Guttural Pouch Mycosis
Robert J. MacKay
■ Definition and Etiology The clinical signs occur because fungi invade vital vascular and neural structures in the roof of one, or occasionally both, guttural pouches.
There is no apparent age, sex, breed, or geographic predisposition to this disease.1 Foals as young as 3 months of age have been affected.2 Aspergillus fumigatus and Emericella nidulans (the sexual form of Aspergillus nidulans) are the fungi most commonly identified in pure or mixed culture.3,4 Lesions are typically diphtheritic membranes of variable size, composed of necrotic tissue, cell debris, a variety of bacteria, and fungal mycelium (Fig. 35.15).1The guttural pouch is partially separated into two compartments by the stylohyoid bone and occipitohyoideus muscle. Cranial nerves IX through XII, the cranial cervical ganglion and postganglionic sympathetic nerve, and the internal carotid artery are located in a fold that traverses the dorsomedial aspect of the medial compartment. For unknown reasons, this site is susceptible to colonization and destruction by invasive mycotic infections.5 In approximately one third of cases, the fungal lesion is located in the lateral compartment, sometimes after extension from a primary site in the medial compartment.1 At this location, the fungal mycelium may invade the wall of the external carotid artery or any of its branches and affect the facial nerve (VII). Facial nerve paralysis has also been observed as a result of direct invasion by a fungal guttural pouch infection into the overlying parotid lymph node and salivary gland.6 Fungal plaques may also spread from one guttural pouch to the other by eroding through the apposed medial walls of the pouches.
■ ClinicalSigns Initial signs are headshaking and unilateral nasal discharge.
There is a tendency to hold the head in extension or lower to the ground than normal. Additional clinical signs are nasal discharge, dysphagia with nasal return of feed-stained saliva, head shyness, stridor, dysphonia, protrusion of the tongue from the mouth, and epistaxis.6,7 Epistaxis may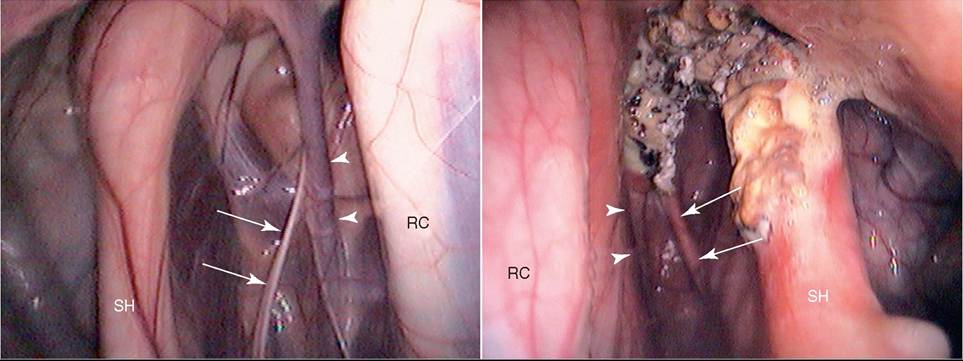
FIG. 35.15 Endoscopic views of the caudal aspects of the left guttural pouch with a mycotic plaque over the neurovascular structures of the medial compartment of left guttural pouch (right) and normal right guttural pouch (left). There is also thickening of the left stylohyoid bone secondary to temporohyoid osteoarthropathy. Arrows point to the glossopharyngeal nerves, and arrowheads point to the internal carotid arteries. RC, Rectus capitis ventralis major muscle; SH, stylohyoid bone.
be bright red, high volume, and life-threatening. Other clinical signs include sensitivity to pressure over the parotid salivary gland, Horner syndrome (sweating, miosis, and ptosis on the side of the lesion), paralysis of the tongue on the affected side, and facial paralysis.6-10 Atrophy of the brachiocephalicus and trapezius muscles secondary to denervation of the spinal accessory nerve (XI) has been described in a few cases. Horner syndrome is a development secondary to damage of the cranial cervical ganglion and postganglionic fibers. The sensorium is intact unless aspiration pneumonia develops or the fungus spreads into the brain.11,12 Affected horses may die peracutely as a result of exsanguination from ruptured internal or external carotid arteries or their branches. Endoscopic examination of the larynx of affected horses may reveal dorsal displacement of the soft palate, inability to swallow, and laryngeal hemiplegia. Mycotic guttural pouch infection can be diagnosed definitively endoscopically by identifying the characteristic fungal mass in the caudodorsal aspect, usually of the medial compartment.
Radiographic examination of the pouches shows a poorly defined border of the pouch in the abnormal area.■ Treatment Before the onset of neurologic signs, the affected artery or arteries may be occluded on each side of the lesion by ligation/balloon-tipped catheter, embolization coils, or nitinol plugs. Occlusion of the ipsilateral common carotid artery alone does not prevent fatal hemorrhage.13 Complete arterial occlusion prevents fatal epistaxis, but it is not clear whether it affects fungal growth. Some studies have shown excellent, albeit delayed, rates of resolution of mycotic lesions in horses that underwent the procedure with or without additional antifungal therapy,14,15 but in other animals the lesion may progress despite complete arterial occlusion. Because some such lesions resolve spontaneously over time, the role of surgery in their resolution remains controversial.1 Optic neuropathy and blindness of the ipsilateral eye are occasional sequelae of occlusion of the external carotid artery and its branches.1 Lesions may be treated topically through an endoscope with povidone-iodine or triazole antifungal agents such as enilconazole, voriconazole, and itraconazole. Itraconazole is also affordable and safe when administered systemically. Nystatin, natamycin, miconazole, and fluconazole have little activity against Aspergillus/Emericella spp. Amphotericin B is effective, although systemic treatment is limited by its toxicity. Topical treatment may be repeated daily (or as frequently as is practicable) for up to several weeks. As the fungal mass degenerates, pieces can be carefully removed endoscopically with biopsy forceps in horses that have previously undergone arterial occlusion. Dysphagic horses may be fed via an indwelling esophagostomy tube while lesions are being treated. Neurologic signs may be permanent, although improvement or recovery over many months has been reported in some horses.
Affected horses are often euthanized for humane reasons. (See Chapter 31 for more on treatment of guttural pouch mycosis.)Listeriosis (Circling Disease; Silage Disease; Listeria monocytogenes Infection) feces of a large percentage of normal animals.7 It is unclear whether this high rate of asymptomatic carriage represents a true carrier state or is simply the result of a high environmental contamination by nonpathogenic isolates.7 The agent infects the udder but rarely causes clinical mastitis. In sheep, excretion of the bacterium in the milk is greatest during the immediate postlambing period.8,9
L. monocytogenes can survive for long periods in the environment and in carriers with no symptoms. Ihe bacterium can multiply at low environmental temperatures and is resistant to environmental influences. L. monocytogenes is shed in the feces of carriers with no symptoms, especially at the end of pregnancy and at lambing. Once in the environment, the bacterium can survive for 2 years in dry soil. It is resistant to freezing and thawing in the soil, but it does not survive for more than 1 to 2 weeks in properly preserved silage. The bacterium proliferates in rotting vegetation in which aerobic conditions exist and the pH is above 5.4.10-12 Common sources of contamination in forage include spoiled silage at the ends of trench silos, decaying forage at the bottom of feed bunks, or rotting hay at the periphery of hay stacks.10,13 The incidence of listeriosis may be increasing because of the greater use of trench silos and bulk handling methods, in which the amount of spoilage is greater than in conventional upright silos. Although L. monocytogenes can be isolated from silage with a pH below 4, fewer bacteria are found in well-preserved forage.14
A selective enrichment medium has been developed for identifying and enumerating the Listeria organisms in silage. This medium enables semiquantitative enumeration of Listeria bacteria in 10 g of silage.
Hemolysin production is measured by overlaying the colonies with bovine blood agar and reincubating the plates. With this method, outbreaks of listeriosis have been correlated with silage containing 1 million Listeria organisms and more than 1 million enterobacteria per gram of silage. The pH of such silage characteristically exceeds 7.8.15There is a significant public health concern about Listeria contamination of milk products. The 4b serotype of L. monocytogenes is most often responsible for infections in humans.16 z~x 1111 1 ∙ ∙ C "1
Outbreaks have been traced to ingestion of unpasteurized milk, cole slaw, and soft, ripened cheese. Foodborne listeriosis outbreaks have also been linked to contaminated fruit and vegetables.
■ Pathogenesis Listeria organisms produce a hemolysin, listeriolysin-O, which is a thiol-activated toxin (molecular weight, 58 kD) that, in certain amounts, produces disease. The molecular role of the toxin in dissemination of the infection and in cell death is not known.
It is unclear whether infection of the brain by L. monocytogenes occurs hematogenously or by ascent from the cranial nerve rootlets.17 Morphologic studies of naturally occurring cases of encephalitic listeriosis have demonstrated the bacterium in the axons of the trigeminal nerve rootlets, which indicates possible centripetal migration.17,18 Similar findings have been reported in animals infected experimentally.19 Younger animals may be susceptible because eruption of the permanent teeth may expose trigeminal nerve rootlets. Lsteriosis has been experimentally induced by inoculation of the bacterium into the pulp cavity of sheep.20 Infection of the CNS without bacteremia has been detected, which also indicates that centripetal migration of the bacterium is possible.21 Some investigators consider axonal migration as an unlikely mode of pathogenesis because L. monocytogenes is not nutritionally dependent on nervous tissue and because of the ready ability to produce multifocal brain microabscesses by intravenous inoculation of the bacteria into susceptible hosts.17,22
■ Clinical Signs The neurologic signs of listeriosis in adults reflect dysfunction of the caudal brainstem, cerebellar peduncles, or spinal cord.5 Fever may be present early in the clinical course, and poor appetite and depression are common.
CNS signs are usually asymmetric and include conscious proprioceptive deficits, head pressing, and cranial nerve deficits. Depressed consciousness is the result of lesions of the reticular activating system. Conscious proprioceptive deficits are caused by interference with the descending motor pathways and the ascending proprioceptive fibers in the brainstem and may precede or accompany cranial nerve dysfunction. Head pressing and propulsive walking or compulsive circling are caused by lesions of the basal ganglia. Severely affected animals may be recumbent and may display torticollis, head tilt, or other unilateral vestibular signs.Cranial nerves V through XII are usually dysfunctional in listeric animals. Patients with loss of the trigeminal nerve (cranial nerve V) show dropped jaw or asymmetric jaw closure and facial analgesia or anesthesia. Facial analgesia is best detected by stimulation of the nasal septum with a pencil or piece of straw. Animals with lesions of cranial nerve VI exhibit a medial strabismus on the ipsilateral side of the lesion. Animals with lesions of cranial nerve VII have ptosis, loss of menace response, no palpebral reflex, drooped ear, loss of levator nasolabialis muscle function, and decreased lip tone (Fig. 35.16). Small ruminants with cranial nerve VII loss have a deviated philtrum. The paralysis of the orbicularis oculi muscle results in exposure keratitis.23 The loss of levator nasolabialis function is best detected by observation of the muscular contraction on the dorsum of the nose during inspiration. Loss of lip and cheek muscle tone is best detected by observation of drooling from the ipsilateral side of the mouth and by palpation of the lips and nostrils.
Animals with cranial nerve VIII lesions display nystagmus that changes as the position of the head is altered. Other signs include a head tilt toward the side of the lesion and a tendency to circle or fall to the lesion side. The nystagmus may be horizontal, vertical, or rotatory and is usually inconstant. If the spinal reflexes can be tested, the affected animals show a
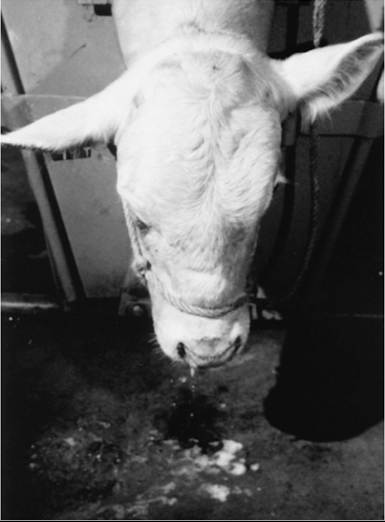
FIG. 35.16 Clinical appearance of the neurologic form of listeriosis in a Charolais bull. Note the drooped right eye and ear and the drooling from the right side of the mouth. (Courtesy Dr. WD. Wilson.)
mild to moderate hypertonia and hyperreflexia in the limbs opposite the side of the lesion. Animals with acute loss of cranial nerves IX, X, and XII develop stertorous breathing and dysphagia. Animals with dysfunctional cranial nerve XII have paresis or paralysis of the tongue. With unilateral lesions, the tongue protrudes from the side of the mouth ipsilateral to the lesion. Progression of listeriosis is associated with decreased consciousness, coma, and convulsions.
Lambs may selectively develop spinal myelitis without brainstem disease. This condition results in flaccid paraparesis or hemiparesis without attendant signs of brainstem dysfunction.24 The clinical signs of myelitis include tetraparesis, tetraplegia, paraparesis, paraplegia, conscious proprioceptive deficits, and recumbency. The sensorium and appetite are normal in some affected animals and greatly depressed in others.25 Primary ocular disease caused by L. monocytogenes, manifesting as keratitis, conjunctivitis, or uveitis, may occur in cattle or horses with no signs of neurologic disease.26
■ Clinical Pathology Examination of the CSF usually helps confirm a diagnosis of listeriosis, but the cell and protein concentrations of the specimens are not necessarily correlated with the severity of the clinical signs or prognosis. The protein concentration in the CSF may exceed 40 Pg/dL, and WBC counts in the CSF may exceed 12 cells/pL with mononuclear pleocytosis.1,27,28 Many cattle with advanced signs of listeriosis develop metabolic acidosis as a result of salivary bicarbonate loss.
■ Pathology Pathologic confirmation of listeriosis is based on identification of multifocal microabscesses in the brainstem and isolation of L. monocytogenes from infected brain tissue. The agent is only rarely isolated from CSF and is best recovered from refrigerated nervous tissues. Enrichment of the Listeria organisms may be accomplished by refrigerating slices of brain at 4° C (39.1° F) for 3 months while the tissues are cultured weekly. In contrast to septicemic listeriosis of monogastric animals, peripheral monocytosis is not observed in infected ruminants.
■ Pathology The lesions of listerial meningoencephalitis are most common in the pons and trapezoid bodies, but they can be located anywhere in the brainstem. Neurologic structures most often affected include the reticular formation and cranial nerves V and VII to X. Macroscopic lesions are limited to mild meningeal congestion and clouding of the CSF. Microscopic lesions include perivascular cuffing with mononuclear cells, multifocal asymmetric brainstem microabscesses, and mononuclear cell meningoencephalitis.16 The microabscesses are composed predominantly of neutrophils. Other microscopic changes include degeneration of the neuropil and neuronophagia.
■ Treatment and Control The recovery rate is best if treatment is administered early in the disease course. Animals that are recumbent, comatose, or convulsive rarely survive despite intensive antibiotic and supportive therapy. In most cases, treatment must be administered for a prolonged period because recovery may take as long as 1 month. L. monocytogenes is susceptible to most of the common antimicrobial drugs. Recommended treatment is either oxytetracycline, 10 mg/kg IV twice daily, or therapy with penicillin G.23 Specific recommendations for penicillin therapy include an initial dosage of 40,000 IU/kg (potassium penicillin G) IV three or four times daily for 7 days and then 22,000 IU/kg (procaine penicillin) IM once daily for 14 to 21 additional days.23
The plasma concentrations of bicarbonate and potassium should be measured, and specific corrective fluid therapy should be administered as indicated by acid-base and electrolyte assays. Good footing and nursing care are also beneficial.
Serologic responses to flagellin and listeriolysin-O develop after oral administration of virulent L. monocytogenes and confer 21
protection against listerial bacteremia.21 Vaccines of attenuated or killed bacteria have been used successfully to protect sheep and goats. Although these vaccines reduce the incidence of listeriosis in vaccinated flocks, they are not commercially available in the United States.
Although the case attack rate of listeriosis is low, occasional epizootics may occur in cattle, sheep, or goat herds, invariably in association with high rates of environmental contamination. In such cases, the hay and silage should be cultured for L. monocytogenes. Rotten vegetation should be discarded, and cattle should be fenced from contaminated areas.
Thromboembolic Meningoencephalitis (Histophilus somni Infection;
Sleeper Calves)
■ Definition and Etiology Thromboembolic meningoencephalitis (TEME) is a fulminant neurologic disease of cattle that arises from septicemia caused by the pleomorphic, nonencapsulated, Gram-negative bacterium H. somni (formerly Haemophilus somnus).i Because it can disseminate via the bloodstream, this organism can incite infection in multiple organs. In addition to TEME, H. somni can cause pleuropneumonia, myocarditis, laryngeal abscesses, polyarthritis, polyserositis, and infections of the ear, eye, udder and urogenital tract.1-6
■ Epidemiology Although TEME occurs most frequently in feedlot cattle,7 outbreaks in the western United States and Canada have been reported in both pasture and dry lot environments.8,9 In a serologic study of feedlot cattle, seroconversion to H. somni occurred early in the feeding period (soon after placement).10 This may be reflective of the role of stressors (e.g., comingling of animals from different sources, transport, or changes in feed) in the pathogenesis of this disease. Chapter 31 includes further details on the epidemiology of H. somni infections in cattle.
■ Pathogenesis Infection of cattle by H. somni probably occurs through the respiratory tract. Bacterial proliferation in the lungs and other soft tissues by serum-resistant isolates results in bacteremia. Histophilus possesses multiple virulence factors including the capability to induce apoptosis of endothelial cells.6 Exposure of subendothelial collagen occurs subsequently, which results in microthrombus formation and organ damage through hypoxia and inflammation. The sites of the body most affected by the thrombosis are the brainstem, spinal cord, synovial membranes, pleura, and lungs. Although the name thromboembolic meningoencephalitis implies the passage of solid material in the vasculature to a downstream occlusion site (embolism), thrombus formation probably occurs directly at the site of the vascular lesion.
■ Clinical Signs Only the neurologic syndrome (TEME) is discussed here. Descriptions of other clinical syndromes of H. somni infection are discussed in Chapters 31, 39, and 43. The initial signs of TEME are fever (40° C to 41.6° C [104° F to 107° F]), anorexia, depression, and ataxia.7,8,11, In addition to depression, affected animals show a number of conscious proprioceptive deficits, including knuckling, circumduction, crossing over, and interference. Affected animals may fall while attempting to walk. Signs specifically associated with lesions of the cerebellum and caudal brainstem include head tilt, nystagmus, strabismus, blindness, muscular tremors, opisthotonos, coma, and convulsions.12 Signs of infection in other organ systems (e.g., pneumonia, arthritis) may be present in the affected animal or in cohorts. Death may occur within 36 hours after the onset of neurologic signs.
■ Clinical Pathology Examination of CSF may be helpful in substantiating a clinical diagnosis of TEME. Specific CSF changes characteristic of hemorrhage include high erythrocyte counts, xanthochromia, and increased concentrations of protein (>100 mg/dL) and neutrophils (>500 WBCsZμL). In untreated cases of TEME, the bacterium may be isolated from the brain, kidneys, pleural fluid, lung sections, aspirated tracheal exudate, urine, blood, and preputial washings. Standard transport swabs containing Amies medium are appropriate for culturing of clinical samples. Isolation of H. somnus from joint fluid and CSF is usually unsuccessful.13 The kidneys and brain should be collected for postmortem examination because these tissues contain the highest concentrations of H. somni.1
Initial changes in the peripheral WBC count include neutropenia, left shift, and toxic changes in the neutrophils. In cattle that develop acute TEME, agglutinating antibody titers are invariably greater than 1: 400 and increase fourfold by 2 to 4 days after infection.14 Serum agglutination titers are greater than 1 : 1024 in convalescent cattle; they may be lower with inapparent infection or vaccination.15
■ Pathology Macroscopic pathologic lesions of the CNS include disseminated multifocal hemorrhages and infarctions in the spinal cord, brainstem, and cerebral cortex. Bacterial colonies are frequently observed in thrombosed blood vessels and the surrounding infarcted tissues. Ocular lesions are characterized by conjunctivitis, multifocal retinal hemorrhages, and areas of retinal edema. The CSF is cloudy and xanthochromic. A focal fibrinous meningitis is observed, and suppurative otitis may occur in some cases.
The earliest microscopic lesion of TEME is vasculitis that progresses to septic infarction and abscess formation. The lesions are usually found in the CNS, but in severe cases they may be disseminated throughout the body.
Nonneurologic lesions of H. somni infection include suppurative arthritis, synovitis, myocarditis, suppurative pleuritis, urogenital infections, and bronchopneumonia. Changes associated with the bronchopneumonia include infarction, cranioventral pulmonary consolidation, and hemorrhagic interstitial pneumonia. Other lesions include ecchymotic to petechial hemorrhages over the serous surfaces, purulent exudate in the joints, and ulceration of the laryngeal and tracheal mucosa with diphtheritic membrane formation.16
■ Treatment and Control During an outbreak, cattle must be examined frequently and should be treated when the neurologic signs first appear. H. somni is susceptible to many antibiotics and antimicrobial drugs. Drugs that have been reported to be effective for the treatment of TEME include tetracyclines, penicillin, aminoglycosides, and ampicillin. Parenteral oxytetracycline is regarded as the most cost-effective treatment for infected commercial cattle; the dosage is 10 mg/ kg of a conventional formulation given IV twice daily for 3 days or 20 mg/kg of a long-acting formulation given SC. Some authors advocate the addition of chlortetracycline (2.2 mg/ kg) to the feed for 10 successive days.17 This, however, would constitute off-label drug use in feed and is currently prohibited by the U.S. Food and Drug Administration. Chlortetracycline is approved as an oral drench for the treatment of H. somni pneumonia in beef, non-lactating dairy cattle, and calves in the United States at a dosage of 22 mg/kg for 5 days.
Antibody responses protective against respiratory challenge have been generated by vaccination with anionic, heat-stable proteins derived from the bacterial cell wall.18 Vaccination of cattle with commercial products affords substantial protection from experimentally induced H. somni septicemia and neurologic disease for more than 3 months18-20 (See Chapter 48 for more information about vaccines). Mass prophylactic treatment of affected cattle with a parenterally administered, long-acting oxytetracycline formulation may be efficacious in preventing TEME in cattle at high risk for the disease.21
Otitis Media/Interna of Ruminants
■ Definition, Etiology, Epidemiology, and Pathogenesis Otitis media/interna is a common bacterial disease of cattle and sheep; it is less commonly observed in goats. The condition usually occurs as a sequela to upper or lower respiratory infections caused by Mannheimia haemolytica, Pasteurella multocida, C. pseudotuberculosis, H. somni, or Mycoplasma spp.1-5 Subclinical otitis media/interna is common in feedlot-reared animals, particularly early in the feeding period.1,3 Although viral infections are the cause of a large proportion of otitis media/interna cases in children,5 the role of viral infections in ruminant otitis media/interna remains speculative; it is possible that viruses play a role in facilitating otitis media interna similar to that in facilitating lower respiratory tract disease. Because Mycoplasma spp. have been detected in clusters or outbreaks of otitis media/interna on dairy farms, contaminated milk is considered an important potential source of this organism in young stock.4,6 Chapter 31 includes more detailed discussion on the role of Mycoplasma spp. in the bovine respiratory disease complex.
Otitis media/interna is considered to most commonly result from ascending infection of the middle ear from the nasopharynx via the eustachian (auditory) tube.5 Infection that progresses from the external ear into the middle ear is less common but may occur secondary to aural infestation by ectoparasites. Once infection is established in the middle ear, it may extend into the inner ear as a result of erosion of bone or extension of the infection through the round or oval windows, or both. The constellation of clinical signs of otitis media/interna results from damage to the peripheral vestibular apparatus residing in the tympanic bulla and petrous temporal bone. In chronic cases, the peripheral vestibular apparatus can be damaged beyond repair, and neurologic deficits may be permanent. In rare cases, infection can extend into the CNS, which results in subdural abscess formation, meningoencephalitis, or brain abscess formation.5 The vast majority of cases shows clinical signs of unilateral peripheral vestibular disease; however, subclinical inflammatory lesions may be present in the contralateral, clinically normal side. Bilateral, clinically apparent peripheral vestibular disease is rare. Additional signs of multisystemic disease caused by Mycoplasma bovis, Pasteurella multocida, or H. somni may be present (e.g., pneumonia, polyarthritis).
■ Clinical Signs and Diagnosis Headshaking (possibly producing an aural hematoma), an ear droop, and reduction in appetite may precede the clinical vestibular signs. Fever is inconsistent.6 Patients with vestibular signs display unilateral head tilt (toward the side of the lesion), continuous horizontal nystagmus (fast phase away from the side of the lesion), and imbalance, manifested as a tendency to stumble, fall, or walk in a tight circle toward the side of the lesion. If the tympanic membrane ruptures, or in the rare case of otitis externa as a preceding condition, purulent exudate may be evident in one or both ears.
Affected animals may become recumbent and lie with the lesion side toward the ground; if turned, they return to the same position. Many animals with otitis media also develop ipsilateral facial nerve dysfunction, which results in ptosis, drooped ear, and flaccid lips and nostrils. In small ruminants, facial nerve paralysis results in deviation of the philtrum toward the normal side. Deviation of the philtrum does not occur in cattle because of the large amount of connective tissue surrounding the planum nasale. On occasion, affected animals develop subtle or pronounced signs of cortical or brainstem disease as a result of extension of infection from the middle ear into the meninges. CSF analysis may reveal increased leukocyte counts in such cases.
Although the clinical signs of peripheral vestibular disease are characteristic, it is important to differentiate this condition from that of central vestibular disturbance. Animals with peripheral vestibular disease are usually appetent, alert, and aware of their surroundings and do not have a significant deficit of postural placement. The nystagmus of these animals is constantly horizontal. In comparison, animals with central vestibular disturbances are depressed, have a nystagmus that varies in direction, and show marked conscious proprioceptive abnormalities.
Diagnostic imaging, including radiography, CT, and ultrasonography of the tympanic bulla, may be useful in confirming a diagnosis of otitis media/interna.
■ Treatment and Control Treatment of bacterial otitis with procaine penicillin (44,000 IU/kg IM or SC daily) may be effective. Because bacteria that do not have a cell wall (Mycoplasma spp.) may be involved, however, initial treatment with an antibiotic other than a member of the β-lactam class might be warranted (e.g., tetracyclines, florfenicol, macrolides, and, where legal, fluoroquinolones), unless bacterial culture and sensitivity results or clinical response indicates treatment with a β-lactam class antimicrobial drug.6 Relapses may occur, which warrants prolonged treatment (3 to 6 weeks). Treatment is effective in obtaining a complete cure of acute otitis but is less so in treating the chronic form. In chronic cases, infection may irreversibly damage middle or inner ear tissues, causing neurologic deficits that can persist despite resolution of infection with antimicrobial therapy. Osteomyelitis of the petrous temporal bone, abscess formation in the tympanic bulla, or a noninfectious cause (e.g., neoplasia) are other considerations for affected animals that do not respond to antimicrobial therapy.
Management practices aimed at reducing the risk for upper respiratory tract infection may aid in reducing the incidence of disease. In dairy herds with a history of otitis media/interna caused by Mycoplasma spp. in calves, pasteurization of waste milk fed to calves or feeding milk replacer instead of waste milk may be warranted.
Ear Mite Infestations of Ruminants
The ear mite of cattle is Raillietia auris, and that of small ruminants is Psoroptes cuniculi. Severe infestations perforate the tympanum and result in vestibular disease, facial paralysis, and ataxia.1-4 Infestation can be recognized by observation of ulceration and purulent debris in the auditory canal next to the tympanum. Mites may or may not be visible during otoscopic examination. Malodorous discharge on the side of the face under the ear canal may be observed in some affected animals.
The accumulation of purulent debris and the swelling of auricular tissues block the transmission of sound to the tympanum.
Ear mite infestations in cattle are common and in some herds may affect most of the adults. The biologic importance of the infestation may be related to changes in the herding or mothering behavior of range cattle. The economic significance of the infestation is unknown.
Ear mite infestations have been successfully treated in goats with eardrops containing rotenone once daily for 5 to 10 days. Good clinical responses can be obtained in cattle with the same treatment. Fenthion drops have also been used successfully. In cases of parasitic otitis in which the discharge has been inspissated, lateral resection of the ear canal should be considered to establish adequate ventral drainage.5 A single subcutaneous injection of ivermectin at 0.2 mg/kg has been shown to be an effective treatment for P. cuniculi otitis in both sheep and goats.6,7
The life cycle of the mite involves two free-living stages, the protonymph and deutonymph stages. These forms molt in the vegetation and reinfest cattle as they graze or bed during the evening. Therefore tilling the soil of the infested pastures or re-treating cattle every 14 to 21 days with insecticide should be considered as part of an eradication scheme.
Diseases Producing Tremors and Ataxia; Cerebellar Diseases even flip over backward. Severely affected foals that fall often panic and struggle for some time before standing.
The diagnosis in an Arabian foal with compatible clinical signs is strongly supported by demonstration of homozygosity for the cerebellar abiotrophy allele. This test requires submission of 20 to 30 hairs with roots to the Veterinary Genetics Laboratory at the University of California, Davis (http:// www.vgl.ucdavis.edu/services/horse.php). Hematologic and serum chemistry findings are usually normal. Some foals have high CSF protein concentration and creatine kinase activity, which are consistent with active neurodegeneration at the time of CSF collection.11 MRI, and possibly CT, of affected foals reveals atrophy of the cerebellum in foals with cerebellar abiotrophy.13
Signs may be stable after onset or get worse for up to several months. It is rare, however, for foals with cerebellar abiotrophy to become persistently recumbent. Modest improvement has been noted in some mildly affected horses once they become adults.9 Foals with cerebellar abiotrophy seldom succumb to direct effects of the condition, but most are euthanized because of severe clinical signs and poor prognosis.
Gross appearance of the affected brain is usually described as normal; however, the ratio of cerebellar to whole brain weight is usually less than 8%, whereas normal ratios are 8% or higher. The characteristic histologic lesion is thinning of the cerebellar cortex, affecting both granular and molecular layers.2,9-12 There is marked reduction in the number of Purkinje cells in the granular layer, and some of those remaining show degenerative changes (swelling, shrinkage, and hyperchro- masia of the perikaryon). There is relative sparing of the Purkinje cells of the nodulus and flocculi.11 Vacuolation may be noted in the olivary nuclei, and mineralized neuronal cell bodies may be found in the thalamus adjacent to the third ventricle.10