Immune-Mediated Ocular Diseases
Kathryn L. Wotman • Mary Elizabeth Lassaline • Mary Belle Glaze
This section describes immune-mediated ocular disease in large animals, beginning with a review of ocular immunology, followed by discussion of immune-mediated ocular diseases including immune-mediated keratitis, eosinophilic keratitis, and equine recurrent uveitis.
Except for the conjunctiva, the eye has no lymphatic drainage. Access of antigens to potentially reactive lymphoid tissue is also restricted by the avascularity of the cornea and the presence of selective blood-ocular barriers. As unlikely as immunologically mediated abnormalities may seem under these circumstances, immune-related inflammation remains a leading cause of blindness in the horse. Reports of immune-mediated ocular disease in ruminants are rare.
Ocular Immunology
The conjunctiva represents an extension of the mucosal immune system. A variety of immune cells can be found in the conjunctival epithelium and within the substantia propria, including intraepithelial CD8+ lymphocytes and mast cells, as well as aggregates of CD4+ T-helper (Th) cells and B lymphocytes, CD1+ dendritic cells, and macrophages.1 The conjunctiva processes ocular surface antigens with the help of regional lymph nodes. Antigen presentation is likely preceded by local tissue damage and release of inflammatory mediators that recruit inflammatory cells to the site. Under the influence of cytokines like interferon (IFN)-α, tumor necrosis factor (TNF)-α, interleukin (IL)-1, and IL-12 released by local and recruited cells, tissue dendritic cells process and carry host and pathogen molecules to regional lymph nodes to activate CD4+ Th cells. Stimulated lymphocytes migrate back to the conjunctiva (T cells) and lacrimal gland (B cells), where they participate in cell-mediated reactions and local production of IgA and to a lesser degree IgG, respectively.1-3
Because the globe itself is without lymphatic drainage, intraocular antigens must be processed at a distant site.
These antigens pass into the systemic circulation, preferentially stimulating the spleen as well as the bone marrow and other distant lymphoid organs. After 5 to 7 days, sensitized lymphocytes migrate back to the eye and localize within the uvea and limbal conjunctiva. As with those on the ocular surface, these immunologically competent cells are capable of antibody production and can participate in cell-mediated reactions. Further exposure to the same antigen can provoke an anamnestic response, endowing the uveal and limbal tissues with behavior comparable to that of a regional lymph node.4The intraocular immune response varies from that of a classic immune reaction, presumably to limit excessive inflammation within the eye. Anterior chamber-associated immune deviation (ACAID) is characterized by preferential stimulation of T suppressor cells that inhibit development of both CD4+ and B cells necessary in delayed-type hypersensitivity reactions and production of complement-fixing isotypes of antibody, respectively.1,5 Cells in the uvea and corneal endothelium also express Fas ligand (FasL), which limits inflammation through apoptosis of activated leukocytes entering the eye.1
Each of the four major types of immunologic reactions occurs within the eye.6 Type I (immediate) hypersensitivity is usually manifested as conjunctivitis, an acute local inflammatory reaction that follows IgE-mediated release of histamine, proinflammatory cytokines and chemotactic mediators from tissue mast cells, and synthesis of cytokines, leukotrienes, prostaglandins, thromboxane, platelet-activating factor (PAF), and kinins.7 These mediators of the IgE-mast cell inflammatory pathway increase vascular permeability, constrict smooth muscle, dilate blood vessels, and activate leukocyte chemotaxis and the complement cascade. Allergic reactions of the lids and conjunctiva undoubtedly occur in all domestic species.
Type II (cytotoxic/cytolytic) hypersensitivity is an antibody- mediated cytolytic reaction in which the antigen is a cell surface or basement membrane component.
Three basic effector pathways lead to cell destruction: (1) opsonization, with increased efficiency of phagocytic destruction; (2) antibody-dependent cellular cytotoxicity, inducing the release of enzymes capable of destroying cells and digesting basement membranes; and (3) lysis of immunoglobulin-bearing cells.8 Conjunctival damage resulting from autoantibodies directed against epithelial basement membranes is described in equine ocular pemphigoid.Type III (immune complex) hypersensitivity may share similar effector mechanisms with those described for cytolytic reactions, but antigen locale accounts for dissimilar disease manifestations in these two pathways.7 This immune complex reaction may explain the clinical signs of pemphigus foliaceus9 and the intraocular inflammation observed in horses after influenza vaccination or contact with infected animals.10 Antibody- mediated cell destruction has also been implicated in uveitis.6
Type IV (cell-mediated/delayed) hypersensitivity is an important factor in contact allergy of the lids and conjunctiva and may also play a role in ocular toxoplasmosis. The tissue destruction associated with herpetic keratoconjunctivitis in the horse has been attributed to a cell-mediated response.6 Increasing evidence implicates delayed hypersensitivity in the pathogenesis of equine recurrent uveitis.11,12 The reaction requires an initial antigen exposure that results in sensitization of antigen-specific T lymphocytes. Reintroduction of antigen induces interleukin production, with subsequent T-cell activation, proliferation, and cytokine production. Once activated by cytokines, recruited leukocytes display increased activity to many antigens.13
Allergic Blepharoconjunctivitis
In humans, several forms of allergic conjunctivitis are mediated by IgE, and histamine (H2) receptors have been discovered on the human ocular surface.14 The ubiquitous presence of H2 receptors in domestic animals implies a similar distribution2 and the potential for immediate hypersensitivity reactions of the eyelids and conjunctiva.
Affected animals demonstrate acute swelling of the eyelids and conjunctiva, accompanied by serous ocular discharge, mild conjunctival hyperemia, and pruritus. If the stimulus persists, multiple subconjunctival aggregates of lymphocytes appear as tiny semitransparent follicles within the conjunctival cul-de-sac. In contrast to bacterial conjunctivitis, crusting and purulent discharge are not typical of allergic conjunctivitis.
Diagnosis of allergic blepharoconjunctivitis is often presumptive, based only on careful and thorough elimination of all other causes of eyelid and conjunctival swelling. Trauma, orbital inflammation, neoplasia, mechanical irritants, conjunctival parasites, and other infectious agents (both ocular and systemic) should be considered. In support of an allergic etiology, conjunctival cytology may reveal eosinophils in response to mast cell degranulation.
The offending allergen may be difficult to identify. Insect stings and toxic plants (e.g., nettle) are possible causes, as are molds and pollens. Allergic conjunctivitis was described in 17 of 187 cows pastured adjacent to a field of blossoming cotton.15 A group of Angus-Holstein cattle demonstrated excessive lacrimation and ocular pruritus associated with familial allergic rhinitis. Several inhaled allergens have been incriminated, including capeweed, clover, dock, lucerne, pepper tree, pas- palum, wattle, ryegrass, sorrel, and fungal extracts.16 New feeds and certain drugs (e.g., oxytetracycline, penicillin, sulfonamides) may produce generalized urticaria, with accompanying eyelid and conjunctival edema.17 Similar findings have been reported in cattle with milk allergy. Agents that directly induce mast cell degranulation through osmotic or charge interactions include hypertonic saline, NSAIDs, thiopental, opiates, neuromuscular blocking agents, mannitol, radiocontrast agents, polymyxin B, and vancomycin.18 Occasionally, allergic conjunctivitis may be associated with a topical medication like neomycin.
Clinical signs exacerbate with continued application and diminish when the medication is discontinued.Ocular signs of hypersensitivity subside with removal of the offending allergen, but this is often impractical. Individual animals may be treated with a topical ophthalmic corticosteroid preparation, such as 0.05% dexamethasone ointment, to hasten resolution of swelling, redness, and discomfort. An agent with antiprostaglandin activity, such as oral or parenteral flunixin meglumine (Banamine®) at 0.5 mg/kg q12h, may be of benefit in the horse. Signs associated with urticaria respond to a decreasing regimen of oral prednisone or prednisolone, initiated at a dosage of 1 mg/kg once daily in the nonpregnant animal.19 Single parenteral doses of short-acting corticosteroids, epinephrine, or antihistamines have also been used with reported success in food animals.16
Ocular Manifestations of Immune- Mediated Dermatoses
Pemphigus foliaceus is the most common of the autoimmune skin diseases described in horses. Lesions are often first noted on the head and lower extremities but spread to other parts of the body with time. Vesicles, bullae, pustules, erosions, and crusting are commonly noted on the skin and mucous membranes, including the eyelids and conjunctiva. Pemphigus foliaceus, bullous pemphigoid, and recently pemphigus vulgaris have been described in the horse.20-25 Direct immunofluorescence reveals intercellular deposition of IgG and complement (C3) within the epidermis. Histopathology from biopsied lesions is reported to be more reliable, with findings of acantholytic cells with associated neutrophilic inflammation and intraepidermal pustules.26 In humans, a Welsh pony stallion, and recently in the equine muzzle skin, circulating autoantibodies to epidermal transmembrane proteins desmoglein 3 (Dsg3) and desmoglein 1 (Dsg1) have also been demonstrated, which leads to acantholysis, vesicle formation, and epidermal clefting.25-27
Ocular manifestations of pemphigus may include ulceration or crusting of the eyelids, mucoid ocular discharge, and conjunctival hyperemia with erosions.
Corneal ulceration may result from mechanical trauma to affected eyelids and conjunctiva or may be a primary manifestation of disease, as has been reported in humans and a Welsh pony stallion with pemphigus vulgaris.24,28 Diagnosis is based on clinical findings, cytology, histopathology, and positive immunofluorescence of affected skin. See the discussion of immune-mediated dermatologic disorders for therapeutic recommendations and prognosis in Chapter 53.Other immune-mediated diseases, such as systemic lupus erythematosus (SLE) or cutaneous lupus erythematosus (CLE), occur infrequently in the horse but can affect the face and eyelids.29,30 In addition to skin lesions, vasculitis may manifest by hemorrhages in mucous membranes, including the conjunctiva.20,29
Eosinophilic Keratoconjunctivitis
Eosinophilic keratoconjunctivitis (EK) is an inflammatory condition of the cornea and/or conjunctiva that can present as unilateral or bilateral ocular disease in the horse. The seasonality typically noted with EK, with a predominance of cases in one study noted during June, July, and August, suggests an environmental etiology, but the specific cause of the disorder is unknown.31 Studies have suggested contributing factors, including climate variables (temperature, rainfall amounts, humidity levels); sex predisposition, with females being overrepresented in one study; and possible causative effects of certain types of feed.31 As the name suggests, eosinophils on conjunctival or corneal cytology are diagnostic.31-35 Recurrence of signs is
y.gy, g 35 g not uncommon in subsequent years.35
■ Clinical Signs Clinical signs of mild to severe blepharospasm, epiphora, characteristic caseous mucoid ocular discharge, conjunctival hyperemia, and chemosis are typically noted at the onset of disease. Corneal lesions typically appear as raised white or pink corneal plaques. The plaques may be surrounded by corneal edema, with vascularization extending toward the ulcer and/or plaque from the limbus. Progression to corneal ulceration that extends from the limbus axially is often noted first in the ventromedial cornea quadrant underlying the third eyelid.31-35
■ Diagnosis Diagnosis is based on clinical signs and cytologic findings of predominantly eosinophils on corneal or conjunctival scrapings and may include segmented neutrophils, mast cells, plasma cells, and lymphocytes. Differential diagnoses include mycotic and/or bacterial keratitis, onchocercal keratoconjunctivitis, neoplasia, foreign body granuloma, traumatic keratitis, squamous cell carcinoma, and calcific corneal degeneration.36-39
■ Pathophysiology The eosinophilic inflammation found in the cornea and conjunctival surfaces suggests a type I or type IV allergic reaction. Although the inciting allergen has yet to be elucidated, parasites such as Onchocerca or Habronema spp. are often implicated, but neither has been specifically identified in a case of EK.31,38 One proposed mechanism for EK is an allergic or inflammatory response to long-term use of ivermectin as an anthelmintic, triggering the complement cascade and cellular chemotaxis in patients with ocular oncho- cerciasis.33 A recent case series of a Standardbred broodmare farm with 19 affected mares described environmental management with minimal medical intervention, including specifically fly control, as a key to decreasing incidence of disease, time to resolution of disease, and the number of recurring cases.34 This suggests that an environmental allergen that may be associated with flies themselves or transferred by flies stimulates the type I allergic reaction. Similarities to vernal keratoconjunctivitis in humans suggest that eosinophil-granule major basic protein may play a significant role in the equine disease, inhibiting corneal epithelial migration and protein synthesis and promoting collagen degeneration.40 Eosinophil-derived collagenase also has been reported to degrade type I collagen, the predominant collagen in the cornea.32
■ Treatment and Prognosis Given the mechanism by which EK is believed to persist (i.e., a toxic effect of eosinophilic major basic protein on the corneal epithelium leading to chronic corneal ulceration), the mainstay of treatment of EK should be prophylactic against secondary infection of corneal ulcers, including topical antibiotic therapy with a broad-spectrum drug such as ofloxacin 0.3% solution or neomycin polymyxin B bacitracin ophthalmic ointment, and in areas where fungal keratitis is prevalent, a topical antifungal as well. Treatment with immunosuppressive drugs such as prednisolone acetate or cyclosporine, although historically used to treat EK in horses, is not recommended due to the risk of infection, as well as complications associated with chronic topical steroid use.31,33,39 Eosinophilic keratoconjunctivitis lesions remodel with minimal corneal scarring, but mean duration of treatment in one series of patients was 64 days (range of 45 to 106 days).33 Use of topical NSAID preparations may increase the severity of clinical signs of EK in horses because of potentiation of leukotrienes, the primary promoter of eosinophilic inflammation, and thus these drugs are not recommended to treat EK.32 Medical management and prognosis were recently evaluated in horses diagnosed and treated in the Mid-Atlantic United States and revealed an average time to resolution of 3.7 months.35 Treatment in some horses included use of tapering doses of systemic dexamethasone starting at a rate of 0.04 mg/kg PO for 1 day,
0. 03 mg/kg for 2 days, and 0.02 mg/kg once daily for 3 to 5 days.35 A group of horses evaluated in the study was also treated with oral cetirizine, an H1 antagonist that may be useful in decreasing the migration and adherence of eosinophils.35,41 Horses treated with oral corticosteroids had a shorter time to resolution when compared to horses that were not given oral corticosteroids. This finding, combined with the risk of secondary corneal infection with topical steroids, suggests that systemic rather than topical corticosteroids should be used to treat EK. Treatment with oral cetirizine did not decrease time to resolution of ocular disease, but during the follow-up period these horses were significantly less likely to have recurrence of disease (1 of 13 horses [8%] had recurrence with cetirizine compared to 8 of 14 [57%] without cetirizine).35 Excision of the corneal plaques by superficial keratectomy appears to enhance healing, attributable to removal of the eosinophil-granule major basic protein.32,33
Immune-Mediated Keratitis
Nonulcerative Keratitis
Chronic nonulcerative corneal opacities that vary in color and depth within the cornea without overt signs of discomfort or intraocular inflammation have been described, and they can be a diagnostic and therapeutic challenge due to difficulties in obtaining diagnostic samples from a nonulcerated cornea.42-45 In a report of 19 horses ages 5 to 11 years diagnosed with nonulcerative keratitis, 11 horses had clinical signs for more than 12 months before referral.42 Nonulcerative keratitis in this report was described as immune-mediated keratitis (IMK), which comprised three distinct clinical entities classified as superficial, deep/mid-stromal, or endothelial, based on the location of the corneal pathology. Superficial keratitis was characterized by a superficial white to yellow infiltrate with diffuse mild to moderate vascularization. Deep/mid-stromal lesions were described as more diffuse, with denser cellular and vascular components. A deep cellular infiltrate with mild corneal vascularization and variable degrees of diffuse corneal edema were typical of endothelial keratitis. Intraocular inflammation was not a feature of the disorder, regardless of lesion location.42 Differential diagnoses include stromal abscess, EK, bullous keratopathy, subepithelial herpes keratitis, nonulcerative keratouveitis, and subepithelial keratomycosis (SEK). The infiltrates seen with SEK lie beneath the epithelial layers and may appear as punctate lesions or more geographic opacities that respond favorably to antifungal treatment.43 Unlike what is typically noted in the equine eye with lesions due to fungal infections, SEK does not have significant blepharospasm or intraocular inflammation as a feature.43
An immune-mediated pathogenesis has been theorized for IMK, based on histopathologic characteristics and response to immunosuppressive therapy. Lesion appearance and description has varied, but typically within the United States, changes are described based on depth: superficial, deep/mid-stromal, and endothelial. Response to treatment and prognosis vary depending on the location of the infiltrate.44 Regardless of lesion depth, histopathology reveals a predominantly lymphocytic-plasmacytic infiltrate, with stromal fibrosis or necrosis and vascularization. Three of five horses tested were seropositive for Leptospira spp. in one study.42 Presumably the immune system is reacting to a self-antigen, antigens of a foreign protein, or an infectious agent within the cornea. Even though infectious agents have not been consistently documented in this particular disorder, immunologic cross-reaction with self-antigens (i.e., molecular mimicry) may occur, as described with leptospiral organisms or their DNA in the equine cornea.46,47 Keratectomies from 10 horses diagnosed withsu- perficial IMK showed a predominantly cell-mediated inflammation with cytotoxic and Th cells being the most common cells noted.48 Local immunoglobulin was also identified in the corneal samples, but this could not be directly associated with a systemic humoral response, leaving the role of this arm of the immune system in question as to the pathogenesis of IMK.48
Owing to the frequency at which the abnormal equine cornea is afflicted with an infectious agent (bacterial, fungal, viral), diagnostic samples (cytology, culture) should be considered prior to starting therapy with immunosuppressive agents, particularly given that typically no independent confirmation of the diagnosis of IMK, nor microbiological samples ruling out an infectious etiology, are available when the diagnosis of IMK is made. Concurrent therapy with topical antibiotics and antifungals may be warranted. Lesions of superficial stromal keratitis have been described as able to be controlled with long-term topical dexamethasone and/or cyclosporine, with the goal of reducing frequency of the topical glucocorticoid.42,45 Tacrolimus is a more potent immunosuppressive agent than cyclosporine and could potentially be used topically to aid in decreasing the activity of T cells, but its efficacy as a sole treatment for IMK has yet to be supported with empirical results.44 Topical ophthalmic NSAIDs (e.g., diclofenac, bromfenac, flurbiprofen) may be a reasonable alternative to topical steroids, particularly for long-term use in some cases. A similar chronic therapeutic regimen may be used in superficial and mid-stromal keratitis45; however, topical corticosteroids may be less effective than cyclosporine in the deeper stromal disorder and, when used in combination long-term, may offer improvement in clinical signs.42 Lesions in 4 of 11 horses with superficial stromal IMK were treated by superficial keratectomy and conjunctival grafting; lesions resolved in all four horses without the need for ongoing medication, suggesting that surgical removal of the inciting antigen in addition to providing a direct blood supply may stop the inflammatory process.42 Keratectomy followed by a conjunctival graft was curative in one horse with mid-stromal IMK.42 Response to antiinflammatory agents varies in patients with endothelial keratitis, resulting from differences in pathogenesis. Only two of four horses were controlled with constant topical dexamethasone and cyclosporine in a retrospective study from Gilger and colleagues.42 In contrast, horses with endothelial IMK in the United Kingdom usually respond rapidly to a glucocorticoid applied topically 2 to 3 times per day and complete resolution of clinical signs is possible.43 In general, due to the deep location within the cornea, endothelial IMK carries a poor prognosis for response to treatment and often progresses.44 Although retention of vision is likely in most cases of nonulcerative keratitis, long-term or even lifelong therapy is required to control the corneal disease.
The therapeutic goal for IMK is disease resolution, or at minimum slowing progression of the corneal changes and decreasing the number of medications and/or frequency of application needed to control the disease. A surgical alternative to a keratectomy of all or a portion of the affected cornea is implantation of an episcleral cyclosporine delivery device, which has shown a positive response in a report of 19 horses with IMK.49 Keratitis was best controlled (i.e., horses were on no more than one medication) in 14 horses with either superficial IMK or endotheliitis, followed for about 6 months. However, in three horses diagnosed with mid-stromal IMK, keratitis was not controlled without additional medical and/or surgical therapy during the 5-month follow-up period after episcleral implant placement. The episcleral implant appears to reduce and in some cases may eliminate altogether the need for other topical medical therapy in horses that have previously responded to topical cyclosporine. Owners should be counseled that the implant likely lasts 1 to 1½ years and the procedure may have to repeated.49
Equine Recurrent Uveitis (Periodic Ophthalmia, “Moon Blindness”)
■ Definition and Etiology Equine recurrent uveitis (ERU) is distinguished by a pattern of intraocular inflammation in which recurring episodes of acute uveitis are separated by periods of clinical quiescence. Inflammation of the iris and ciliary body (anterior uveitis or iridocyclitis) predominates in the early stages; repeated episodes damage the cornea, lens, vitreous, retina, and optic nerve. A more insidious form of ERU characterized by persistent low-grade inflammation occurs in the Appaloosa and Draft breeds of horse.
Equine recurrent uveitis is a leading cause of blindness in the horse and mule. Although the exact prevalence is unknown, estimates as high as 10% to 25% have been reported.50,51 The financial impact on the equine industry is estimated at US$100 to $250 million annually as a result of the effects on performance and the costs of veterinary care.52
Despite extensive clinical research, the specific cause of ERU is still unknown. The pathogenesis is immune mediated, and characterization of T-lymphocyte populations in affected horses documents a delayed hypersensitivity reaction as the basic immunologic mechanism underlying the recurrent inflammatory episodes.12 Identification of the triggering antigen has proved more elusive, suggesting that the disease does not result from persistence of or repeated exposure to a single antigen, but rather to a variety of circulating antigens or native ocular antigens. L. interrogans serovar pomona is the most frequently incriminated infectious pathogen,51 but diversification of T-cell responses to a particular antigen or group of antigens over time may result in evolution of the immune response to encompass endogenous ocular self-antigens.9,53
■ Clinical Signs The ocular lesions observed in ERU vary depending on the severity and duration of the disease. ’’’ ERU can occur at any age, but the initial uveitis episode frequently occurs in horses 4 to 8 years of age. Acute episodes are painful, characterized by blepharospasm and excessive tearing. Affected eyes are often described by owners as “red”

FIG. 39.15 Active uveitis characterized by hypopyon, pupillary irregularities secondary to posterior synechiae, pigment adherent to anterior lens capsule, and a dull tapetal reflection.
and/or “cloudy” because of changes in the conjunctiva, cornea, anterior chamber, or vitreous. Dilation of subconjunctival vessels near the limbus, termed ciliary flush, may intensify the generalized conjunctival hyperemia. As corneal endothelial function decreases, diffuse corneal edema gives the eye a bluish-white appearance. The cornea may also exhibit peripheral circumferential vascularization, cellular precipitates on its inner (endothelial) surface, and linear stromal opacities.
Increased uveal vessel permeability causes the aqueous humor to appear cloudy after influx of plasma proteins (flare), inflammatory cells (hypopyon), erythrocytes (hyphema), or fibrin into the anterior chamber (Fig. 39.15). The iris often appears edematous and lackluster or “muddy.” A change in iris color may be noted in breeds with lightly colored eyes, changing from blue to yellow or green in response to uveal edema, vascular congestion, and cellular infiltration (see Color Plate 39.10). Prostaglandins and other inflammatory mediators cause pupillary constriction, favoring the formation of adhesions between the iris and lens (posterior synechiae) that distort the pupillary shape. Even without adhesions, the inflamed iris responds poorly to mydriatic agents. IOP is usually decreased because of diminished aqueous production by the inflamed ciliary body, but intermittent IOP elevations can occur.56 The ciliary body can also deposit cellular exudates within the anterior vitreous, creating an opacity within the pupillary space that may be mistaken for cataract.
Active chorioretinitis causes dullness and loss of detail in affected tissues. Retinal detachment may follow choroidal exudation. Multifocal depigmented or hyperpigmented foci on either side of the optic disk are the sequelae of chorioretinitis (“chorioretinal scars”), commonly referred to as peripapillary “butterfly” lesions (Fig. 39.16).
Intraocular damage increases each time inflammation recurs. Permanent corneal opacity caused by edema results if the corneal endothelium is severely compromised. Chronic recurrent uveitis is characterized by widespread posterior synechiae, iris depigmentation or hyperpigmentation, and iris atrophy. The anterior chamber may appear shallow if aqueous trapped in the posterior chamber by extensive iris-to-lens adhesions causes the iris to balloon forward (iris bombe). Most lens changes occur weeks or months after uveitis begins. Abnormalities may range from pigment flecks on the anterior lens capsule (Fig. 39.17) to dense cataracts (see Color Plate 39.2). Lens luxation often follows degeneration of the lens zonules and vitreous. Retinal detachment may also follow vitreous liquefaction or may result from traction by fibrous tissue bands within the vitreous. If retinal degeneration is substantial, the optic
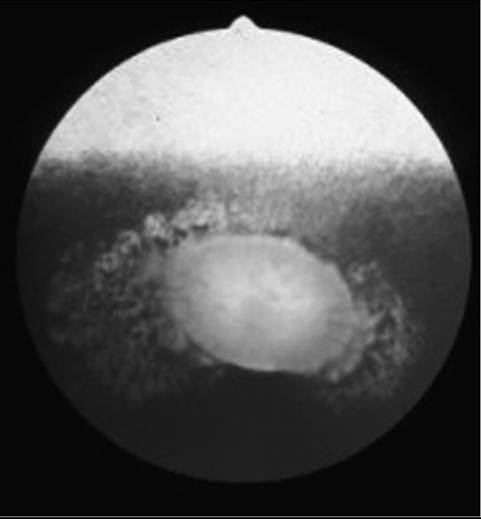
FIG. 39.16 Fundus adjacent to the optic disk takes on a mottled appearance as a result of pigment migration after previous chorioretinal inflammation from recurrent uveitis. Because of the shape, such lesions are sometimes referred to as “butterfly lesions.”
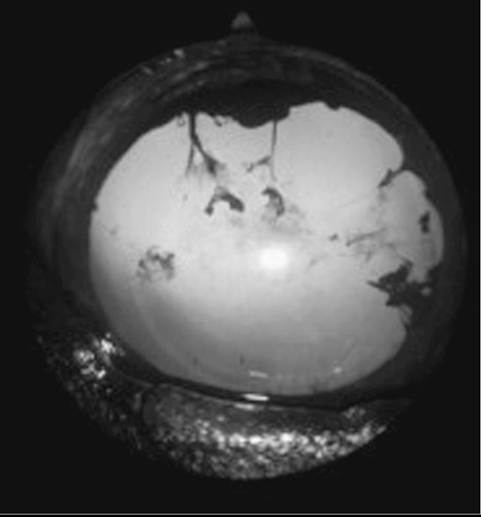
FIG. 39.17 Prior episodes of anterior uveitis are indicated by pigmented remnants on anterior lens capsule and thin adhesions of iris to lens (posterior synechiae). Pupil is pharmacologically dilated.
disk atrophies (Fig. 39.18). Permanent hypotony is followed by shrinkage of the globe (phthisis bulbi). Conversely, chronic uveitis may result in secondary glaucoma (see Color Plate 39.8). The combination of these acute and chronic ocular lesions determines the degree of vision loss in the affected animal.
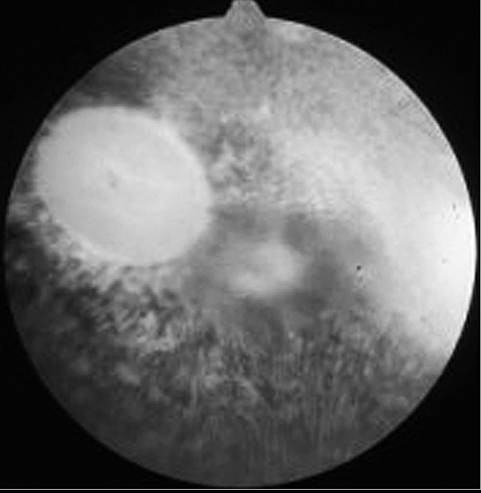
FIG. 39.18 Disk pallor and nontapetal depigmentation accompany an adjacent dark gray preretinal exudate in a horse with chronic active recurrent uveitis. This patient had poor vision.
Equine recurrent uveitis may be accompanied by transient and variable inflammation of the pineal gland.57-60 Similar pineal inflammation has been reported in experimentally induced recurrent uveitis in laboratory animals.
■ Diagnosis Not every case of uveitis in the horse qualifies as ERU. Diagnosis is based on a chronic, recurrent history of intraocular inflammation and the presence of characteristic ocular lesions. In cases where the history is unknown but recurrent disease is suspected, at least several of the following indicators of previous inflammation should be observed before a presumptive diagnosis of ERU is made: corneal edema or vascularization, synechiae (typically posterior), iris color change, corpora nigra atrophy or “polishing,” lens capsular pigmentation, cataract, lens luxation or subluxation, vitreous opacities or traction bands, retinal detachment, or peripapillary scarring.50 Other causes of a red and painful eye that can mimic acute ERU include conjunctivitis, corneal ulceration, corneal stromal abscessation, keratouveitis, and glaucoma.
Serologic testing of paired serum samples for Leptospira spp. or other infectious agents incriminated as causes of equine uveitis (see Table 39.2) may contribute to a diagnosis of ERU, but negative titers neither exclude the diagnosis nor eliminate leptospirosis as a contributing factor to the disease.61,62 Acute leptospiral infections are characterized by high-titer seroreactiv- ity to at least one serovar by the eighth day63; the titer usually falls with time, but seroreactivity may persist for many years. Some authors suggest that a leptospiral titer of 1 : 400 or higher is of clinical importance, particularly for L. interrogans serovar pomona.5 A higher titer in the aqueous than in the serum is indicative of intraocular antibody production and further supports a leptospiral cause for the uveitis.64 Onchocerca microfilariae may be identified in conjunctival biopsies, although detection of live microfilariae does not necessarily indicate a causal relationship for uveitis.65,66 Equine leukocyte antigen (ELA) typing may help determine susceptibility to ERU.67
Histopathologic lesions of the ciliary body considered pathognomonic for ERU include the presence of a thick, noncellular hyaline membrane adherent to the nonpigmented epithelium (NPE) and the presence of eosinophilic linear cytoplasmic inclusion bodies within the NPE.68,69 Clusters of lymphocytes and plasma cells also accumulate in the posterior iris, in the ciliary body, near the ora ciliaris retinae, within the choroid, and near the optic nerve head.52,70 Dense bundles of fibrils coupled with necrotic cells and mononuclear inflammatory cell infiltrates characterize the changes within the vitreous.71
■ Pathophysiology Breed has been established as a risk factor for ERU. In a 1988 retrospective study of more than 16,000 equine patients at Cornell University, researchers determined that the Appaloosa had a significantly higher risk of developing uveitis than Thoroughbreds.72 A subsequent New York field study substantiated the breed predilection, concluding that the Appaloosa was 8.3 times more likely to develop uveitis than all other breeds combined.51 Within the Appaloosa breed, those with overall light hair coats and focal dark spots are more likely to develop ERU than horses with a dark, basic coat pattern and a light “blanket” over the rump.52 Trotters and warmbloods were overrepresented in a report of 130 ERU-affected horses in Germany.73 Of 669 mares included in a serologic study of leptospirosis, significantly fewer positive titers were found in Thoroughbreds and Standardbreds.74
In humans, an immunogenetic predisposition to certain types of uveitis has been linked to the major histocompatibility complex (MHC), a closely aligned cluster of genes designated as the human leukocyte antigen (HLA) region located on a single chromosome.75 Similar genetic loci occur in the horse, and the gene products are referred to as equine leukocyte antigens (ELAs). Products of these genes are glycoproteins found either on most nucleated cells (class I antigens) or restricted to accessory cells such as monocytes or macrophages (class II antigens). The immunoregulatory role of the MHC is especially important in discriminating self-peptides from those of nonself origin. Recent studies have shown an increased risk of uveitis linked with the MHC class I haplotype ELA-A9 in a group of German Warmblood horses.67 As proposed in studies of human HLA-associated uveitis, cross-reactivity between selfantigens and ELA cell surface peptides could explain an inadvertent immunologic attack on normal cells.76,77
Experimental findings in ERU patients indicate that a T cell-mediated autoimmune mechanism underlies the recurrent episodes of inflammation. T lymphocytes are the predominant cell type to infiltrate the anterior uvea,11,70 choroid,78 and vitreous79 of horses with ERU, and affected horses demonstrate cell-mediated immunity to retinal autoantigens and peptides.79-81 B lymphocytes have been reported primarily in retinas from horses seroreactive for L. interrogans serovar pomona, suggesting that Leptospira-associated ocular inflammation may be a distinct subset of equine uveitis.82 Equine ciliary body epithelium may play a role in recruitment and activation of leukocytes through expression of a chemotactic cytokine (chemokine),83 although in the normal ocular microenvironment, ciliary body pigment epithelium suppresses T-cell activation by direct cell contact and the action of unidentified molecular mediators.84 Analysis of messenger RNA (mRNA) collected from horses with uveitis demonstrates elevated levels of IL-2 and IFN-γ, indicating a Th1 response in the disease process.85 In the absence of bacteria or viruses, this Th1 response by CD4+ uveal T lymphocytes suggests a delayed-type hypersensitivity (DTH) reaction to self-antigens or sequestered antigens in the uveal tract.12,86 In contrast to the ocular T-lymphocyte population, systemic lymphocytes of ERU-affected horses do not exhibit a Th1 response.12 The expression of a deviant MHC class II antigen on resident ocular cells (e.g., Muller, retinal pigment epithelial) suggests that aberrant immune regulation may also play a role
in ERU.11,87
Aqueous and vitreous immunoglobulin levels have been used to characterize immunologic responses within ERU-affected eyes. Using radioimmunoassay, an early study found that aqueous levels of IgG, IgM, and IgA were 50% to 120% greater in diseased eyes than in normal controls, but that the IgG/albumin ratio suggested leakage of protein through an impaired blood-aqueous barrier rather than intraocular antibody synthesis.88 Subsequent reports support local ocular antibody production but disagree on the dominant immunoglobulin in ERU-affected eyes. Wagner and colleagues89 found selectively increased IgA levels in the vitreous of affected horses; Eule and colleagues90 reported substantial IgM titers in 79.6% of intraocular samples from ERU-affected eyes. In contrast to the intraocular immunoglobulins, there are no significant differences in serum immunoglobulin concentrations between healthy and ERU-affected horses.89’90
Both exogenous and endogenous antigens have been proposed as stimuli for these basic immunologic responses. One theory suggests that an infectious agent such as L. interrogans (or another, perhaps noninfectious, exogenous antigen) causes the initial iridocyclitis. Sensitized immunocompetent cells enter the uvea during this first inflammatory episode, imparting immunologic memory that is specific for the inciting antigen. Subsequent challenge of these cells by the immunogen causes recurrence of the inflammatory reaction.6’91 However, although some reports suggest persistent infection as the cause of ERU,92 the premise of an infectious agent that exclusively induces and maintains ERU through a classic anamnestic response does not fully account for the disorder’s clinical course and response to therapy.
The role of leptospiral infection in ERU has been studied extensively in recent years. All major serogroups of L. interrogans have been identified in the horse and implicated as initiating factors in ERU.51’62’93-96 In a report of 130 ERU cases in Germany, 58.8% demonstrated positive serum titers to leptospirosis, an incidence 7 to 10 times higher than the control population.73 Anti-Leptospira antibodies have been found in the serum, tears, aqueous humor, and vitreous of infected horses.62’94’9' 99 Wollanke and colleagues99 reported positive serum antibody titers to Leptospira serovars in 25% (24 of 97) of normal-eyed horses and 22% (50 of 227) of ERU-affected horses’ but only the ERU-affected animals had positive antibody titers in the vitreous.99 Leptospiral organisms have been cultured from the aqueous and vitreous of ERU-affected horses.61’62’96’100’101 However, in one study, Leptospira was not frequently detectable in fixed ocular tissues of horses affected with ERU when using traditional immunohistochemical and real-time PCR techniques.102 In another study, there were no differences in bacterial DNA detection or in serum or aqueous humor anti-Leptospira antibody production between clinically normal horses, horses with ERU’ and horses with ocular inflammation not associated with ERU in the southeastern United States.103
Horses seropositive to L. interrogans serovar pomona are reportedly 13.2 times more likely to have signs of uveitis than seronegative horses.51 Ocular signs during the acute infection are usually subtle or absent, but overt ocular inflammation develops months to years later.104-107 Risk factors for equine leptospirosis include rodent and wildlife exposure, proximity to ponds and rivers, a dense equine population on site, and increasin ae 74’108’109
Iiicieasiiigage.
Although direct Leptospira-mediated injury to the eye cannot be ruled out in the pathogenesis of ERU’ a growing body of evidence instead links leptospiral infection with autoimmune responses to ocular tissue components. Complement-binding anti-Leptospira antibodies capable of cross-reacting with equine corneal tissue and lens have been found in the tear film and aqueous humor of horses with leptospirosis.97’98’110 These antibodies bind corneal epithelial cells, activating complement and initiating tissue damage, a mechanism replicated in tissue culture.111 A leptospiral protein epitope that shares antigenic determinants with the equine cornea and lens has been found in bacterial homogenates,46 and a DNA fragment of several serovars of L. interrogans was determined to encode a 90-kilodalton protein that cross-reacts with equine corneal proteins.47’112 Novel leptospiral lipoproteins, identified as LruA and LruB’ stimulate local intraocular IgA and IgG production and also cross-react with equine ciliary body, lens, and retina.113 Immunohistopathologic examination has also demonstrated leptospiral cross-reactivity with iris pigment epithelium and retina from horses with ERU.82’114 This antigenic relationship between Leptospira spp. and equine ocular tissues supports the concept of molecular mimicry as a contributing factor in ERU; exposure to exogenous antigens that share molecular structural sequences with equine self-antigens initiates an autoimmune response.10
Toxoplasmosis, brucellosis, salmonellosis, streptococcal hypersensitivity, E. coli, R. equi, borreliosis,115,116 intestinal Strongylus, and onchocerciasis have also been implicated as causes of ERU’ with no consistency in culture or serology results in affected horses.51 Viruses suspected of a role in ERU include equine influenza virus’ equine herpesvirus (EHV-1’ EHV-4)’117 equine arteritis virus, and possibly equine infectious anemia.50,52 More recent studies on vitreous and serum samples from affected horses question the role of B. burgdorferi, Borna disease virus, and Toxoplasma in ERU.118’119
Both humoral and cell-mediated hypersensitivities have been implicated in the lesions of ocular onchocerciasis. Immuno- electrophoretic studies have demonstrated an influx of IgG and complement (C3) into the tears of affected horses in response to larval death.120 The resulting chemotaxis of mast cells, eosinophils, and lymphocytes perpetuates the inflammatory response and facilitates destruction of the parasite. Human patients with ocular onchocerciasis demonstrate conjunctival infiltration by CD3+ T lymphocytes and increased expression of class II MHC antigens in conjunctiva and iris’121 as well as deficiencies in suppressor T-cell function that may interfere with the normal regulation of antibody function.122
In addition to the role of infectious agents in the pathogenesis of ERU’ autoimmunity may occur when a normally sequestered component is exposed to lymphoid cells or when the antigenicity of a component increases as a result of a structural alteration.123 Several endogenous ocular proteins, including retinal soluble antigen (S-antigen, or S-Ag), interphotoreceptor retinoid- binding protein (IRBP)’ cellular retinaldehyde-binding protein (CRALBP)’124 and uveal melanin-associated proteins, are known to induce uveitis in various animal models.125-128 Clinical studies also implicate these potent autoantigens in the pathogenesis of some forms of human uveitis.129-131 An autoimmune phenomenon in response to damaged uveal tissue has been proposed in the pathogenesis of ERU.132 The isolation of S-Ag in the horse and the subsequent finding of anti-S antibodies in the aqueous humor and vitreous of horses with uveitis support the theory that this species is similarly capable of local production 7981133 of antibodies to normally sequestered autoantigens.'9-81’133 Experimental uveitis with features similar to spontaneous ERU has also been induced in horses after injection of IRBP in complete Freund’s adjuvant.78 Autoantibodies to S-Ag and IRBP were found in 72% of vitreous specimens from horses with uveitis.79 A more recent equine study concluded that retinal S-Ag is a weaker autoantigen than IRBP; T and B cells were activated after immunization with S-Ag, but only one in five horses developed uveitis or demonstrated inflammatory cell infiltration of the uveal tract.134 Because the retina and NPE of the ciliary body originate from neuroectoderm, it is even possible that ciliary body damage may release an S-like antigen or another uveitogenic substance.135 Evidence suggests that response to S-Ag is predominantly T-cell dependent.136
Verma and colleagues113 proposed a link between leptospiral cross-reactivity and the release of other ocular autoantigens, based on strong IgG and IgA responses to LruA and LruB lipoproteins in uveitic eyes but not in companion sera. The early phase of ERU may involve production of non-complementfixing antibody and non-DTH T lymphocytes specific for LruA and LruB. The antibodies and cells react with the leptospiral lipoproteins, initiating a process that ultimately liberates IRBP and other ocular autoantigens.
The concept of “epitope spreading” has been offered as an explanation for the relapsing character of ERU.137 The theory proposes that after destruction of an initial target, the immune response spreads from the first autoantigenic determinant to others not previously recognized by the immune system.138-139 Active uveitis subsides as regulatory cells suppress the inflammation, recurring as the immune response shifts to an epitope of the same autoantigen (intramolecular spreading) or a completely different autoantigen (intermolecular spreading). A recent 22-month study of peripheral T-cell reactions in 8 horses with spontaneous ERU demonstrated intramolecular shifts to different S-Ag-derived (6 of 8) or IRBP-derived (5 of 8) epitopes and intermolecular shifts in all horses, spreading from IRBP-derived to S-Ag-derived peptides (5 of 8) or vice versa (3 of 8).137 A shift of the immune reaction could be correlated to new uveitic episodes in 10 of 14 relapses that occurred during the observation period. The confounding factor in this theory is the shifts in immune response observed during quiescent stages, perhaps to minor uveitogenic epitopes that fail to result in overt inflammation or as part of an unknown regulatory or protective function of these T-cell clones.
Regardless of etiology, the ocular inflammatory process may attract other reactive lymphocytes to the eye. During primary uveitis, only 10% of the ocular immunoglobulin-secreting cells are specific for the inciting antigen. The remaining cells produce antibodies against immunogens that may not have entered the eye but with which the host had previous contact. As a consequence, the eye may develop recurrent inflammation after systemic exposure to any one of multiple antigens. It is therefore conceivable that subsequent episodes of uveitis may differ etiologically, creating a perplexing clinical picture.140
■ Treatment
ACTIVE INFLAMMATION. Reduction of intraocular inflammation is the primary therapeutic objective in acute uveitis. Preservation of vision depends on successful management at this stage, when sight-threatening sequelae are minimal. If a specific cause for the uveitis is identified, it is also targeted pharmacologically. In most cases, symptomatic therapy combines corticosteroids, NSAIDs, and mydriatic or cycloplegic agents. Nonspecific suppression of T-lymphocyte activation with cyclosporine implants141 and surgical removal of T cells and, potentially, organisms from the eye by core vitrectomy142 are recent innovations aimed at preventing recurrence of disease.
No therapy is indicated in nonpainful eyes with lesions of chronic end-stage uveitis. Those eyes that remain painful or do not respond to therapy are candidates for enucleation or evisceration, followed by silicone prosthesis implantation in the orbit or sclera, respectively.
CORTICOSTEROIDS. The severity of the uveitis dictates the routes and frequency of corticosteroid administration. Although topical therapy is most often used, efficacy is limited by the agents' relatively short contact time with the eye. Therefore topical corticosteroids must be applied three or four times daily, even in eyes with mild clinical signs. In more severe uveitis, topical preparations should be combined with other routes of therapy. A subpalpebral lavage system should be considered when frequent application is indicated (see the Bacterial Keratitis in Horses section earlier).
Either ophthalmic solution or ophthalmic ointment is acceptable for topical use in the horse. Prednisolone acetate 1% suspension has excellent intraocular penetration and is considered the drug of choice. Potent dexamethasone preparations, 0.1% solution or 0.05% ointment, are also effective. In general, therapy should be continued for at least 2 weeks after clinical signs have resolved. Ideally, that assessment includes an objective IOP measurement to ensure resolution of ciliary body inflammation and dysfunction.
The subconjunctival injection of a repository corticosteroid preparation is an alternative or supplement to frequent topical therapy. Triamcinolone acetonide 4% suspension is effective for 1 to 3 weeks when injected in a 0.5- to 1-mL volume (20 to 40 mg) beneath the superior bulbar conjunctiva. Subconjunctival injection of methylprednisolone acetate suspension has a comparable antiinflammatory effect but is more likely to cause granuloma formation at the injection site. Duration of effect of either drug depends on the severity of the uveitis. Nonocular use of either drug has been linked to equine laminitis.
Intravitreal triamcinolone injection may provide a safe and effective method to control ERU. In one study evaluating the ocular distribution and toxicity of intravitreal triamcinolone, six horses were injected intravitreally with 10, 20, or 40 mg of triamcinolone. There was no evidence of overt toxicity from intravitreal triamcinolone injection in normal horses, and a single intravitreal injection resulted in ocular levels of triamcinolone for 21 days. However, the risk for bacterial infection after intravitreal injection or anterior chamber aspiration in horses appears to be high.143
Evaluation of inflamed eyes should always include topical application of fluorescein dye to rule out ulcerative keratitis. This precaution is especially critical when considering the use of subconjunctival corticosteroids that deliver prolonged and irreversible effects. Topical and subconjunctival corticosteroids are contraindicated in the presence of corneal ulcers because they delay healing, potentiate the destructive effects of endogenous and microbial enzymes, and predispose the cornea to secondary infection.
NONSTEROIDAL ANTIINFLAMMATORY DRUGS. Parenteral corticosteroids may be used when topical and subconjunctival agents are ineffective in controlling inflammation, but NSAIDs are usually preferred in such cases. Use of these antiprostaglandin agents counteracts an important mediator of intraocular inflammation, minimizing the role of parenteral steroids in uveitis therapy and the attendant risk of laminitis. Flunixin meglumine (Banamine) is the NSAID of choice for the eye, administered at a dose of 0.5 to 1.1 mg/kg PO or IV twice daily for 5 days, then 0.5 mg/kg PO once or twice daily. Oral phenylbutazone at 2.2 to 4.4 mg/kg once or twice daily can be used in cases of mild uveitis or in animals that require chronic low-dose oral prophylaxis for recurrent disease. Dosage requirements for aspirin make it less practical in acute cases, but prolonged oral administration of 15 mg/kg twice daily has been used to avert relapses. Frequency of NSAID administration should be reduced as clinical response occurs because antiprostaglandins have been linked to GI ulceration and renal dysfunction with high doses or chronic use.
Topical ophthalmic NSAIDs are generally more costly than corticosteroids and not as potent if used alone. However, an additive antiinflammatory effect can be seen when topical NSAIDs are used in conjunction with topical corticosteroids in horses with acute or resistant uveitis. Although generally considered a safe alternative to topical corticosteroids in the presence of corneal ulceration, topical NSAIDs have been implicated in the development of melting corneal ulcers in humans. Available generic solutions include 0.03% flurbiprofen sodium and ketorolac tromethamine 0.5%. Dosage frequency is empirical, with intervals ranging from every 6 to 12 hours.
MYDRIATIC/CYCLOPLEGIC AGENTS. A parasympatholytic mydriatic or cycloplegic agent must be used if equine uveitis is to be managed successfully. By dilating the pupil and decreasing iris-to-lens contact, the chance of posterior synechia formation—and secondary glaucoma—is reduced. An adequately dilated pupil may also promote vision during the acute episode. Ciliary spasm is relieved, making the horse more comfortable, and the iridociliary vessels return to a more normal state of permeability, with normalization of aqueous humor constituents.
Topical application of 1% atropine solution or ointment is indicated at a frequency no more than two to four times daily until the pupil dilates. The ultimate goal is to maintain mydriasis with the least frequent application possible, keeping in mind the resistance of the inflamed iris and ciliary body to the effects of atropine. Horses on an intensive parasympatholytic regimen should be strictly monitored for signs of reduced gut motility and colic because systemic effects can occur with frequent topical atropine administration.144 Pupillary dilation may persist for 4 weeks or more after cessation of therapy.
If mydriasis is slow or incomplete, 10% phenylephrine hydrochloride solution may be used topically in conjunction with atropine.145 Although a study in the horse suggests that phenylephrine is ineffective when combined with a parasympatholytic agent, investigators did not rule out a possible benefit if dosage or duration of therapy was increased.146 However, frequently applied phenylephrine has been associated with the development of corneal ulcers, corneal endothelial toxicity with secondary corneal edema, and increased uveal exudation, so response to the drug should be monitored carefully.
ANTIBIOTICS. Because current evidence suggests an immune rather than an infectious basis for recurrent uveitis, antibiotics have assumed a secondary role in ERU management. Although topical antibiotic preparations may discourage opportunistic bacteria during intensive corticosteroid therapy, few will cross the intact cornea and reach therapeutic levels in the anterior chamber or uveal tract. In horses with positive leptospiral titers in serum or ocular fluids, systemic antibacterial therapy with oral doxycycline (10 to 20 mg/kg twice daily for 4 weeks) may minimize recurrences of uveitis.147 In eyes with mechanical disruption of the blood-aqueous barrier, administration of enrofloxacin IV at 7.5 mg/kg q24h resulted in aqueous humor concentrations greater than the reported MIC for L. pomona, suggesting that enrofloxacin may be a good antibiotic choice for horses with leptospirosis-associated ERU.148
OTHER THERAPIES. A novel therapeutic approach to management of equine recurrent uveitis was recently described by Fischer and colleagues.149 Intravitreal injection of 4 mg gentamicin showed promising results in controlling chronic recurrent and persistent uveitis in 71 horses. Complications of the injections were minimal; however, progression of cataract was noted in 5.4% of the horses. Intravitreal gentamicin injections can be performed under standing sedation and may be recommended in horses with uveitis that are refractory to antiinflammatory medication, since a lesser therapeutic effect of a suprachoroidal cyclosporine implant may be seen in such patients.159
If leptospiral infection has been well documented in a group of horses with uveitis, vaccination against the disease may be considered. However, although in one study vaccination significantly increased the interval to recurrence (median of 126 days) compared with nonvaccinated controls (median of 86 days), the practice failed to slow the progression of disease in a group of 41 ERU-affected horses.150 Recently, Zoetis developed the Lepto EQ Innovator® vaccine for L. pomona to prevent leptospirosis infection and thereby reduce the risk of abortion, acute renal failure, and development of equine recurrent uveitis. It is not advisable to administer the vaccine to horses that have already developed uveitis, since the immune response to the vaccine could potentially exacerbate the uveitis.
An intracameral injection (25 μgZ0.1 mL) of tPA can be used to accelerate fibrinolysis and clear hypopyon in the anterior chamber of horses with severe uveitis. However, tPA should be avoided in eyes with evidence of hemorrhage in the previous 48 hours.
The precise role of Onchocerca species in the pathogenesis of ERU is not yet determined, and considerable controversy exists regarding the necessity or benefit of microfilaricidal therapy in cases of ocular onchocerciasis (see the Ocular Parasites section later).
Acupuncture and homeopathic remedies such as poultices of chamomile and oral methylsulfonylmethane (MSM) have been used in the treatment of ERU, but the efficacy of these unconventional modalities is unknown.
■ Prevention of Disease Recurrence
CYCLOSPORINE. Cyclosporine A (CsA) is a noncytotoxic immunosuppressive drug that blocks transcription of IL-2 and decreases T-cell responsiveness during the initiation of inflam- mation.151,152 These properties could block the nonspecific activation of T cells in recurrent episodes of ERU. With its poor inherent antiinflammatory properties, cyclosporine is likely to be more effective in preventing recurrences than treating active inflammation. Unfortunately, topical application of cyclosporine fails to achieve effective intraocular levels in horses and other species.153 However, reports of sustained intraocular levels of CsA in ocular tissues154,155 and resolution of clinical signs in experimental uveitis after implantation of a CsA-impregnated device into the vitreous of rabbit eyes156 set the stage for implantation of a similar device into the anterior vitreous of horses with experimental uveitis. The CsA-containing implant significantly decreased the duration and severity of inflammation, cellular infiltration, tissue destruction, protein concentrations, and the level of transcription of proinflammatory cytokines in the experimental group.141 The intravitreal device also prevented recurrences in 81% of horses with spontaneous ERU, but overall success was limited by complications from intraocular hemorrhage, cataract progression, and retinal detachment.157 Because of significant risk of postoperative complications in the face of concurrent inflammation, a horse with active uveitis is not a suitable candidate for cyclosporine implantation until the inflammation is adequately controlled by conventional means.52 Intravitreal delivery devices containing other immunosuppressive agents such as tacrolimus were also effective in suppressing inflammation after intravitreal implantation in rabbits with experimental uveitis.158
To minimize ocular morbidity related to implantation, ongoing studies of cyclosporine have focused on development and evaluation of a deep scleral delivery device.159 Superficial episcleral implantation failed to achieve substantial intraocular levels of CsA or control inflammatory episodes in ERU-affected horses. Therefore the effects of a bioerodible implant infused with CsA and inserted into the suprachoroidal space beneath a partial-thickness scleral flap 1 cm posterior to the dorsolateral limbus were studied. High concentrations of CsA were achieved in the equine ciliary body, choroid, retina, and optic nerve. In horses with severe ERU, only 15% of eyes were blind a mean of 14.2 months after implantation. In contrast, 90% of patients with severe ERU treated conventionally are blind within 1 year.52 In vitro studies of CsA also documented a direct inhibitory effect on Leptospira growth at concentrations achievable within the uveal tissues after deep scleral implantation.159
In one retrospective study evaluating the long-term efficacy, complications, and duration of effect of suprachoroidal CsA implants in horses with ERU, the long-term maintenance of vision of these horses was demonstrated. In 151 eyes of 133 horses from the United States and Europe that had CsA devices implanted with a mean and median follow-up time of 28.9 and 26.3 months (range of 13 to 85 months), respectively, 78.8% of eyes were considered visual at last follow-up.160 The overall mean frequency of uveitis episodes after CsA implantation was 0.09 ± SD 0.08 episodes per month. Among implanted horses, the most common complications leading to vision loss at last follow-up were persistent uveitis episodes (54%), glaucoma (22%), mature cataracts (16%), and retinal detachment (6%). Persistent uveitis episodes tended to be the highest cause of vision loss in implanted horses with less than 24 months and more than 48 months of follow-up.160
CORE VITRECTOMY. Pars plana vitrectomy has been used to remove fibrin, inflammatory cells, and debris trapped in the vitreous and to improve vision and delay progression of clinical signs in affected horses.12,161,162 Proponents theorize that removal of T cells or infectious organisms like Leptospira may reduce adverse interactions between the vitreous and the uveal tract, thereby reducing the recurrence of ERU. The technique appears more beneficial in European warmbloods with ERU than in Appaloosas with ERU in the United States. In one German study, recurrence of ERU was prevented in 85% (29 of 34) of treated eyes followed for 5 months to 5 years, but 45% of horses developed significant cataract formation.142 A study of vitrectomy performed in the United States was also complicated by postoperative cataract formation and progressive loss of vision, despite some decrease in recurrence of uveitis.163 More recent reports of vitrectomy performed on more than 1200 eyes at the University of Munich described no further recurrences of ERU in 98% of patients.164 Cataract formation and retinal detachment were reportedly rare in this group of animals. Investigators explained their success on the basis of improved patient selection and surgical expertise.
■ Prognosis The long-term prognosis for vision in horses with recurrent uveitis is poor, although statistics of actual rates of vision loss are limited. Dwyer's 11-year study of ERU-affected horses reported that 56% of the 160 study animals experienced blindness in one or both eyes.52 Appaloosas and Leptospira- seropositive horses were at increased risk for blindness over the course of the study. All seropositive Appaloosas (100%) lost vision in at least one eye; 50% were completely blind. Among seronegative Appaloosas, 72% lost vision in one or both eyes, and 29% were totally blind. Seropositive horses of other breeds lost vision in one or both eyes 51% of the time, with total blindness in only 17%. Seronegative non-Appaloosas had the best prognosis, with 34% losing vision in one or both eyes and total blindness in only 6%.
Bovine-Specific Ophthalmia
A recurrent uveitis of cattle has been described and compared to that of the horse.165,166 As with ERU, its definitive etiology is unknown, although a viral infection was originally suggested. Clinical signs include conjunctival hyperemia, corneal edema and vascularization, inflammatory cells and hemorrhage within the anterior chamber and uveal tract, and retinal and choroidal edema and hemorrhage. The disorder is uncommon and does not share the notoriety of its equine counterpart. Therapy is directed at reducing inflammation, as described for the horse.