Hepatic Lipidosis*
Vincent Dore
Fat Cow Syndrome and Lipid Mobilization Syndrome
Hepatic lipidosis (fat cow syndrome) is a multifactorial condition that occurs in dairy cows after parturition.
The syndrome is characterized by progressive depression and failure to respond to treatment of other predisposing diseases. It is associated with excessive mobilization of fat to the liver in well-conditioned or overconditioned cows. This mobilization of fat is induced by the negative energy balance and hormonal changes that occur around the time of calving. This negative energy balance in most cases is aggravated by concurrent periparturient diseases that reduce feed intake and increase energy needs.1-3Fat cow syndrome occurs sporadically in dairy cows but more frequently in cows that become overconditioned during late lactation and during the dry period.2 The overconditioning may be caused by a poor breeding program associated with cows having very long lactations or extended dry periods and having excessive weight gain. Mortality can exceed 25%, with even higher rates occurring without intensive treatment and correction of concurrent diseases. Clinical disease in obese cows that enter the dry period can be minimized by carefully controlling their diets to meet National Research Council (NRC) requirements and preventing milk fever.
■ Clinical Signs The clinical condition occurs in the postparturient period. Most affected cows are either obese or very well conditioned, with a large amount of omental and subcutaneous fat. Presenting signs usually include depression, anorexia, weight loss, and weakness that can lead to recumbency. Most have nonspecific signs like decreased rumen motility and decreased milk production. Other signs vary and are related to concurrent diseases. The concurrent diseases most frequently seen are metritis, retained fetal membranes, mastitis, parturient paresis, and displaced abomasum.1 It is important to look for these other diseases; even if mild, they could be significant in these cases and must be treated.
■ Diagnosis Most laboratory tests are poor indicators of hepatic lipidosis and are of little value in determining disease severity.4 Liver-derived enzymes are usually elevated above the level in the dry cow but are often within normal ranges. Liver enzymes most consistently elevated in cases of hepatic lipidosis are OCT, total bilirubin, and AST.5 Bile acid concentrations have not been shown to be significantly increased in most cows with fatty liver.5 Many cows with hepatic lipidosis have leukopenia and a degenerative left shift, but this is not specific. As expected, non-esterified fatty acid (NEFA) levels will be increased, and triglycerides and cholesterol will be decreased. Most of the total cholesterol is in lipoproteins. The sulfobromophthalein dye excretion test may be useful prognosti- cally because those with a half-life longer than 9 minutes have a more guarded prognosis.6 Measurement of serum paraoxonase
^Contributions to previous editions by John Maas and Erwin G. Pearson are acknowledged.
1, an enzyme exclusively synthesized by the liver, was recently assessed for its ability to diagnose hepatic lipidosis and showed promising results.7 Decreases in some amino acids, such as glycine and glutamine, can also be observed with increasing severity of hepatic lipidosis.8
Several recent studies have examined ultrasound as a tool to detect hepatic lipidosis in cattle. With increasing fat accumulation in the liver, an increased gray level (hyperechogenicity) is seen in the ultrasound image, and the liver appears brighter. Overall, hepatic vessels seem to be smaller. However, this is subjective and is also dependent on the settings of the machine. One study found that the liver increases in size and becomes rounded with increasing severity of lipidosis; however, measuring the thickness of the liver and angle of the ventral margin had limited diagnostic value.9 Another study used digital analysis of hepatic ultrasound images via a computer-aided ultrasound system and found that imaging findings correlated well with liver triacylglycerol concentrations.10 Digital analysis of B-mode liver images used a computer program to correct for abdominal wall effects and removal of artifacts.
Although not commonly available at this point, the use of ultrasound and computer-aided correction has the potential to help determine the severity of hepatic lipidosis and to estimate with high accuracy the triacylglycerol content of the liver.11Although clinical chemistry and ultrasound may be helpful in diagnosing hepatic lipidosis, a liver biopsy is the gold standard. Liver biopsy may confirm the fatty infiltration of the hepatocytes, but a moderate to high amount of fat is present in the liver of all postparturient, high-producing dairy cows, even those that remain healthy.12 Fat is usually quantified using histologic methods by determining percentage of hepatocytes containing lipid vacuoles, measuring total hepatic fat on a wet-weight basis, or floating in copper sulfate solutions of various specific gravity (to estimate total fat on a wet-weight basis).13 Classification schemes characterizing severity of hepatic lipidosis based on percentage of hepatocytes containing fat vacuoles have been presented (e.g., 75% being equal to mild, moderate, and severe lipidosis, respectively).4 More recent studies have advocated the use of triacylglycerol analysis on a wet-weight basis to differentiate degrees of hepatic lipidosis.3 These studies categorized hepatic lipidosis as normal, mild, moderate, and severe by triacylglycerol concentrations of less than 1% (100 mg/g), respectively.3 At present, triacylglycerol analysis of hepatic tissue is not a routine procedure in veterinary diagnostic laboratories, so total hepatic fat concentrations remain the gold standard for laboratory diagnosis. A recent study evaluated the correlation between cytology of the liver biopsy and triglyceride concentration. The study showed that hepatic triglyceride concentration could be estimated with better accuracy by making touch imprint preparations of liver biopsy specimens than by measuring BHBA or NEFA.14 Clinically, little correlation exists between the amount of hepatic fat and signs of disease until the fat is more than 34% wet weight, at which point the liver tissue will float in distilled water with a specific gravity of 1.000.
Generalized obesity is noted at necropsy unless the animal has been sick for more than 1 to 2 weeks. Changes in the liver are most striking; it is enlarged with swollen and rounded edges, is pale yellow in color, and may float in water. Histologically, there is fatty infiltration of the hepatocytes, especially in the centrilobular and intermediate areas. However, these liver tissues are sometimes not much different from those of healthy, high-producing dairy cows in early lactation.
■ Pathophysiology Storage of excess energy as fat and the periodic mobilization of fat for use as energy by the body is crucial.2,3 The liver plays a major role in lipid metabolism and must process the absorbed chylomicrons, the volatile fatty acids, and many of the fatty acids and much of the glycerol obtained by mobilization of fat from adipose tissue (Fig. 33.8). The liver of large herbivores has unique functions because much of the dietary energy is absorbed as volatile fatty acids and not glucose. Glucose is still needed (in high amounts in lactating animals) and must be produced by gluconeogenesis, 85% of which takes place in the liver.15
Negative energy balance is induced by lactation, fetal growth, exercise, decreased feed consumption, environmental chilling, and diseases (Fig. 33.9). During these periods of negative energy balance and before lactation, blood glucose may drop slightly, the insulin/glucagon ratio drops, and these and other hormones (e.g., catecholamines, growth hormone) activate hormonesensitive lipases that convert tissue fat to free fatty acids (FFAs) or NEFAs and glycerol (Fig. 33.10). After a 4-day period of fasting in cattle, plasma insulin concentrations decreased and insulin-stimulated blood glucose reduction was decreased as compared to cows that were not fasted.16 In this study, insulin response was negatively correlated with plasma NEFA and liver triglyceride concentrations, suggesting that decreased insulin response may be an important complication of negative energy balance.
In the liver, the glycerol may be used to produce glucose or may be recombined with FFAs to make triglycerides (TGs). In addition to being recombined with glycerol to make TGs, the fatty acids may be degraded through β-oxidation, and the two carbon fatty acids converted to acetyl coenzyme A (CoA). The acetyl CoA combines with oxaloacetate to enter the tricarboxylic acid (Krebs) cycle for the production of energy. This pathway is in competition with the use of oxaloacetate for gluconeogenesis.2 If there is not enough oxaloacetate available, the acetyl CoA is converted to ketone bodies, which in high concentrations can reduce feed consumption and perpetuate the negative energy balance.When the liver is overwhelmed with mobilized NEFAs, greater amounts of TGs are deposited within the hepatocytes. These TGs eventually leave the liver as very low-density lipoproteins (VLDLs), which are plasma-soluble complexes of phospholipid, cholesterol, TG, and apolipoprotein A. Hepatic lipidosis results when the rate of hepatic triglyceride formation exceeds oxidation of fatty acids and the formation and release of VLDLs into the peripheral circulation. A number of factors have been incriminated in the inability of the liver to secrete adequate VLDLs to keep up with the deposition of TGs brought about by FFA mobilization from fat. Ruminants have a poor ability to export excess lipid from the liver as VLDLs. This is particularly true in bovine hepatic lipidosis17,18 and is theorized to result from a shortage of apolipoprotein A. Hepatic lipidosis can be induced in cows by inhibiting the production of apolipoprotein,19 and the lowest concentrations of lipoproteins occur in the serum of cows with the most severe hepatic lipidosis.18 Cows on low-protein diets in the dry period are more likely to develop hepatic lipidosis than those on higher protein diets, regardless of the energy content.17 Depression in drymatter intake in the final week before calving will increase the liver TG content after calving in dairy cows.20 Hepatic lipidosis can be consistently reproduced experimentally in cattle by limit feeding or fasting overconditioned cows immediately after calving.2 In the past, a lack of phospholipid or its precursor choline has been incriminated but never substantiated.
However, in the face of an energy shortage, it seems redundant and a waste of energy to repackage fat and send it back to the tissues, even if the liver is being overwhelmed with fatty acids. Some of the same endocrine hormones that activate hormone-sensitive lipase and inhibit lipogenesis and glycogen synthesis may also inhibit production of VLDLs.It has also been suggested that subclinical liver damage may inhibit the production of VLDLs, but experimental studies have indicated no significant elevation in liver-specific enzymes before
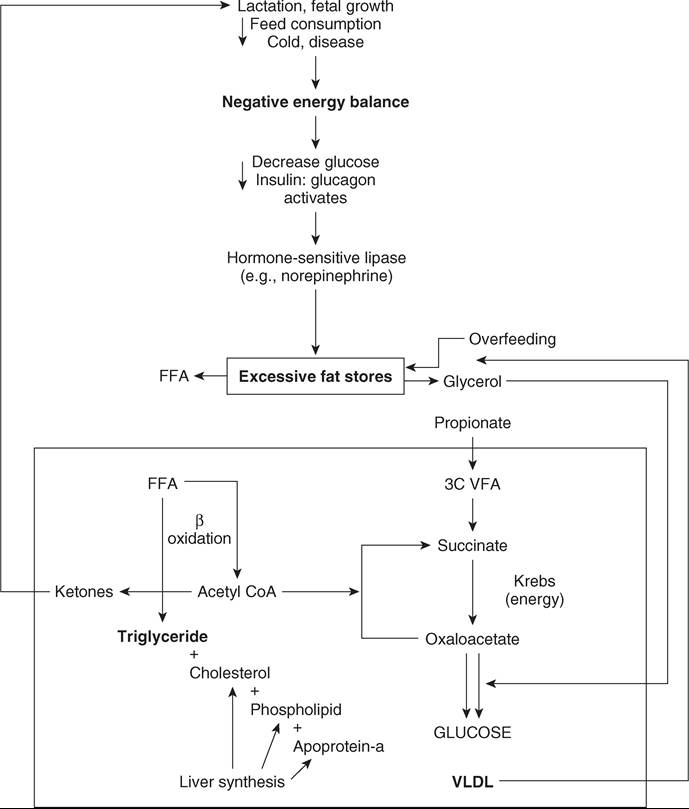
FIG. 33.8 Metabolism of fat in animals with hepatic lipidosis. 3C VFA, Volatile fatty acid; CoA, coenzyme A; FFA, free fatty acid; VLDL, very low-density lipoprotein.
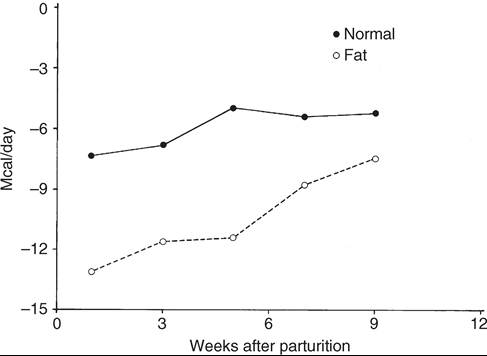
FIG. 33.9 Energy balance (megacalories per day) in normal-condition and obese dairy cows after parturition. (From Perkins B: PhD thesis. Cornell University, Ithaca, NY, 1983.)
lipid accumulation.12 Function may eventually be impaired by the accumulation of fat, because fasted cows have a decrease in the surface area of rough endoplasmic reticulum and the number of mitochondria per unit volume.21 Changes in the liver seem to be functional and not degenerative.22 Hepatic lipidosis appears to be a reversible condition if the cause is removed and energy balance becomes positive (less negative). In cows fasted and then returned to full feed, all major liver functions returned to normal within 18 days of refeeding, and all lactating dairy cows with postparturient hepatic lipidosis had normal liver fat content (liver content. There were trends for increased milk yields, fat and 3.5% fat milk-correction, but no significant increase.27 Addition of inositol both before and after birth did not reduce the incidence or severity of hepatic lipidosis.26 Methionine at 40 to 50 g/day has also been used for the same purpose. Nicotinic acid (niacin) fed at 6 to 12 g/head/day may help reduce lipolysis at the tissue level and thus reduce the amount of fat presented to the liver.28 Treatment of hepatic lipidosis with nicotinic acid is often associated with a rebound of clinical signs, and its use as a preventive measure is recommended.
Despite the treatments listed previously, it is imperative to get cows suspected of having fatty liver eating again. Everything possible should be done to encourage dry-matter intake. Appetite can sometimes be enhanced by transfaunating with rumen fluid from a normal cow. This may increase the absorption of volatile fatty acids used for energy and for glucose precursors. Prognosis must be guarded unless the concurrent diseases can be treated successfully and the liver fat mobilized. It is most important to treat the primary disease. Reducing the negative energy balance and treating the hepatic lipidosis must be attacked vigorously.
■ Prevention Prevention is based on preventing overconditioning during the late lactation period and dry period and treating periparturient diseases in a timely manner. Hepatic lipidosis and associated conditions are most common in dairy cattle. Preventing obesity in cows during late lactation is an important factor in controlling this disease. This process involves a successful breeding program (maintaining a 12- to 13-month calving interval), monitoring body condition (calving, breeding, mid-lactation, and dry periods), and closely matching energy in the ration to the level of milk production during late lactation. Once the cow reaches 7 months of pregnancy and the dry period, any dietary restriction below requirements for maintenance and pregnancy are certain to be counterproductive.
Prevention of hepatic lipidosis involves minimizing or eliminating the primary risk factors associated with disease both pre- and postpartum. The primary prepartum risk factors for fatty liver include obesity (body condition score ≥4.0), severe feed restriction, feeding excess energy, and long calving interval. Postpartum risk factors include other concurrent diseases, anorexia or fasting, feed restriction, and sudden feed changes.3 Adequate protein in the dry period is essential.15,19 It has been shown that cows fed higher protein diets during the dry period will perform better in the lactation that follows. Feeding good- to excellent-quality roughages (hay, silages) to meet most of these requirements is preferred. Additional grain 2 to 4 weeks before parturition is important to acclimate the ruminant to anticipated changes in the rations fed after calving. It must be stressed that high-quality dry cow rations be fed but not overfed. Dry-matter consumption should be limited to approximately 2% of body weight per day while meeting requirements. Other factors in the dry cow ration also must be considered to prevent periparturient diseases such as milk fever, displaced abomasum, mastitis, metritis, ketosis, ruminal lactic acidosis, and retained placenta. Rations should be adequately supplemented with cobalt, the precursor of vitamin B12 that is a cofactor in the rate-limiting step in conversion of propionate (the primary glucose precursor) to succinyl CoA. Nicotinic acid has been included in the dry cow ration at 6 g/head/day and in the early-lactating cow ration at 12 g/head/day to aid in the prevention of ketosis, which is a major risk factor for the development of hepatic lipidosis. The use of monensin in the dry cow ration and the early-lactation ration shows promise to aid in preventing ketosis and thus may be of some benefit in preventing hepatic lipidosis.29,30 Other approaches such as sodium borate or administration of glucose precursors in the dry period have also been attempted.3
Immediately and aggressively treating cows (particularly obese cows) for other diseases that occur after calving is important in preventing fatty liver. This includes both infectious diseases (e.g., mastitis, metritis) and metabolic diseases like hypocalcemia. It is important to limit stress on fresh cows and provide adequate bunk space, good ventilation, and high-quality feed. Anything possible to encourage dry-matter intake is important. Several different therapies have been promoted to improve the metabolic state of cows during late gestation by supplying an extra source of glucose and decreasing the mobilization of NEFAs from fat. For example, subcutaneous injections of glucagon beginning 2 weeks prior to calving increased glucose and insulin concentrations and decreased plasma NEFA levels in a model of hepatic lipidosis.31 Feeding an oral drenches of 1 L/day of propylene glycol for the last 10 days prior to calving also increased glucose and insulin level with decrease in NEFA and BHBA concentrations.3,32 Slow- release doses of insulin (0.14 IU/kg) have also shown some efficacy in preventing triacylglycerol accumulation in the liver, but higher doses (0.29 IU/kg) can result in profound hypo- glycemia.33 Growth hormone had no beneficial effect.34
Protein-Energy Malnutrition and Pregnancy Toxemia of Beef Cows
Protein-energy malnutrition (PEM) and pregnancy toxemia of beef cows are conditions of pregnant beef cattle on marginal diets, usually occurring in the winter and characterized by weight loss, weakness, depression, and sometimes inability to rise. The condition is the result of the negative energy balance caused by decreased quality and quantity of feed when caloric requirements are increased by fetal development and cold weather. Growing, pregnant heifers are especially susceptible because energy requirements for growth are superimposed on the other caloric requirements. A number of other factors, such as unpalatable feed, snow cover, and diseases, may reduce caloric intake. Fatty infiltration of hepatocytes occurs transiently in early PEM, and at necropsy the liver is smaller than normal.
Animals are usually thin and have a long hair coat. In some cases, they are down and unable to rise but are still alert. The body temperature may be normal or subnormal. Occasionally the cows also develop diarrhea. Most animals die 7 to 14 days after becoming recumbent.35 Differential diagnosis includes Johne's disease, lymphosarcoma, parasitism, chronic pulmonary disease, other deficiencies, and debilitating diseases.
■ Diagnosis Diagnosis is usually based on demonstrating decreased caloric intake and ruling out other chronic diseases that could cause debility. Laboratory tests support but do not rule out the disease. Total serum calcium may be decreased. Packed cell volume also may be decreased, and serum insulin levels may be reduced. Ketonuria is not typical in PEM. At necropsy, muscle mass usually is decreased. Serous (brown) atrophy of fat is often present, especially in the coronary groove, bone marrow, and perirenal areas. Lesions of concurrent disease also may be found if PEM is acute, and a fatty yellow liver may be noted.
■ Treatment Treatment is often unrewarding. Efforts to reverse an advanced catabolic state may fail. A 454-kg cow requires 13 Mcal of metabolizable energy daily, or approximately 6.5 L of 50% glucose solution by continuous drip. Alfalfa pellet gruels are helpful if force-fed, and approximately 11 kg/day of alfalfa is recommended. Propylene glycol (150 to 200 mL) orally twice daily can be helpful as a glucose precursor. Treatments include IV fluids, improving the energy balance, and treating any concurrent disease.
■ Prevention Nutrient requirements increase greatly for beef cattle during the third trimester of pregnancy. As forage quality (digestibility) decreases, the time feed material stays in the rumen increases (increased rumen turnover time). Therefore as quality decreases, the maximum dry-matter intake (DMI) decreases, which greatly decreases the maximum nutrient (energy) intake. This compounding effect of poor-quality forage on maximum intake is particularly important for preventing hepatic lipidosis and the accompanying protein-calorie malnutrition (PCM) of pregnant beef cattle in the winter. The approximate maximum DMI of forage of poor quality (oat straw, corn stover), medium quality (meadow grass hay), and excellent quality (alfalfa hay [25% crude fiber], corn silage) is 1% to 1.5%, 2%, and 2.5%, respectively. Environmental temperature can increase energy needs for beef cattle on pasture or range; as the temperature falls from 20° C (68° F) to 10° C (50° F), roughly 10% more energy is necessary for maintenance, and at freezing temperatures, 0° C (32° F), 20% additional energy is required. The key to preventing PEM in pregnant beef cattle is adequate body condition (scores of 5 to 7) entering the third trimester and availability of good-quality to excellent-quality forage in adequate amounts.
Pregnancy Toxemia in Ewes and Does
Pregnancy toxemia, also known as ketosis or twin lamb disease, is a condition that occurs in ewes and does during the last 2 to 4 weeks of gestation. It is characterized by anorexia, weakness, and depression. Nearly 80% of the fetal growth occurs in the last 6 weeks of gestation, which can result in a negative energy balance occurring from the increased energy demands of rapid fetal growth in late gestation and insufficient feed intake. The incidence of pregnancy toxemia is greater in ewes with more than one fetus, during the last 2 to 4 weeks of gestation, and in does with three or more fetuses.36 Poor-quality feed, cold weather, lack of exercise, and stress of movement during the period at risk also may increase the incidence. Overweight animals are also more likely to suffer from negative energy balance and develop the disease. Does seem to be more resistant to pregnancy toxemia than ewes, in that three or more fetuses are usually required to produce the condition. Prevalence in the herd varies from less than 5% to up than 20% in some herds, depending of the predisposing factors and nutritional state.
Initial clinical signs include partial to complete anorexia and separation from the rest of the flock or herd. The disease will progress to severe depression and recumbency. Neurologic signs such as tremors, star-gazing, incoordination, circling, blindness, and grinding the teeth may precede terminal depression. If untreated, animals will appear comatose in lateral recumbency and will die shortly after developing neurologic signs. Differential diagnosis includes other periparturient diseases, such as mastitis and hypocalcemia, as well as polio- encephalomalacia, enterotoxemia type D, and toxicoses.
■ Diagnosis Ketonuria is usually present and detected before ketonemia. Hypoglycemia is not a consistent finding but is sometimes present. Some authors associated sudden hyperglycemia in previously hypoglycemic goats suffering from pregnancy toxemia with death of the fetus.37 Affected ewes and does often are generally acidotic and may have lowered serum calcium and potassium levels.38 Blood urea nitrogen (BUN) and creatinine levels are elevated terminally in some cases. Fatty acid concentrations in the plasma are usually elevated above 500 μEqZL. Serum β-hydroxybutyrate (BHB) concentrations are elevated (>1 mmol/L) using electronic on-farm test in goat and sheep.39-42 A nonspecific but marked neutrophilia may be found in some affected animals and is particularly dramatic in does, sometimes reaching 35,000 neutrophils^L.
■ Treatment Treatment of pregnancy toxemia is based on two principles: (1) administering exogenous energy sources (i.e., glucose) and (2) removing the factors increasing the energy demand on the animal (i.e., fetuses). Mortality is high unless treatment is started early and the fetuses are removed—the most important step—either by inducing parturition or by cesarean section. Parturition can be induced in ewes with 15 to 20 mg of dexamethasone; in does the dose is either 10 mg of dexamethasone or 10 μg of prostaglandin F2α.42,43 A cesarean section may be performed if the animal's value warrants it and there does not seem to be enough time to induce parturition. Besides removing the fetuses, the ketotic condition should be treated with IV glucose (250 to 500 mL of 10% to 20% glucose as an IV bolus followed by a slow IV drip of 5% to 10% glucose). Acidosis and hypocalcemia must be corrected if present. Administration of oral propylene glycol as a glucose precursor has also been advocated. Although recommended doses vary, an initial treatment of two doses (150 to 200 mL) given at a 12-hour interval followed by 60 mL per dose thereafter for 3 to 6 additional days appears to work well.43 Giving recombinant bovine somatotropin at a dose of 0.15 mg/kg of body weight also has shown some benefit.44 The energy intake must be increased. If the ewe is down and unable to stand, removal of the fetuses should be performed by cesarian section as soon as possible. In such cases the prognosis is often poor, so euthanasia of the ewe or doe must be considered. Immediately after parturition or cesarian section, the animal should be started on broad-spectrum antibiotics along with flunixin to prevent metritis.43
■ Prevention Preventing pregnancy toxemia and the associated severe hepatic lipidosis in ewes and does requires measures similar to those outlined for PEM in beef cattle. Both overconditioned and thin ewes and does in the third trimester of pregnancy are at increased risk. Because of the common occurrence of twins and triplets, nutrient requirements for pregnant ewes greatly accelerate during this period. Goodquality to excellent-quality forage for feeding sheep is very important. An additional tool for diagnosing underfeeding in ewes and goats is measurement of plasma BHB during the last month of pregnancy.45 This test greatly facilitates assessment of nutritional inadequacy in pregnant ewes. Plasma BHB concentrations of 0.8 mmol/L or higher are diagnostic of the need for increased energy consumption by pregnant ewes. Does have been shown to have a significant decrease in blood pH, bicarbonate concentration, and base excess values well in advance of the clinical signs associated with pregnancy toxemia.38 Therefore these parameters could also be early indicators of disease in pregnant sheep or goats. Measures of the cardiac biomarker troponin I could also be used as a prognostic indicator in sick goats prior to cesarean section.46
Hyperlipemia and Hypertriglyceridemia in Ponies
Hyperlipemia is a life-threatening condition that occurs in horses, ponies, and occasionally donkeys.47-49 It is characterized by a fatty liver and serum that is cloudy with accumulation of lipids. Triglycerides are usually much higher than 500 mg/dL.47 The condition is caused by decreased caloric intake, which causes fat mobilization and fat accumulation in the liver and accumulation in the plasma. The decreased food intake may be secondary to other diseases. Suggested predisposing factors include hypophagia, pregnancy, or lactation, often in obese ponies, American Miniature horses, or donkeys.48-50 The incidence of hyperlipemia is greater in ponies than in horses. It is seen more often in the winter, especially from February to May in animals receiving poor feed. Pregnant animals and those that are lactating are affected more frequently.
Equine hyperlipemia is characterized by production of an abnormal VLDL fraction (VLDL1) that has a reduced content of apolipoprotein B-100 and an increased content of apolipoprotein B-48.51 The substitution of B-48 for B-100 is thought to allow greater TG content because B-48 is the apolipoprotein of importance in chylomicrons. The activities of lipoprotein lipase and hepatic lipase, the enzymes responsible for VLDL catabolism, were increased in hyperlipemic ponies.51 It was concluded that overproduction of VLDL is the cause of hyperlipemia, possibly complicated by defective catabolism.
Hyperlipidemia is a mild condition of ponies and horses characterized by mildly elevated TG concentrations (100 to 500 mg/dL), clear plasma, and no evidence of hepatic dysfunction.47 An increase in caloric intake is usually sufficient to reverse the condition. The more severe condition, hyperlipemia, is discussed further.
■ Clinical Signs The clinical signs of hyperlipemia are nonspecific. Ponies usually are anorexic, depressed, weak, and uncoordinated. Diarrhea, colitis, cachexia, ventral edema, and abdominal pain are frequently seen in presenting cases.52,53
■ Diagnosis Definitive diagnosis is based on an increased level of circulating TGs (>500 mg/dL). Gross examination of the blood and plasma to detect the white to yellow opacity caused by the presence of lipids is a fast method to evaluate the presence of lipemia. TG level and presence of gross lipemia and clinical disease are used to differentiate between the types of hyperlipidemias in horses. Those values are summarized in Table 33.8. Bilirubin usually is elevated, as in most horses that are fasted. Fatty acids are also increased. Bromosulfophthalein clearances are delayed and, terminally, a large base deficit may be caused by metabolic acidosis.47
Postmortem examination reveals fatty infiltration of the liver and kidneys, which are pale and swollen and have a greasy texture. In ponies the liver is sometimes ruptured, resulting in intraabdominal hemorrhage and death. Renal lesions may be seen histologically. There may be a primary disease that produces anorexia and secondarily has resulted in hyperlipemia.
■ Treatment It is most important to treat any primary disease to alleviate the cause of anorexia and correct the negative energy balance. Resting energy requirements of a sick, hospitalized horse have been estimated at 22 to 23 kcal/ kg/day.53 Nutritional support is critical, in the form of either dextrose-supplemented fluids or partial parenteral nutrition. Oral supplementation using a 60-mL dose of corn syrup (4 kcal/mL) given orally every 2 hours will provide around 5 kcal/kg/day to a 500-kg horse and is usually well tolerated.53 Heparin is also recommended in some cases and has been shown to decrease triglyceride concentrations in affected horses.52 Regular insulin (0.2 IU/kg) IM every 3 to 6 hours can be used initially for severely
■ TABLE 33.8
Types of Hyperlipidemias in Horses

Modified from McKenzie H: Equine hyperlipidemias. Vet Clm Equine 27:59-72, 2011.
Iipemic animals; however, this is usually discontinued within 24 hours and a longer-acting product is used for maintenance. Protamine zinc insulin (PZI) has been used at an IM dose of 30 IU twice daily with 100 g of PO glucose for a 200-kg pony. This is continued on odd days; on even days, IM injections of 15 IU of PZI are given twice daily.47 Ultralente insulin can be given at a dose of 0.4 IU/kg SC q24h.52 The use of a continuous rate infusion at 0.07 IU/kg/h with concomitant IV drip of glucose to avoid hypoglycemia can also be used. If the hyperglycemia (>180 mg/dL) is not adequately controlled after 2 to 3 hours at the initial rate, increase the rate by 50%. Further increases can be made; however, it is important to allow the dose to equilibrate over a period of several hours before adjusting the dosage. Close monitoring of blood glucose levels is required while using insulin therapy. Slow IV drip of glucose for several days or until lipemia clears may be indicated. Heparin (100 to 250 IU/kg SC twice daily) has been used to alter the lipoprotein lipase activity and inhibit hormone-sensitive lipase of adipose tissue, but it may alter coagulation enough to cause hemorrhage.
The presence of hyperlipidemia is readily detected and easily solved by increasing caloric intake. Although therapy of hyperlipemic ponies and horses is often unrewarding, the diagnosis is relatively straightforward, and prevention depends on providing adequate feed of good quality and avoiding high- stress situations.
■ Prognosis High mortality rates have been seen with hyperlipemia in ponies and donkeys. Previous studies reported mortality rates between 22% to 80% in hyperlipemic ponies.54 A recent study from the United Kingdom revealed a mortality rate of 48.5% in donkeys due to hyperlipemia.55 The donkeys were from a donkey sanctuary, and the disease prevalence was 10.7% over the study period. Development of hyperlipemia was highly associated with the presence of a concurrent disease (odds ratio [OR]: 76.98). Other risk factors associated with development of the disease were cardboard bedding, movement to the sanctuary in the previous 2 weeks, weight loss of more than 10 kg in the last month, dental disease, and concentrate feeding. Even if the prognosis is often grave, decreased mortality rates have been observed when adequate and aggressive treatment is performed.49