Gallbladder and Biliary Tract Disease
Jennifer L. Davis
Biliary tract disease in large animal medicine is rare and results from both intrahepatic and extrahepatic causes. Intrahepatic causes of cholestasis include cholangitis, cholecystitis, cho- ledocholithiasis, and presence of a foreign body.
Extrahepatic causes include abscess formation, obstructive or inflammatory intestinal disease, and neoplasia.Choledocholithiasis, Cholelithiasis, and Hepatolithiasis
By definition, cholelithiasis describes the presence of biliary calculi in either the bile ducts or the gallbladder, whereas Choledocholithiasis describes stones found in the common bile duct. Hepatolithiasis indicates the presence of calculi in the intrahepatic bile ducts above the right and left hepatic ducts and is a variation of cholelithiasis. These conditions have been described in horses, cattle, sheep, and pigs, but they do not seem to be recognized as a clinical problem in sheep, and rarely in cattle.1-15 Choledocholithiasis is the most common cause of biliary obstruction in large animals and occurs more frequently in horses.1-9
Biliary stone formation begins with precipitation or aggregation of normally soluble components of bile. Other mechanisms involved in the pathogenesis include ascariasis, ascending biliary infection or inflammation, biliary stasis, changes in bile composition, and presence of a foreign body.14 Several pathogenic bacteria (Salmonella spp., E. coli, Aeromonas spp., Citrobacter spp., group D Streptococcus spp., Clostridium perfringens) have been cultured from the bile ducts of horses and cows with cholelithiasis.2,6,9,16 Whether these bacteria were the cause or the result of the stone formation remains unclear. In most reports the chemical analysis has shown that choleliths have a mixed composition, containing bilirubin, bile pigments, cholesterol esters, esters of cholic and carboxylic acid, calcium phosphate, and sodium taurodeoxycholate.6,8,9 In one study, 80% of the choleliths contained less than 10% cholesterol.9
Cholelithiasis should be suspected in horses when a triad of clinical signs exists: recurrent abdominal pain, intermittent pyrexia, and icterus.
Hyperammonemic hepatic encephalopathy, photosensitization, and weight loss are other, less common features of cholelithiasis.3,5,6,14,16 A subclinical presentation due to partial obstruction of the biliary tree may be recognized only on postmortem examination.11 A large cholelith was the cause of duodenal obstruction in a horse presented for colic.12Elevations in the serum activity of ALP, AST, GGT, SDH, and total bilirubin are associated with cholelithiasis.3,6,9,14,16 The rise in total bilirubin is due to an elevation in both direct and indirect bilirubin. Serum bile acid concentrations also increase when bile flow is obstructed. Other laboratory abnormalities that may be seen include hyperammonemia, increased urine bilirubin, and prolonged partial thromboplastin and thrombin times.5,6,9 The most common alterations in the leukogram include a neutrophilic leukocytosis. Elevations in globulin and fibrinogen may also occur.5
Ultrasound examination of the liver is a safe, noninvasive tool for diagnosing cholelithiasis. Hepatomegaly and bile duct dilation are seen in horses with biliary calculi. The echogenicity of the hepatic parenchyma is increased compared with that of normal horses and may approach that of the spleen. The bile ducts are thick and distended. The parallel channel sign (dilation of interhepatic biliary radicals adjacent to the portal vein) may also be seen. Several choleliths are generally seen, but a single stone may be present (Fig. 33.12). Choleliths may be hyper- echoic, casting acoustic shadows, or they may be sonolucent. Choleliths are most likely to be visualized in the cranioventral part of the right hepatic lobe, especially in the sixth to eighth intercostal spaces. Cholelithiasis can be diagnosed accurately by ultrasound in at least 75% of horses if an adequate scanning image of the liver is obtained and bile duct dilation and choleliths are visualized.8
The differential diagnosis for a horse with the clinical signs associated with cholelithiasis include other causes of liver disease and mild recurrent abdominal discomfort, including verminous arteritis, mesenteric abscesses, sand enteropathy, enterolithiasis, abdominal neoplasia, and urolithiasis.3
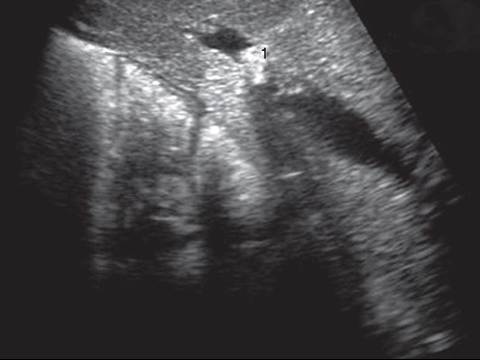
FIG.
33.12 Ultrasound image of a cholelith taken from the right side of a horse. Note the hyperechoic stone (1) visible inside a distended bile duct. Hyperechoic parenchyma is also noted beneath the stone, which may represent hepatic fibrosis.

FIG. 33.13 Multiple choleliths present with the bile ducts of a horse.
Hepatomegaly is usually noted at necropsy, although a shrunken liver may be observed. The liver is firmer than normal, has a consistent texture, and varies in color from red to greenbrown. The hepatic ducts and common bile duct are generally dilated and may contain the calculi (Fig. 33.13). Histologically, periportal fibrosis is a common finding. Bile duct stasis and hyperplasia are usually noted; suppurative cholangitis is less common.9’14’10
Treatment of cholelithiasis initially includes broad-spectrum IV antibiotics (penicillin plus gentamicin or enrofloxacin) and oral metronidazole. This is followed by long-term oral antibiotics, based on culture and sensitivity of a biopsy specimen, if available. If culture and sensitivity results are not available, treatment should be aimed at suspected gram-negative enteric bacteria or anaerobes. Potentiated sulfonamides or enrofloxacin plus metronidazole are good choices. Chloramphenicol has a good spectrum against most cultured bacteria, but since it is highly metabolized by the liver, it should not be used if hepatic function is severely compromised. Antibiotic treatment should continue for 0 weeks past the time when GGT values return to normal. DMSO (0.5 to 1 g/kg IV as enteritis, right dorsal displacement of the large colon, and less frequently, left dorsal displacement of the large colon.22-24 Duodenal strictures secondary to severe gastroduodenal ulceration have also been reported as a cause. Clinical signs associated with cholangitis and cholangiohepatitis in the horse may include anorexia, pyrexia, subtle behavioral changes, chronic weight loss, colic, and icterus. Septic peritonitis may occur as an extension of bacterial infection into the intraperitoneal space.25 Alterations in hepatic enzyme activity may indicate hepatocellular damage, cholestasis, or both. Histopathologic examination and bacterial culture are indicated to further identify the causative agent. In cases of suspected bacterial etiology, long-term antibiotic therapy is indicated.25 Antibiotic choice should be based on bacterial sensitivity, but in cases where no bacterial organism is identified, an antibiotic that is effective against enteric organisms and secreted or cleared in the bile is warranted.