ESOPHAGEAL STRICTURES
Esophageal strictures occasionally occur in dogs and cats. Stricture usually occurs secondary to severe esophagitis that extends into deeper layers of the esophagus, inciting fibroblastic proliferation.
Common causes of this degree of esophagitis in dogs and cats are reflux of gastric acid and enzymes during general anesthesia, persistent vomiting in patients that are also weak and recumbent (e.g., patients with parvoviral enteritis, pancreatitis), medications that induce esophagitis when they become lodged in the esophagus (e.g., that caused by NSAIDs in dogs, doxycyline tablets in cats), ingestion of strong acid or alkali, foreign body trauma, and thermal burns. Severe stricture may also occur in cats that develop esophagitis after a large hairball has been vomited or has become lodged in the esophagus. I have treated cats that developed a severe esophageal stricture within 7 to 14 days after vomiting a hairball as long as 12 to 15 cm. Presumably, the coarse texture of the hair significantly irritates the esophageal mucosa as it sits in and subsequently is ejected from the esophagus. Acid and enzymes that are mixed in the hair material add to the damage. Figure 4-12 illustrates a case in which a large hairball was lodged in the esophagus for approximately 36 hours before it was removed. Severe esophagitis resulted, and within 10 days there was a stricture, despite aggressive early medical management for esophagitis.Anesthesia-related reflux is the most common cause of esophageal stricture. Stricture formation can occur after relatively short anesthetic procedures (e.g., for ovariohysterectomy), as well as after long procedures. It appears that prolonged anesthesia, especially when followed by inability of a patient to resume sternal or upright posture, promotes gastroesophageal reflux that may persist even beyond the duration of the anesthesia, and thereby initiating and perpetuating to some degree the transition from severe esophagitis to stricture formation.
Clinical signs of dysphagia and regurgitation are usually evident by 5 to 14 days after the anesthetic episode. Occasionally, significant clinical signs are not evident until 4 to 6 weeks later. Variable degrees of luminal narrowing can occur, and in some patients the lumen diameter at the stricture site is extremely narrow (sometimes as small as 1 to 2 mm) (Figure 4-13). Stricture length also varies. Occasionally, one or two additional strictures will develop at other sites in the esophagus.
Clinical Signs
Clinical signs generally progress over 5 to 14 days after their onset. The predominant sign is regurgitation of solid food. In some patients there initially is vomiting during the recovery phase after an anesthetic event that is followed by occasional vomiting over the ensuing several days. Regurgitation may then begin to occur. As a stricture worsens, only gruels can be successfully transported to the stomach. In strictures associated with a very narrow luminal diameter (1 to 2 mm), only water is likely to be retained. Affected patients typically remain active and alert and have excellent body condition. Signs of pain or discomfort are uncommon. The appetite is usually ravenous. Weight loss may occur over time as a result of decreased caloric intake associated with regurgitation.
Diagnosis
Esophageal strictures occur more commonly than many clinicians may recognize. A review of a patient's recent medical history is the first step in making an early diagnosis of esophageal stricture. Most patients with an esophageal stricture have undergone general anesthesia within the previous 2 to 3 weeks. Most patients that begin regurgitating shortly after an anesthetic event have an esophageal stricture. A recent history of frequent severe vomiting in dogs or cats, onset of regurgitation associ-
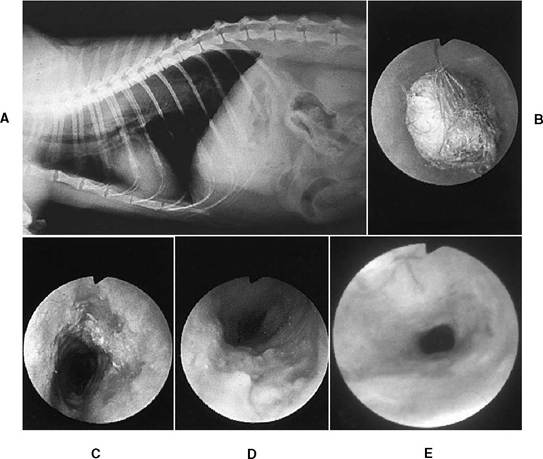
FIGURE 4-12 Esophageal foreign body in a cat with subsequent development of esophageal stricture.
A, Note the long area of increased opacity in the dorsocaudal thorax (later confirmed to be a hairball). The history included salivation, increased respiratory rate, and anorexia. B, Esophagoscopy confirmed a diagnosis of esophageal foreign body (hairball). The hairball was very tightly wedged in the esophagus. It could be neither pulled orad nor pushed back into the stomach. A gastrotomy was done, and the hairball was pulled back to the stomach and removed. C, Immediate postoperative esophagoscopy, showing erosive damage of the esophagus (twelve o’clock and five o’clock positions). Sucralfate suspension, famotidine, metoclopramide, and corticosteroids were instituted for severe esophagitis. There was concern that an esophageal stricture might develop. D, Appearance of the esophagus 4 days after surgery. The mucosa was quite irregular and friable. There is evidence of esophageal narrowing and early stricture formation. E, Endoscopic appearance of an esophageal stricture identified at 10 days. Balloon dilation procedures were initiated.ated with administration of NSAIDs to dogs, doxycycline tablets to cats, or other medications, or recent vomiting of a large hairball by a cat also should heighten suspicion of esophageal stricture.
A diagnosis is established either by endoscopy or by barium contrast radiography using a swallow of barium and either static radiographs or fluoroscopy (Figure 4-14). In some cases barium liquid mixed with food is required to demonstrate an esophageal stricture, since liquid barium may pass easily through a stricture without delineating its presence. Endoscopy allows evaluation of the appearance and pliability of the esophageal wall and luminal diameter. The endoscope is often too large to pass through the stricture area, so an assessment of stricture length often is not possible from direct examination alone. Stricture length can be assessed, however, by advancing endoscopic biopsy forceps through the stricture and then opening the cups once the instrument has been passed.
As the biopsy instrument is then retracted, the open cups will stop at the distal border of the stricture. A determination of stricture length also can be made by insufflating air into the esophagus, using the endoscope, and then making a lateral survey thoracic radiograph. There is an increased opacity at the stricture site as compared with the surrounding air.Esophageal neoplasia occasionally causes intramural stricture formation, and there usually is an appearance of mucosal irregularity and intraluminal mass effect. However, rarely a malignant stricture will appear benign with no intraluminal mass effect typical of neoplasia. If any uncertainty exists regarding the cause of a stricture (e.g., no recent
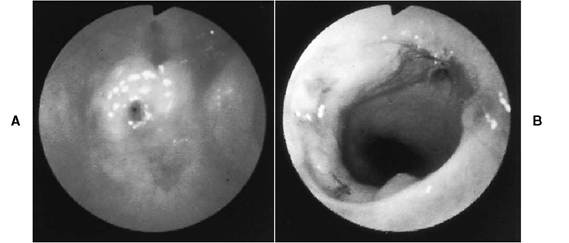
Figure 4-13 Severe cranial thoracic esophageal stricture in an 11-month-old cat that had been anesthetized 14 days before. There was a 5-day history of regurgitation that progressively worsened, resulting in referral for endoscopy. A, The extremely narrow esophageal lumen (approximately 1.5 mm) is visible just to the left of center. Note the white fibrous connective tissue around the lumen. Because the stricture was too narrow to attempt bougienage and balloon catheters had not yet been developed when this case was seen, stricture resection was performed through a right thoracotomy. Resection of 1.5 cm of esophagus was performed. B, Endoscopic examination 4 weeks after esophageal resection and anastomosis. Mild narrowing of the lumen remains, but the endoscope was easily advanced. Note the suture tags and the esophageal lumen beyond the anastomosis site. The cat was asymptomatic. (From Tams TR: Esophagoscopy. In Tams TR, ed: Small animal endoscopy, St.Louis, 1990, Mosby-Year Book.)
history of anesthesia to suggest a reflux episode), biopsies should be done to differentiate a truly benign stricture from a malignant one. Brushings for cytologic examination are useful for rapid assessment while one waits for biopsy results.
If the lumen at the stricture site is extremely narrow, biopsy specimens should be taken before and after dilation. Also, a mass impinging on the outside of the esophagus may compress the esophageal lumen enough to cause a stricture effect. In this situation the esophageal mucosa will appear normal. The endoscopist will note that the esophageal walls do not readily distend in response to air insufflation. Additionally, it may not be possible to advance the endoscope through the narrowed area.Treatment
Treatment options for benign esophageal stricture include surgical procedures such as resection and anastomosis or patch grafting, bougienage, and balloon catheter dilation. In humans laser therapy and prosthesis has also been utilized. The success rate in animals treated with surgical procedures has been reported as less than 50% and in those treated with bougienage techniques as 50% to 75%. Surgical resection may result in restricture at the site of the anastomosis. Balloon catheter dilation is much more successful than either surgery or bougienage. The advantages of this technique over bougienage include decreased risk of esophageal perforation, longer symptom-free periods between procedures, and a smaller total number of procedures required to resolve the problem.
Bougienage
A wide variety of esophageal dilation devices whose diameters increase in stepwise fashion are available, including mercury-filled bougies and Pilling bougies. Bougies have either rounded tips or tapered ends with bases that are wider than the tips. The narrow tip is advanced to the stricture site under endoscopic guidance, and the wider area of the bougie dilates the stricture as the bougie is advanced through it. Care must be exercised to ensure that the bougie tip is directed into the stricture opening and not too far lateral to it. There is risk of perforation if the latter occurs. Other dilators that can be used in selected cases include endotracheal tubes (for cervical esophageal strictures in small patients) and the flexible endoscope itself.
The key to successful bougienage is to repeat the procedure as often as necessary to maintain improved luminal diameter. In many patients two to three bougienage procedures per week are necessary during the first several weeks of treatment before the desired effect is reached. After a stric-
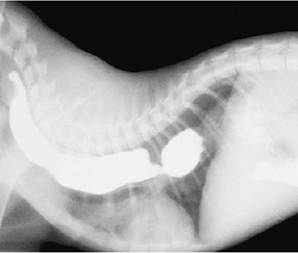
Figure 4-14 Barium liquid contrast radiograph from a 5-month-old kitten that had been regurgitating for 2 months. At the time the kitten was seen at a referral center, it was regurgitating solid food immediately after eating. The kitten had been anesthetized and neutered at a shelter at approximately 8 to 9 weeks of age. Note the proximal esophageal dilation and the narrowing of the dye column just caudal to the heart. Esophagoscopy confirmed a diagnosis of esophageal stricture, related to an internal fibrous band (i.e., there was no appearance of a narrowing due to external compression). Because of the kitten’s poor body condition at the time of presentation at the referral center, a gastrostomy tube was placed surgically so that nutritional support could be provided immediately. The esophageal stricture was managed successfully through a total of four ballooning procedures performed under endoscopic guidance. At 2 years of age there had been no stricture recurrence, and the cat continues to do quite well. (Courtesy Dr. Susan Hackner.)
ture has been forced open, the natural tendency is for it to narrow again as collagen is formed during epithelial healing.
Balloon Catheter Dilation
Balloon catheter dilation produces results superior to bougienage techniques. Advantages include a minimal chance of esophageal perforation, the ability to visualize more adequately the stricture dilation as the procedure progresses, and longer stricture-free intervals.A major advantage to balloon dilation is that it produces a radial stretch force rather than a longitudinal shearing force, as occurs with bougienage (Figure 4-15). In many patients only two to four balloon dilation procedures are required.
Balloon catheters are available commercially (Microvasive/Boston Scientific, Natick, MA 01760). The catheter is constructed of polyethylene, and

Figure 4-15 A diagrammatic representation of the shearing forces associated with bougienage compared with the radial forces associated with balloon dilation. (From Dawson SI et al.: Severe esophageal strictures: indications for balloon catheter dilation. Radiology 153:631,1984.)
the balloon consists of a specially treated polyethylene located peripheral to the central tubing.There is a radiopaque visible metal band at each end of the balloon. Various size balloons are available. A full set of balloons for use in animals would include balloons of the following inflated diameters: 6, 8, 10, 12, 15, and 20 mm. 25 and 30 mm—diameter balloon catheters are available for use in large dogs.
Smaller balloon dilators can be passed through the instrument channel of an endoscope with a 2.6-mm or larger instrument channel. However, since pediatric size human and veterinary use flexible endoscopes have a channel size of 2.0 to 2.5 mm, most procedures are done in animals by passing the balloon dilator alongside the endoscope. The balloon can be inflated with dilute iodinated contrast material or water. With the patient under general anesthesia, the catheter is advanced under endoscopic guidance and positioned with the middle part of the catheter centered in the stricture. During the first procedure a lateral thoracic radiograph is usually made, especially in situations in which the stricture site is very narrow, to confirm whether or not the balloon positioning is correct. If fluoroscopy is used, the stricture and its response as the balloon is dilated can be observed directly. The stricture is apparent as a narrowing or waist in the balloon. Fluoroscopy is certainly not necessary to perform the procedure safely, however, and in most cases it is not used.
Once positioned, the balloon is distended with water or dilute contrast medium, and the luminal pressure is monitored with the pressure gauge. This increased pressure is associated with effacement of the waist, indicating dilation of the stricture (Figure 4-16).A dilation time of 2 to 4 minutes at 40 to 45 psi seems to be adequate for stricture dilation in dogs and cats (initially a time of 2 minutes is used so that initial response can be determined). After dilation, the balloon is deflated and the catheter removed. Immediate postdilation endoscopy is recommended to ensure resolution of the stricture. Dilation periods of 4 minutes are usually used in cases in which frequent procedures have not yet successfully solved the problem.
Mild to moderate hemorrhage around the stricture site is a normal postdilation finding. If there is no hemorrhage, the stricture was not dilated to any significant degree. With a very aggressive dilation, long and fairly deep longitudinal splits may occur in the esophageal wall. It is generally best to act a little conservatively during initial dilation procedures so as to minimize the likelihood of perforation that could result from using too large a balloon. Usually 2 to 3 progressively larger balloons are used in sequence during each individual anesthesia. Because esophageal strictures tend to close down again fairly quickly after being dilated, two to three individual dilation procedures are routinely scheduled during the first 7 days. Subsequent procedures are scheduled based on patient response during the first 1 to 2 weeks.
Factors that help determine the number of balloon dilation procedures that will be necessary
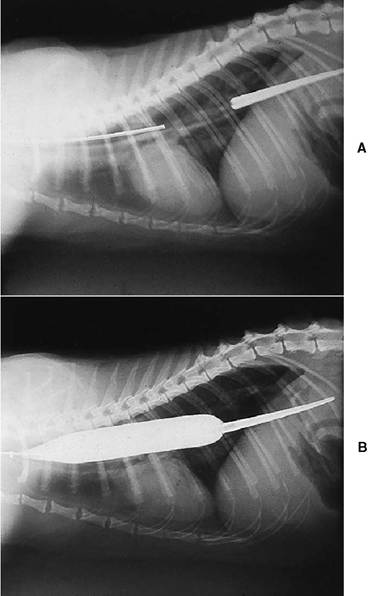
FIGURE 4-16 Radiographic appearance of a balloon catheter during an esophageal stricture dilation procedure. A, The balloon catheter is advanced under endoscopic guidance. The stricture is located over the base of the heart. The catheter’s soft, flexible radiopaque guide tip is visible in the stomach and distal esophagus. The radiopaque wire in the catheter shaft is clearly visible in the cranial and middle thorax. B, A fully distended balloon catheter with a diameter of 20 mm. The stricture has been fully dilated.
include severity and length of the stricture, number of strictures, and the ease of the initial stricture dilation. In general, tight strictures and those that were several millimeters long require more dilations than those of moderate severity and shorter length. Patients with multiple strictures tend to require more dilations than those with single strictures.
A stricture that has been present for longer than several months may become so fibrotic that it may not be possible to dilate the stricture with balloons. Therefore, once the presence of a stricture is confirmed, proper treatment should be instituted. A case in which an attempt to dilate a cervical esophageal stricture was not made until 9 months after it was diagnosed is illustrated in Figure 4-17. Surgery was required to remove the stricture.
After bougienage or balloon dilation is begun, intensive therapy for esophagitis is instituted. This includes ^-receptor antagonist therapy, metoclopramide, sucralfate suspension, and prednisone (0.25 to 0.5 mg/lb/day). Food, usually chopped canned consistency, is usually resumed later on the same day or on the following day. If there is severe esophageal damage, it might be necessary to place a gastrostomy tube so that adequate nutritional support can be given. Most patients eat well very soon after a dilation procedure, even if there is significant esophageal mucosal tearing.
Prednisone is used to decrease fibroblastic activity. Whether or not it really helps to decrease or prevent further stricture formation is controversial. I have observed patients in which an esophageal stricture developed despite aggressive therapy (famotidine, sucralfate, metoclopramide, and prednisone) for acute moderate to severe esophagitis that was diagnosed early in its course via endoscopy. This therapeutic regimen is given both to treat the existing esophagitis and, it is hoped, to decrease the likelihood of stricture formation. Unfortunately, this approach does not always work. Some specialists have begun to take the additional step of injecting intralesional triamcinolone with a Wang needle, under endoscopic guidance, after dilating severe esophageal strictures in an effort to further decrease fibroblastic activity. Endoscopy guided laser treatment used as an adjunct to ballooning is also being investigated.
It is emphasized that careful surveillance for development of a stricture is warranted in animals that are most at risk (e.g., those with anesthesia- related esophagitis and those that have recently vomited a large hairball). Esophagoscopy is the ideal procedure to monitor for progression or regression of esophagitis. Clinicians must recognize that once severe esophagitis is present, a stricture can form very rapidly.
The prognosis for resolution of an esophageal stricture disorder is excellent when balloon dilation is used. Sometimes mild permanent narrowing remains at the stricture site, but this is usually clinically insignificant. Cats and small dogs can manage well with an esophageal diameter of 1 cm or less if food consistency is limited to soft meals. A diameter of 1 to 1.5 cm is necessary in medium to large dogs. Many patients are eventually able to eat foods of normal consistency.