Infarctive Purpura Hemorrhagica
Stephanie J. Valberg
Infarctive purpura hemorrhagica (IPH) is a severe form of purpura with a high fatality rate. In one study, prevalence of IPH was 3 of 53 cases of purpura.97 Exposure to S.
equi within 3 weeks of presentation, vaccination for S. equi, and a concurrent Salmonella infantum infection are reported as inciting causes. Titers for serum enzyme-linked immunosorbent assay (ELISA) M protein may be markedly elevated.98 The primary presenting complaint is often painful lameness with limb swelling, muscle stiffness, and/or colic. Careful physical examination reveals classic signs of purpura hemorrhagica such as petechia, oral infarctions resembling ulcers, and moderate well-demarcated limb edema; however, in addition, horses with IPH will have focal firm intramuscular swellings (Fig. 42.9). Horses with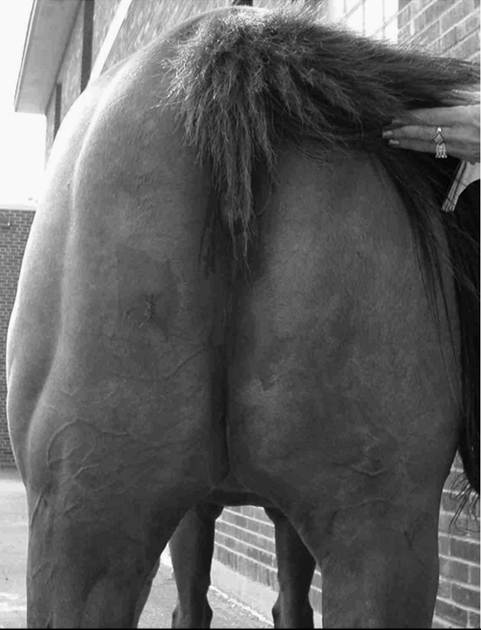
FIG. 42.9 Marked swelling of the right adductor muscles of the thigh due to infarctive purpura hemorrhagica.
evidence of colic may have markedly decreased borborygmi and hemorrhagic gastric reflux.
Hematologic abnormalities include a leukocytosis characterized by a neutrophilia with a left shift and toxic change, hyperproteinemia, hypoalbuminemia, and marked elevations in CK (47,000 to 280,000 U/L) and AST (960 to 7000 U/L) activities.93,98 Peritoneal fluid obtained by abdominocentesis may be normal or may have an increased total protein, nucleated, and RBC counts if gastrointestinal infarction is present. Ultrasonographic examination of swollen muscle reveals focal hypoechoic lesions within muscle tissue. Biopsies of abnormal muscle show diffuse acute coagulative necrosis, whereas samples from palpably normal muscle tissue show no pathologic abnormalities.
Postmortem findings of horses with IPH include infarction of the skeletal musculature (Fig.
42.10), skin, gastrointestinal tract, pancreas, and lungs, as well as S. equi abscessation of a lymph node. Definitive histopathologic findings include leukocytoclastic vasculitis and acute coagulative necrosis resembling infarction in numerous tissues.98 IPH resembles Henoch- Schonlein purpura in humans, which is characterized by infarctive vasculitis of the skin, kidneys, and gastrointestinal tract due to immunoglobulin A (IgA) immune complex deposition. Immune complexes are present in the sera of horses with purpura hemorrhagica that appear to be primarily composed of IgM or IgA and streptococcal M protein.99 Deposition of complement near immune complexes in vessel walls may result in cell membrane destruction, cell death, and vascular occlusion. The distinctive feature of IPH in horses is the extensive infarction of skeletal muscle and consequently marked elevation in serum CK and AST activity.Early recognition of signs and aggressive antibiotic and corticosteroid treatment are essential to combat the high fatality rate with IHP. Treatment of Henoch-Schonlein purpura in humans, including cases with intestinal infarctions, involves high-dose intravenous pulse therapy with methylprednisolone followed by oral corticosteroids plus immunosuppressive agents such as cyclophosphamide and azathioprine. One horse with IPH was successfully treated with penicillin, NSAIDs, and 3 weeks of dexamethasone (0.01 to 0.07 mg/kg IM or IV) followed
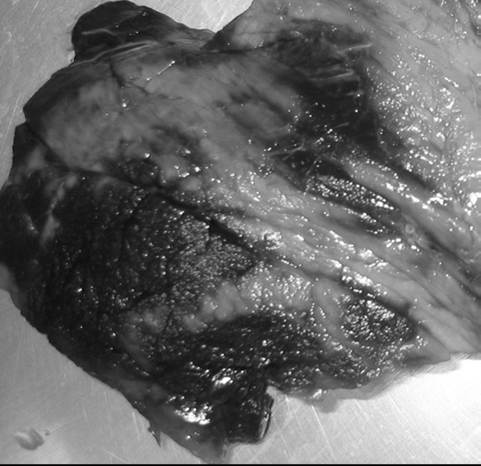
FIG. 42.10 Numerous infarctions of skeletal muscle due to infarctive purpura hemorrhagica. (Courtesy Dr. Beth Davis.)
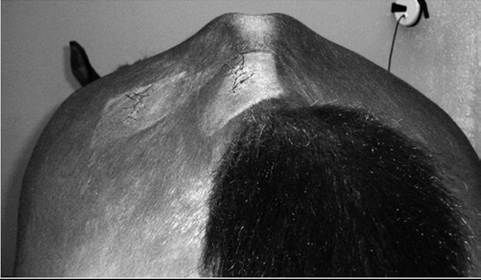
FIG. 42.11 Symmetric atrophy of the gluteal muscles with immune- mediated myositis. (Courtesy Dr. Beth Davis.)
by a 10-week tapering course of oral prednisolone (2 mg/kg initially).95