumduction), that are not observed when the animal is walked in a straight line. Assessment of gait is facilitated when animals are halterbroken and can be led. This is not the case in many ruminants, so the clinician must rely more on observing the animal in its usual environment or in a confined area such as a pen. A handler may drive animals that are not halterbroken, but this should be done with due consideration of animal and handler safety.A grading system for gait deficits has been described elsewhere,46 as follows:
Grade 0: Normal gait
Grade 1: Very subtle deficits, observed only by an experienced clinician
Grade 2: Deficits apparent to an inexperienced clinician Grade 3: Deficits apparent to laypersons
Grade 4: Severe deficits, including stumbling, knuckling at the fetlock, falling
Grade 5: Recumbency and inability to rise
Proprioception is the sense of body position in space. Proprioceptive information is collected by receptors in the skin, joints, muscles, and vestibular system. General proprioceptive pathways run mainly in the lateral (spinocerebellar) and dorsal (conscious perception) funiculi of the spinal cord, relaying information to centers in the brainstem, cerebellum, and cerebral cortex.
The vestibular system and pathways in the spinal cord to the vestibular centers in the medulla oblongata and cerebellum also help to control proprioception. Abnormalities of proprioception include stumbling, adduction or abduction of the limbs, circumduction, and interference between limbs (Fig. 8.2). Animals with proprioceptive deficits often slap down the feet hard, rather like the gait of a person walking down stairs in the dark, unsure of where the next step is. Walking the animal off a curb or step or down a slope exaggerates this appearance. When spun in a tight circle, normal animals lift the inside forefoot as the weight shifts. The outside rear leg is put down within a line demarcated by the lateral margin of the trunk. When spun in a tight circle, patients with abnormal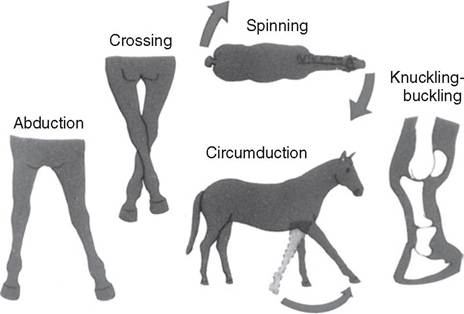
FIG. 8.2 Examples of conscious proprioceptive deficits in a horse. The signs of proprioceptive deficits in ruminants are similar.
proprioception may pivot on the inner hindfoot rather than lifting it and replacing it into a normal position. The outside foot may circumduct widely, knuckle, or buckle, and the inside foot may step on the outside foot. Animals with abnormal proprioception worsen when they are required to climb hills or lift the foot over a curb or are walked with the head elevated. The gait of noncompliant cattle may be assessed by observation of maneuvers through corrals, alleys, or a squeeze chute.
Having the animal walk backward also tests proprioception. The normal subject should be able to do so in a smooth, coordinated fashion, with conjugate movement of diagonally opposite limbs. Animals with lesions of upper motor neurons in the descending motor pathways may exhibit abnormalities such as foot dragging and weakness, sometimes to the point of “dog-sitting”; others may be reluctant to move straight backward and will try avoidance maneuvers such as circling to one side or the other to avoid it.
Such tactics should raise the index of suspicion of a neurologic deficit. Care should be taken when backing an animal with severe neurologic deficits because some animals could fall backward during the procedure. Animals that are uncooperative or that have been little handled may exhibit a reluctance to walk backward that is not caused by neurologic disease. Observing the patient's general level of cooperation and having a behavioral history will help the examiner determine whether the problem is caused by neurologic disease or the animal's lack of compliance.Cerebellar disease causes errors in the rate, range, and force of voluntary movements; there is generalized ataxia with a rolling, drunken gait. Protraction of the limbs is delayed and limb movements are exaggerated, characterized either by excessive flexion during protraction, a condition known as hypermetria, or by hypometria, characterized by reduced joint flexion. There are often coarse bobbing movements of the head when the patient is walking; an intention tremor (most notable in the head) occurs when the animal initiates purposeful movements, such as reaching out to take food. Intention tremors may disappear when the animal is relaxed or recumbent. Cerebellar diseases may also result in opisthotonos or seizure-like fits.
Spontaneous circling is seen in diseases of the vestibular system and forebrain. Circling varies from a mild tendency to move in one direction to spinning and staggering in tight circles. Circling most often occurs toward the side of the lesion, except in paradoxical vestibular disease (caused by lesions in the vestibular components of the cerebellum) and with some asymmetric forebrain lesions, in which the animal circles away from the side of the lesion. Localization of the neurologic lesion in animals that circle is made based on other neurologic abnormalities such as dementia, seizures, central blindness (forebrain disease) or proprioceptive deficits, head
tilt, spontaneous nystagmus, obtundation, and other cranial nerve deficits (vestibular disease).