Infertility Caused by Abnormalities of the Female Tubular Genitalia
Salpingitis
Inflammation of the oviducts is characterized by macroscopic enlargement. Lesions are frequently bilateral and consist of infiltration by lymphocytes, plasma cells, and neutrophils, and desquamation of epithelial cells.
Most cases of salpingitis follow infections of the uterus. Necrotizing and granulomatous salpingitis may follow infection by Trueperella pyogenes (formerly Arcanobacterium pyogenes), Mycobacterium tuberculosis, and Brucella abortus. Mild inflammation of the uterine tubes that does not usually result in permanent damage accompanies uterine infection caused by Campylobacter fetus subsp. venerealis and Tritrichomonas foetus. Salpingitis may be a sequela to manipulations of the ovaries and uterine tubes by palpation per rectum, transvaginal ovum pickup, aggressive irrigation of an infected uterus, and inappropriate treatment with estrogenic hormones. Migrating larvae of Strongylus edentatus have been proposed as a possible cause of nonobstructive infundibulitis in mares, but their role is speculative.
Pyosalpinx is characterized by segmental accumulation of pus within the lumen of the oviduct after mechanical blockage of either end. Pyosalpinx frequently follows severe cases of uterine infection and may be complicated by perimetritis and localized peritonitis.
Hydrosalpinx is characterized by accumulation of thin mucus within the lumen of the oviduct. Hydrosalpinx and adhesions to perisalpingial tissues are common sequelae to chronic salpingitis.
■ Clinical Signs and Diagnosis The usual history associated with diseases of the uterine tubes is one of infertility. Additional history may include uterine infection or traumatic therapy such as uterine irrigation, enucleation of CLs, or administration of exogenous estrogen during CL function. Salpingitis is an uncommon clinical finding in the mare.
However, in one study up to 88% of mares were found to have macroscopic lesions in the oviduct, including adhesions, fibrous bands, and parovarian cysts, which may or may not have affected fertility.1 Accumulations of cells and debris may form intraluminal masses; however, their role in infertility has not been adequately tested.2 Similarly, moderate lesions of uterine tube disease may escape diagnosis by physical examination in cows, but the results of abattoir studies suggest that lesions of the oviducts are not uncommon. In cows, lesions involving adhesions among the ovary, ovarian bursa, oviduct, and surrounding tissues may be identified per rectum by inserting two or three fingers into the ovarian bursa and rolling the oviduct between the fingers and thumb. Easy identification of the oviduct by palpation per rectum is sometimes considered indicative of abnormalities. Diagnosis of diseases of the oviducts in ewes and does is impossible by physical examination. Although a history of infertility after one of the predisposing causes might suggest oviductal lesions, diagnosis is made by exploratory laparotomy, peritoneoscopy, or necropsy.Lesions of the oviductal or perisalpingial tissues must be differentiated from other causes of abnormal enlargements such as ovarian neoplasia, parovarian cysts, cystic ovarian disease, and ovarian hematomas. Neoplasia of the oviducts in domestic animals is extremely rare.
■ Clinical Pathology Several tests that determine oviductal patency of mares3,4 and cows5 have been described, but neither the starch test nor the phenolsulfonphthalein dye test is reliable or consistently diagnostic. For suspected unilateral blockage, each uterine horn may be catheterized individually with a Foley catheter placed at the base of the horn on different days.6
■ Embryo Recovery Embryo recovery after either a single ovulation or superovulation is objective evidence that one or both uterine tubes are patent and functional.
Improved reproductive performance of cows may follow uterine lavage; therefore embryo recovery as a diagnostic test may have therapeutic benefits as well.7■ Treatment and Prognosis Treatment of diseases of the oviducts is not likely to be successful. Appropriate treatment for concurrent uterine infections should be instituted. A period of sexual rest may be beneficial and is indicated in valuable animals. The prognosis for reproduction in cases of bilateral obstruction of the oviducts is poor. In vitro fertilization of ova harvested from affected females is a therapeutic option. Affected females can also serve as embryo recipients.
■ Prevention and Control Traumatic manipulation of the ovaries, irrigation of the endometrial cavity with large volumes of fluid (>100 mL in heifers or 150 mL in cows) or irritating chemicals, and administration of estrogenic hormones to luteal phase females should be avoided. Because abnormalities of the oviducts are frequently associated with uterine infections, reduction of the prevalence of uterine infections results in fewer tubal infections as well.
Uterine Abnormalities
Retained Fetal Membranes
MARES. Retention of the fetal membranes beyond a period of 3 hours is an abnormal occurrence in the mare. The mare has an epitheliochorial placenta characterized by diffuse microvilli that interdigitate with endometrial crypts. After delivery, blood flow through the placental vessels is reduced. Placental microvilli shrink and disengage from endometrial crypts. The pathophysiology of the disease is poorly understood but may involve disturbances of normal prepartum endocrine events or myometrial contractility. The condition is more common after abortion, dystocia, cesarean section, and fetotomy. Partial placental retention may be localized to well-defined areas of continued placental attachment. The most common site of partial retention is the previously nongravid horn.
Equine placentas should be spread on a flat surface after expulsion and examined to ensure that the complete membrane is present.
Areas of placental necrosis are common near the tips of the uterine horns, and the fragile area may be incarcerated by the rapidly contracting uterus.■ Clinical Signs and Diagnosis Retained fetal membranes (RFMs) are usually visible at the vulva. However, small tags of placental tissue may remain attached to the uterus without being apparent and may be a nidus for infection, resulting in severe metritis, endotoxemia, and laminitis hours to days postpartum.
■ Treatment and Prognosis The severity of sequelae makes early intervention essential. Treatment should begin if fetal membranes are not passed within 3 hours of foaling. Most instances respond to vigorous early pharmacologic treatment. Occasional cases require several days of persistent treatment.
MANUAL REMOVAL. Manual removal should be avoided because trauma induces placental tearing, leaving microvilli in endometrial crypts.
OXYTOCIN. Oxytocin induces myometrial contractions, which may aid placental expulsion. Oxytocin may be administered by IV injection (5 to 20 IU every 30 to 60 minutes) or IM injection (10 to 20 IU every 30 to 60 minutes), or it may be infused slowly (30 to 80 IU in 500 mL of warm saline IV over 30 to 60 minutes). Care should be taken to avoid higher doses, which may result in signs of abdominal pain and will cause tetanic rather than orchestrated uterine contraction.
ALLANTOCHORIONIC INFUSION. If the allantochorion is intact, the allantochorionic cavity may be filled to distention with 3 to 4 gallons of warm saline or water through the cervical star.1 The opening in the placenta is held closed manually until the mare exerts abdominal pressure. Oxytocin may be used in conjunction with this treatment.
UTERINE LAVAGE. If the allantochorion is not intact, uterine lavage with an isotonic saline solution will clear debris, will trigger myometrial contractions, and may help free the retained fragment of the fetal membrane. The isotonic saline solution may be infused into the uterus through an equine nasogastric tube (dedicated to reproductive use) manually held in place.
Approximately 5 L may be placed in the uterus of a full-grown, postpartum mare at one time, but care should be taken to observe the mare for signs of discomfort and to gauge the amount of fluid felt within the uterus. During fluid infusion the operator may carefully explore the uterus manually, searching for RFM remnants. Once the uterus is relatively full of fluid, the fluid is siphoned out. Care must be taken to protect the fragile endometrium from damage incurred by the strong suction force of the siphon. The operator’s hand should guard the end of the tube from direct contact with the endometrium. This process should be repeated until the effluent is clear. Uterine lavage should be performed at least once daily until 12 to 24 hours after the RFM remnants are retrieved.ADJUNCT THERAPY. Concurrent therapy directed at controlling or minimizing common sequelae to retained placenta is often indicated.
1. Antimicrobials. Bacterial infections are commonly associated with prolonged (>6 to 8 hours) retention of the fetal membranes. The bacterial population is frequently mixed and likely to include β-hemolytic streptococci and coliforms. In prolonged cases, bacterial culture and sensitivity should be performed. Broad-spectrum antibiotics known to be effective against commonly isolated organisms are indicated. Drugs that have been recommended for systemic administration include amikacin, ampicillin, gentamicin, kanamycin, penicillin, ticarcillin (with gentamicin for Pseudomonas infection), and trimethoprim-sulfamethoxazole. Intrauterine administration of antibiotics and antiseptics depresses phagocytic activity of uterine neutrophils, and many chemicals irritate the endometrium. Drugs that have been suggested include those recommended for systemic administration.
2. Antiinflammatory drugs. Laminitis may be a sequela to metritis and is commonly associated with RFMs. Treatment with administration of antiinflammatory drugs such as phenylbutazone or flunixin meglumine is indicated to reduce the likelihood and severity of laminitis.
Polymyxin B may also be indicated in cases in which preliminary signs of laminitis are noted because of its antiinflammatory and antiendotoxic effects. Additional therapy for laminitis should be administered as indicated.3. Other treatments. Caslick's surgery may be indicated in some cases of RFMs to control aspiration of air. Tetanus may complicate RFMs, and prophylaxis with tetanus antitoxin in unvaccinated animals or tetanus toxoid in previously vaccinated animals is indicated.
Some cases of RFMs are refractory to treatment, and membranes may remain firmly attached to the endometrium for several days. Aggressive attempts at manual removal should be eschewed because severe endometrial damage may follow. Persistent treatment with uterine lavage antibiotics, antiinflammatory drugs, and oxytocin is indicated until the placenta is expelled and bacterial infection of the uterus is controlled.
The prognosis for RFMs is generally good but is reduced if treatment is delayed or if retention is accompanied by infection with virulent pathogens. Sequelae to RFMs include metritis, endometrial fibrosis, invagination of a uterine horn, uterine prolapse, and laminitis.
Ruminants
■ Clinical Signs and Diagnosis The majority of affected cows show no serious clinical signs other than a transient decrease in appetite and milk production. However, 20% to 25% of cows affected by RFMs develop moderate to severe metritis. The most overt clinical signs are malodorous discharge and placental tissue hanging from the genital tract. RFMs are usually expelled by 4 to 10 days after calving when the caruncular tissue has become necrotic and is sloughed. Some affected cows show signs of endotoxemia, including depression, fever, ruminal stasis, and inappetence, as a result of RFMs.
■ Treatment and Prognosis A variety of treatments have been suggested for RFMs in cows, including aggressive attempts at manual removal, myometrial stimulants, intrauterine and systemic antibiotics (alone or in combination with other approaches), and no therapy whatsoever. Because the processes that culminate in RFMs begin during late gestation, it is expected that treatment initiated at calving has little effect on the loosening process. Most treatments for RFMs are directed toward controlling the intrauterine bacterial population.
MANUAL REMOVAL. Manual removal of the placenta is indicated only when gentle traction is sufficient to withdraw the membranes in a short time. Attempts at manual removal are contraindicated if the patient shows clinical signs of septicemia. Trauma caused by manual removal inhibits phagocytosis by uterine neutrophils and predisposes to severe sequelae, including endometritis, septic metritis, peritonitis, and a delay to first ovulation.
MYOMETRIAL STIMULANTS. Administration of a single dose of oxytocin does not reduce the prevalence of RFMs in cows that calve spontaneously or in cows that require assistance at delivery.4,5 Cows with RFMs have an elevated plasma concentration of estrogen during the period of retention; therefore administration of additional estrogen for treatment of RFMs may be of questionable value. Intravenous calcium solutions are indicated in cases of RFMs secondary to hypocalcemia. Because a relatively small proportion of RFMs are due to myometrial atony, myometrial stimulants may not be beneficial in many cases.3
PROSTAGLANDIN. In one trial, treatment with fenprostalene (a prostaglandin) resulted in a shorter period of retention in treated cows, reduced the number of treatments subsequently required for metritis, and slightly reduced the intervals to first service and conception. However, other researchers found that fenprostalene produced no changes in myometrial activity between days 1 and 4 after calving and concluded that uterotonic agents are unlikely to hasten placental expulsion, because uterine effort is already increased in animals that have RFMs. An imbalance between synthesis of PGF2α and Prostaglandin I2 (PGI2) between 30 and 60 minutes after parturition has been demonstrated in cows affected by RFMs. Prostaglandin at the time of calving does not reduce the incidence of RFMs or improve reproductive performance.
ANTIBIOTICS. Intrauterine tetracycline may reduce fertility, or the reproductive performance of treated cows may be as good as that of untreated herdmates. Intrauterine treatment with 4 to 6 g of oxytetracycline per day until the placenta is expelled may reduce the prevalence of metritis associated with RFMs, but pyometra may develop in treated cows. The placenta is released only after necrosis of the caruncles, which may be delayed by the presence of intrauterine antibiotics. Systemic antibiotics are indicated in cases of RFMs in which the cow has a fever, is off feed, or has a drop in milk production. Multiple studies have demonstrated that the effects of systemic antibiotics are just as good as intrauterine antibiotics alone or a combination of systemic and intrauterine antibiotics in terms of systemic health and future fertility. Ceftiofur (2.2 mg/kg IM or subcutaneously [SC] q24h for 3 to 5 days) given to febrile cows with retained membranes has shown a beneficial effect in future reproductive parameters and may reduce the incidence of acute metritis.3,13,14
Cows that retain their membranes for more than 12 hours after calving are more likely to develop metritis than are cows that promptly expel the membranes. However, reproductive performance of cows that rapidly return to normal after RFMs is similar to that of their unaffected herdmates, indicating that in the absence of a secondary reproductive abnormality, RFMs have a minimum effect on future fertility.
COLLAGENASE. An alternative approach to the treatment of RFMs is the injection of collagenase into the umbilical arteries of the retained membranes.15 This treatment is aimed directly at the lack of cotyledonary proteolysis, and although effective, it is expensive and often not economically justifiable. Intrauterine infusion of collagenase is not effective.
Ewe and Doe
Fetal membranes are considered retained in ewes and does if not expelled within 12 hours after delivery of the last fetus. The prevalence in does is approximately 6% after spontaneous delivery but may be higher when delivery is complicated by dystocia or abortion. Selenium deficiency has been suggested as a cause.
The clinical signs of RFMs in ewes and does are usually obvious. Does may ingest their placentas, complicating identification of cases of partial retention. RFMs may accompany retention of a fetus within the uterus, and does and ewes should be carefully examined.
Other tissues that may be exposed from the vulva in association with parturition are a prolapsed uterus, a prolapsed or everted urinary bladder, prolapse of some portion of the digestive tract through a uterine rupture, prolapsed rectum, prolapsed vagina, or a twin fetus.
■ Treatment and Prognosis Manual separation of cotyledons from caruncles is impossible in ewes and does; therefore manipulative attempts to remove the placenta are limited to gentle traction on exposed membranes at daily intervals. Treatments with broad-spectrum systemic antibiotics, oxytocin (10 to 20 IU) at 12-hour intervals until the placenta is expelled, and antiinflammatory drugs have been suggested. Prophylaxis against tetanus is indicated.
Camelids
The placenta is usually passed within 1 to 2 hours of parturition. Camelid placentas resemble equine placentas (diffuse, micro- cotyledonary, epitheliochorial), with the exception that the left horn is almost always the pregnant horn. RFMs in camelids are most commonly seen as sequelae to dystocia or other disorders of parturition. Treatment is similar to that described for the mare.
Uterine Infections
■ Mare
Endometritis
A failure of the uterine defense mechanisms to effectively eliminate an antigen (bacteria or spermatozoa) and inflammatory products from the uterus results in persistent endometritis, which is a major cause of reduced fertility in broodmares.16 In the normal mare the uterus is well protected from external contamination by physical barriers consisting of the vulva, vestibule, vagina, and cervix, and any compromise of these barriers may predispose the mare to a chronic uterine infec- tion.17 Breeding is another source of uterine contamination. Intrauterine deposition of semen causes an inflammatory reaction resulting from bacterial contamination of the ejaculate or from spermatozoa.18 Approximately 10% to 15% of a normal population of Thoroughbred broodmares developed persistent endometritis after breeding.19 AI with frozen semen resulted in 16% to 25% persistent inflammation after breeding.20,21 Natural resistance to experimentally induced bacterial contamination has been demonstrated in young mares, whereas a population of multiparous and barren mares developed persistent endometritis after bacterial contamination of the uterus.22,23 On the basis of these studies, mares have been classified as either susceptible or resistant to persistent uterine infection.22 Endometritis has severe effects on the fertility of affected mares. A persistent inflammation may interfere directly with the survival of an embryo or may cause premature luteolysis and embryonic loss because of increased PGF2α concentrations.24
Several classes of immunoglobulins have been isolated from the equine uterus. Although antibody-mediated uterine defense may be important for effective elimination of bacterial contaminants from the uterus in susceptible mares, concentrations of immunoglobulins in uterine secretion are similar or even elevated compared with those of resistant mares.25-29 Polymorphonuclear neutrophils (PMNs) are the first inflammatory cells to enter an inflamed site. Chemoattractive properties of uterine fluid have been described in vitro in horses, and the uterus responds quickly to an antigen with release of PMN-chemotactic mediators, which results in a rapid migration of PMNs into the uterine lumen.30 Complement products and leukotriene B4 (LTB4), Prostaglandin E (PGE), and PGF2α may all serve as chemoattractants for PMNs in the uterus.30-34 Studies on the role of local uterine factors in PMN function suggested that an impaired phagocytosis by uterine PMNs in susceptible mares is the result of insufficient opsonization in uterine secretion rather than a primary dysfunction of the PMNs.35
Recent work by researchers at the University of Kentucky found that breeding, as well as a bacterial infection with Escherichia coli, resulted in an upregulation of both proinflam- matory and inflammatory modulating cytokines in the endometrium. A transient upregulation of proinflammatory cytokines was observed in resistant mares, whereas a sustained expression of proinflammatory cytokines coupled with an altered ratio of proinflammatory and modulating cytokines was observed in susceptible mares.36 An imbalanced cytokine expression was also observed in susceptible mares following breeding. Inflammatory modulating cytokines were expressed at a significantly lower level at 6 hours after breeding in susceptible mares when compared with resistant mares, leading the authors to conclude that susceptible mares may have a deficiency in their ability to regulate endometrial inflammation.37
Mechanical aspects of the uterine defense system are currently believed to be a major contributor in uterine clearance of bacteria and inflammatory products.38-40 Through use of intrauterine inoculations of a combination of radioactive-labeled microspheres and bacteria, impaired uterine clearance was demonstrated in susceptible mares but not in resistant mares.38 Studies using scintigraphic measurements of intrauterine clearance of radioactive colloids further defined a delayed physical clearance in susceptible mares.39 Through use of electromyography (EMG) to register myometrial activity, it was observed that the impaired uterine clearance in susceptible mares was caused by reduced myometrial activity in response to the inflammation.39 This may be explained by an accumulation of nitric oxide (NO) in susceptible mares following breeding.41 NO is an inflammatory mediator that causes smooth muscle relaxation. The dependent position of the mare's uterus may also interfere with effective clearance.
Based on pathogenesis, persistent endometritis can be divided into (1) sexually transmitted diseases (STDs), (2) persistent uterine infection, and (3) persistent breeding-induced endometritis.
SEXUALLY TRANSMITTED DISEASES. Contag ious equine metritis (CEM) is an example of a true STD.42’43 The disease is caused by Taylorella equigenitalis, a highly contagious and pathogenic microorganism. Although the present status of a mare's uterine defense mechanism is important for the manifestation of the disease, this bacterium is highly resistant and capable of overcoming the mare's normal disease barriers.
PERSISTENT UTERINE INFECTION. Bacteria most commonly isolated from the uterus of the mare are β-hemolytic streptococci (Streptococcus Zooepidemicus and Streptococcus equisimilis), E. coli, Pseudomonas aeruginosa, and Klebsiella pneumoniae. Other aerobic bacteria isolated from the reproductive tracts of mares include α-hemolytic streptococci, Corynebacterium spp., Staphylococcus spp., Enterobacter spp., Actinobacter spp., Proteus spp., Citrobacter spp., Candida spp., and Aspergillus spp. and are the organisms most commonly associated with yeast or fungal endometritis. The role of viruses, mycoplasmas, ureaplasma, and anaerobic bacteria in endometritis is poorly understood. P aeruginosa, K. pneumoniae, and possibly S. Zooepidemicus and E. coli can be sexually transmitted in horses, but the consequences of exposure to these microorganisms are determined by the particular strain involved and active participation of all facets of the mare's uterine defense mechanisms. In contrast to a true STD, persistent infectious endometritis is often the result of contamination of the uterus by the mare's fecal and genital flora in combination with compromised uterine defense.44,45 It has been proposed that endometrial biofilms are responsible for chronic infectious endometritis that appears to be nonresponsive to conventional treatment.46 A bacterial biofilm is a complex aggregation of microorganisms. They are characterized by structural heterogenicity, genetic diversity, complex community interactions, and an extracellular matrix of polymeric substances, which greatly increases resistance to antibiotic therapy.47 Although uterine biofilms have not yet been identified in the clinical setting in horses, an experimental model to study biofilms in the equine endometrium has recently been developed. Workers inoculated mares with a uterine infusion of P aeruginosa and later successfully identified biofilms within the mares endometrial folds.48 An alternative explanation for persistent bacterial endometritis has been offered by Petersen and colleagues.49 The authors suggested that bacteria can persist in the endometrial glands and the uterine wall in a dormant state. This would increase their resistance to antibiotic therapy. Another study investigated potential mechanisms of persistent uterine infections with S. Zooepidemicus and hypothesized that the bacteria can enter epithelial cells and evade diagnosis and attempts to treat and resolve the infection.49 More work needs to be done to further understand the ways in which bacteria infect and survive in the equine endometrium.
PERSISTENT BREEDING-INDUCED ENDOMETRITIS. Intrauterine deposition of semen causes an inflammatory reaction resulting from spermatozoa.50,51 The mechanism of the induced inflammation is similar to endometritis caused by bacteria, involving activation of the complement cascade.51 The role of spermatozoa in breeding-induced endometritis implies that a transient uterine inflammation is a physiologic reaction to semen, and it appears to be a normal process by which excess sperm and bacterial contamination are eliminated from the 4552
mares reproductive tract.45’52 Transport of spermatozoa from the uterus to the oviduct is completed within 4 hours after breeding, and only a small portion of the ejaculated or inseminated semen reaches the oviduct.53,54 The rapid transport of spermatozoa to the oviduct coincides with increased uterine activity.52 Increased myometrial contraction in response to breeding is also responsible for rapid sperm elimination from the uterus through the cervix.55 Not all excess spermatozoa are removed from the uterus through this mechanism. The remaining spermatozoa have to be eliminated by means of other uterine clearance mechanisms, such as PMN-phagocytosis of spermatozoa.45 However, the condition may develop into a persistent inflammation in mares with impaired uterine clearance.38,39 If sperm elimination and all physical and chemical reactions that are involved in the induced inflammation persist beyond the time when the embryo enters the uterus at 5 days after ovulation, embryonic loss will occur because of an incompatible inflammatory uterine environment. The incidence of persistent breeding-induced endometritis has been reported to be approximately 10% to 15% in a normal population of Thoroughbred broodmares and up to 25% in mares bred by AI with thawed frozen semen.19,20
In contrast to spermatozoa, seminal plasma has a suppressive effect on complement activation, PMN-chemotaxis, and phagocytosis.56 A function of seminal plasma may be to act as an inflammatory inhibitor or modulator in the uterus, which may be of importance with regard to the transient nature of breeding-induced endometritis. The duration of breeding- induced uterine inflammation was shown in a study to be shorter when seminal plasma was included in an insemination dose, compared with when all seminal plasma was removed and replaced by a commercial semen extender.57 Although the peak numbers of PMNs were the same for both groups, significantly fewer PMNs were recovered from the uterus at 24 hours compared with 6 and 12 hours after insemination when seminal plasma was included. In contrast, there was no significant difference in the number of uterine PMNs at 6, 12, and 24 hours of insemination in the absence of seminal plasma. Another function of seminal plasma in breeding-induced endometritis may be to protect spermatozoa from being phagocytosed and destroyed in an inflammatory environment. PMNs are present in the uterine lumen by 0.5 hours after breeding, but sperm transport is not completed until 3 to 4 hours later.53 In addition, when mares are inseminated twice within a 24-hour period, semen from the second insemination is introduced into an inflammatory environment. This environment is detrimental to sperm motion characteristics, and motile sperm cells appear to bind to PMNs, forming large clusters of PMNs and spermatozoa. Addition of seminal plasma has been shown to reduce the binding between spermatozoa and inflammatory cells in vitro.58 Recent data suggest that a specific protein in equine seminal plasma, CRISP-3, selectively protects viable but not dead spermatozoa from PMN-binding and phagocytosis.59,60 Selective protection of viable spermatozoa from PMN-binding and phagocytosis increases their survival in a hostile uterine environment and ensures that a sufficient number of spermatozoa reach the oviduct for fertilization while effective sperm elimination of nonviable spermatozoa can be maintained.
■ Diagnostic Approach History compatible with endometritis includes infertility after breeding to a fertile stallion. Mares with severe endometritis may have shortened interestrous intervals and may show vaginal discharge. Physical and speculum examination may show anatomic defects of the vulva or cervix. Excessively easy passage of a vaginal speculum may indicate loss of integrity of the vestibulovaginal sphincter. Discharge from the cervix and vaginal inflammation may be apparent. Transrectal palpation and ultrasonography may reveal accumulations of luminal fluid (Fig. 43.5). Diagnostically, it may be difficult to identify susceptibility to breeding-induced endometritis before breeding. Some mares have free fluid present in the uterine lumen before breeding, but most mares are not diagnosed until after they have been bred. If susceptibility to persistent breeding-induced endometritis is suspected, the mare should be monitored closely by ultrasonography per rectum at 6 to 12 hours after breeding, if possible, and at a minimum within 24 hours after breeding. If free fluid is present in the uterine lumen, the mare should be considered to have persistent

FIG. 43.5 Transrectal ultrasonographic image of uterine intraluminal fluid accumulation in a mare with endometritis.
mating-induced endometritis. Clearance of charcoal particles from the uterus within 48 hours of inoculation and the use of scintigraphy to measure uterine clearance have been suggested to be useful in identifying mares that are susceptible to persistent breeding-induced endometritis.39,61 However, these methods may not be practical under field conditions. Recent attempts to identify genetic markers for susceptibility to persistent endometritis are encouraging and may aid clinicians in identifying susceptible mares in the future.62
MICROBIOLOGY. Quantitative aerobic bacterial culture of the uterine lumen is necessary to identify potential pathogens and for antibiotic sensitivity testing. Samples can be obtained using a swab, low-volume uterine lavage, or an endometrial biopsy, and they should be taken during estrus. If a uterine swab is used, the swab should be transported in a nonnutritive medium to the laboratory. Inadvertent contamination of cultures with bacteria from the lower reproductive tract is common, so the culture instrument should be guarded until it is within the uterus.63 A false-positive bacterial sample result may be obtained as the result of contamination (even when doubleguarded swabs are used), and culture results should always be interpreted together with results from endometrial cytology. Samples obtained through a vaginal speculum may decrease the risk of contamination. The use of low-volume lavage (50 to 100 mL) has been suggested to be a sensitive method to obtain an endometrial sample for culture.64,65 It is important to use a closed system to infuse and recover fluid from the uterus in order to avoid environmental contamination when this method is used. False-negative results are frequently obtained even under optimal circumstances, and laboratory results should always be interpreted with consideration given to clinical findings. Use of culture and histologic interpretation of an endometrial biopsy appears to be the most accurate method to diagnose persistent infectious endometritis.66 Cultures may also be performed on endometrial biopsy samples. Culture samples for T. equigenitalis should be taken from the endometrium, cervix, clitoral fossa, and sinuses. Samples should be placed in Amies medium with charcoal or Stewart medium and be kept refrigerated until delivered to the laboratory.
ENDOMETRIAL CYTOLOGY. PMNs migrate into the uterine lumen in response to inflammation, so endometritis is rapidly and accurately diagnosed by examination of exfoliated endometrial cells. A sample may be taken with a guarded swab, with a cytology brush, or by low-volume lavage. Air-dried
■ TABLE 43.5
Endometrial Biopsy Grade and Fertility Prognosis (Kenney and Doig)
| Biopsy Category | Degree of Change | Predicted Foaling Rate (%) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| I | None | 80-90 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIA | Mild | 50-80 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| IIB | Moderate | 10-50 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| III | Severe | of the clitoral fossa and sinuses. Best results can be expected when treatment is initiated when the mare is in estrus and is combined with uterine lavage if inflammatory debris or intraluminal fluid is present. Cleansing of the vulva and the clitoris daily for 5 days with a 4% chlorhexidine or nitrofurazone ointment has been recommended.72 Sinusectomy can also be performed.73 Import regulations in countries free from CEM serve to prevent outbreaks of the disease. The spread of CEM on farms in endemic countries is best prevented by implementation of strict hygiene, screening of breeding stallions before the breeding season, and the use of AI, if allowed by the breed registry. PERSISTENT UTERINE INFECTION. Treatment of mares with persistent uterine infections needs to be directed toward the underlying breakdown of the uterine defense and against the microbial agent. The first therapeutic concern should be to remove predisposing causes, such as a breakdown of external genital barriers. Persistent uterine infection frequently follows degenerative or traumatic anatomic changes and loss of integrity of the barriers of ascending infection. Therefore Caslick's surgery, repair of cervical damage and perineal lacerations, and correction of urovagina should precede specific endometrial treatment. All potential sources of contamination, including intrauterine passage of diagnostic and treatment implements, should be minimized. In some mares, recovery follows with sexual rest and no further treatment. Mares that are susceptible to persistent uterine infections should be bred using minimal contamination techniques to avoid bacterial contamination of the uterus.74 Antibiotics may be administered by either local or systemic routes. Intraluminal fluid and inflammatory debris should be removed by uterine lavage before local treatment. Drugs and doses are summarized in Table 43.6. Treatment should be based on sensitivity. Mares should be treated during estrus when natural defense is maximal, and strict aseptic technique should be used. The volume of fluid used for antibiotic therapy depends on the size of the uterus. A total volume of 30 to 60 mL is usually sufficient. Treatment should continue daily for 4 to 6 days during the duration of estrus. Repeated contamination may indicate an unsuccessfully resolved predisposing cause. The clitoral fossa should always be considered as a primary location of bacteria grown in these cases. If culture results from the endometrium and clitoral fossa match, the clitoral fossa should be cleaned and treated locally with antibiotics. Removal of the primary microorganism may result in overgrowth of a second bacteria or fungus (superinfection). Critical studies of the efficacy of systemic antibiotics are limited, although effective concentration of amikacin has been measured in the endometrium after systemic administration.75 Parenteral administration may be easier, and the opportunity to introduce uterine contamination or cause uterine irritation with treatment is eliminated. Treatment of fungal infections is generally more challenging than treatment of bacterial infections. Culture and sensitivity will determine the choice of antifungal drugs (see Table 43.6). Fungal endometritis may require daily intrauterine infusions for 7 to 10 days to effectively resolve the infection. To avoid intrauterine infusions in the presence of high circulating concentrations of progesterone, treatment can be initiated 1 or 2 days after an injection of PGF2α in diestrual mares and continued until 1 or 2 days after ovulation. A single dose of a benzoylphenyl urea (lufenu- ron) has been suggested to effectively treat mares with fungal endometritis.76 Antimicrobial Alternatives and Supplemental Treatments. Although suitable antibiotics are the most effective treatment against infectious endometritis, recent research has focused on situations where this treatment alone is not sufficient to eliminate bacterial growth from the uterus. Suggested presence of biofilms, dormant bacteria in the deeper layers of the endometrium, and other barriers may prevent antibiotics from reaching their target and effectively eliminating bacteria.77-79 Although further evidence may be needed to conclusively confirm some of these hypotheses, their suggestive presence in the uterus have given rise to multiple treatment options to accompany or replace traditional antibiotics. The medical value of most of these treatments is often anecdotal rather than evidence based. ■ TABLE 43.6 Antibacterial Drugs Used for Intrauterine Administration for Treatment of Uterine Infections in Mares
N-acetylcysteine (NAC): This mucolytic substance has been used to reduce the viscosity of mucus in the uterus. In addition, NAC has been suggested to have antiinflammatory, antioxidant, and antibacterial activity.80 Typically, 30 mL of a 20% solution NAC (200 mg/mL) is diluted in 150 mL of saline and infused into the uterine lumen during estrus, followed by ecbolic treatment or uterine lavage 12 hours after treatment. The treatment protocol has been suggested to be beneficial both 24 to 48 hours prior to breeding and 24 hours prior to antibiotic treatment. Repeated lavage may be indicated if the effluent fluid is cloudy.81 When used together with antibiotics, the interaction with antimicrobials should be kept in mind. NAC enhances the efficacy of β-lactams but reduces the antibacterial activity of aminoglycosides, fluoroquinolones, and erythromycin. Oral treatment with NAC at 10 mg/ kg did not reduce viscosity of uterine mucus; however, an antiinflammatory effect was observed in one study.82 NAC was also suggested to decrease biofilm biomass and reduce bacteria within biofilms of E. coli isolates in vitro.79 The same effect, however, was not observed for other bacteria. Intrauterine treatment with NAC is sufficiently proven to be safe and has been suggested to improve pregnancy rates, although the pregnancy data were not supported by 77 controlled experimental conditions.77 EDTA-Tris: Tricide® (a third-generation chelator) chelates calcium and magnesium within the bacterial cell wall, which may potentiate the effect of the antibiotic.83 It has been suggested to potentiate the effect of antibiotics on some bacteria, but its effect to disrupt gram-negative biofilms is less clear.79 Treatment protocols often consist of intrauterine infusions of 250 to 750 mL Tricide followed by uterine lavage with a buffered saline solution the next day. The treatment is repeated until the effluent fluid is clear, at which time the mare is treated with local antibiotics for 5 days. Tricide can also be added to antibiotics but is not recommended for use together with ceftiofur, penicillin K, or Timentin due to precipitation in the solution.81 Cationic steroid antimicrobial (CSA): Ceragyn® belongs to a class of peptides that cause depolarization of bacterial cell wall membranes and activate apoptotic pathways. These peptides have been used for various conditions in human medicine because of their biofilm breakdown and broadspectrum antimicrobial activities. Ceragyn (60 mL; 1 vial) is labeled for use up to 24 hours before or 12 to 48 hours after breeding. The drug has become increasingly popular among equine practitioners, but the authors have not been able to find conclusive data from controlled studies to support its effect on equine endometritis. Hydrogen peroxide: H2O2 has a bactericidal effect on most uterine pathogens. A 1% solution (20 mL of a 3% H2O2 solution diluted in 60 mL lactated Ringer's solution [LRS]) has been suggested to be effective on biofilms in vitro.79 Information regarding the efficacy of H2O2 treatment is anecdotal and needs to be supported by controlled in vivo studies. bActivate: A proprietary substance marketed as bActivate® has been shown to activate dormant Streptococcus spp. from the equine endometrium.78 Dormant bacteria are not sensitive to antibiotics, but after confirmed activation with bActivate, evidenced by a positive culture, mares can successfully be treated with intrauterine infusion of antibiotics. However, fertility data from controlled studies are needed to confirm claims of improved fertility following treatment. Immune Modulators. The immune response of the equine endometrium has been investigated following bacterial inoculation, and treatment protocols aimed at restoring a normal immune response in susceptible mares have been reported.84 Bacterial cell wall extracts: Cell wall extracts of Mycobacterium phlei (MCWE) as well as Propionibacterium acnes have been investigated regarding their effect on the uterine immune system and reproductive performance. Fumoso and col- leagues85 found that MCWE treatment of susceptible mares at the time of breeding resulted in an endometrial immune environment similar to that of resistant mares at 24 hours after AI. In a follow-up study,86 the authors concluded that MCWE treatment was effective in eliminating inoculated bacteria from the uterus in 70% of treated mares at 7 days after infusion. In another study,84 the immune response between 3 and 72 hours after intrauterine inoculation of E. coli was characterized; cytokine expression in MCWE- treated mares was not different from that of untreated mares, but messenger RNA (mRNA) expression of serum amyloid A was suppressed in treated mares. Clinically, MCWE had a favorable effect on the clearance of pathogens and fluid retention.84 These results supported a comprehensive clinical study in which problem mares were treated with P. acnes extract (Settle®); the authors found a 10% increase in pregnancy rates compared to untreated controls.87 However, the mares received additional treatments and the effect of stallion fertility was not considered in that study. Plasma: Intrauterine infusion of autologous or heterologous plasma has been used to treat mares with infectious endometritis.88 The rationale for the treatment was to add immunoglobulins and complement to assist the mares in eliminating pathogens from the uterus. Supplementation of fresh or cryopreserved PMNs into the uterine lumen in mares with persistent endometritis has also been proposed 8991 as an alternative treatment to antibiotics.89-91 PERSISTENT BREEDING-INDUCED ENDOMETRITIS. Management of mares susceptible to persistent breeding-induced endometritis should include limiting uterine exposure to semen and bacteria and assisting the uterus to physically clear contaminants and inflammatory products after breeding.30,92 Preexisting uterine infections should be resolved before the mare is bred. Exposure to semen should be limited to a single breeding per cycle, if possible. This can be accomplished by closely monitoring follicular development and hormonal treatment to induce ovulation of mature follicles. Woodward and colleagues37 found that the imbalance of proinflammatory cytokines and inflammatory cytokines in response to semen in susceptible mares is present already within 3 to 6 hours after insemination. This information should serve as a guideline for timing of treatments in susceptible mares after insemination. Uterine lavage: Infusion of 1 to 2 L of buffered saline solution after breeding is effective in removing accumulated fluid and inflammatory products from the uterus. Because sperm transport to the oviduct is completed within 4 hours after breeding, uterine lavage 6 to 24 hours after breeding will not have a negative effect on fertility.53 The uterine lavage is typically repeated until the recovered effluent fluid is clear. The treatment is often combined with an ecbolic drug in order to facilitate recovery of the infused fluid.81,90,92 Manual dilation of the cervix in mares with poor cervical dilation may help these mares more effectively clear the uterus of fluid. Ecbolics. The administration of ecbolic drugs after breeding is effective in overcoming impaired myometrial contractility 9395 in susceptible mares.93 95 Oxytocin: Low doses of oxytocin appear to be more effective than high doses.96 A common treatment protocol is 10 to 20 IU of oxytocin 4 to 6 hours after breeding, repeated every 6 to 8 hours until the intraluminal fluid has disappeared. The half-life of oxytocin is relatively short, resulting in approximately 50 minutes of myoelectric activity after the administration of 10 IU.97 Carbetocin: Carbetocin is a long-acting oxytocin analog with an extended half-life after administration of 0.175 mg IV.98 Limited data are available on the efficacy of carbetocin versus oxytocin. Prostaglandin: PGF2α has considerably longer duration on uterine contractility compared to oxytocin.95 Treatment is not recommended after ovulation, since PGF2α and its analogs can cause a delay in the formation of a functional CL when administered within 2 days after ovulation.36-39 It is the authors' observation that luteolytic doses of PGF2α are excessive and may cause myometrial “cramp” initially rather than a physiologic contraction that would be more suitable for removing fluid from the uterus. A suitable dose of PGF2α and its analogs for treatment of equine endometritis has not been established. In severe cases of persistent breeding- induced endometritis, ecbolic treatment is often combined with uterine lavage with 1 to 2 L of buffered saline 6 to 12 hours after breeding.81 Social interaction with a stallion: Social interaction with a stallion may facilitate normal uterine clearance following breeding. Audio, visual, and physical exposure of mares to a stallion stimulated pituitary oxytocin release and caused uterine contractions.100 This observation was confirmed in a subsequent report.101 Housing susceptible mares close to a tease stallion after breeding may therefore enhance normal uterine activity and clearance. Immune Modulators. The immune response of the equine endometrium has been investigated following insemina- tion,37 and treatment protocols aimed at restoring a normal immune response in susceptible mares after breeding have been reported. Corticosteroids: Several studies support a positive clinical effect of corticosteroids on persistent breeding-induced endometritis. A single dose of dexamethasone (50 mg at the time of breeding) was found to improve pregnancy rates in mares with more than three risk factors for susceptibility to persistent breeding-induced endometritis.102 Researchers from Belgium did not observe a positive effect of treatment with 10 mg or 20 mg of dexamethasone 6 to 12 hours after AI in a large group of unclassified mares,103 emphasizing the importance of correctly identifying mares as susceptible to persistent endometritis before implementing treatment regimens. Furthermore, mares with a history of excessive postbreeding inflammation had significantly higher pregnancy rates when treated with acetate 9-α-prednisolone (0.1 mg/kg) twice daily compared to control cycles.104 Although the immune modulation appears to favor resolution of inflammation, it does not mimic that of resistant mares.105 Recent observations suggest that dexamethasone suppresses the proinflammatory cytokine interleukin-1β (IL-1β) in susceptible mares at 6 hours after breeding.106 However, no effect was observed for modulating cytokines, which previously had been suggested to differ between susceptible 37 and resistant mares.37 Nonsteroid antiinflammatory drugs (NSAIDs): Because of its modulating effect on inflammation, treatment of susceptible mares with NSAIDs has been studied.107 Oral administration of Vedaprofen (2 mg/kg) the day before AI, and of 1 mg/ kg twice daily until one day after ovulation, had no effect on fluid accumulation or uterine cytology but resulted in higher pregnancy rates. It should be noted that the mares were also treated with oxytocin (20 IU) three times per day. More research is needed to determine the potential value of this treatment protocol. Bacterial cell wall extracts: Studying the immune response to semen, Woodward and colleagues105 found that MCWE downregulated mRNA expression of IL-1β in susceptible mares at 6 hours after AI, supporting previous observations by Fumuso and colleagues.108 As noted under infectious endometritis, a comprehensive clinical study suggested that treatment of problem mares with P. acnes extract (Settle®) resulted in a 10% increase in pregnancy rates compared to untreated controls.87 However, the mares received additional treatments and the effect of stallion fertility was not considered in that study. Plasma: The use of plasma products has recently been directed toward immunomodulation rather than elimination of pathogens from the uterus. Platelet-rich plasma (PRP) was shown to modulate the uterine inflammatory response to semen,109,110 including downregulation of mRNA coding for proinflammatory cytokines and NO.111 The protocol for treatment with PRP entails separation of 180 mL of whole blood by a special centrifugation system (Angel Cytomedix, Inc., Gaithersburg, Md.) followed by resuspension of the PRP in 10 mL plasma before the mix is being infused into the uterus at 24 to 36 hours prior to breeding. Lactoferrin: Recombinant human lactoferrin (rhLF) has been demonstrated to be safe to administer in the equine uterus and modulates breeding-induced inflammation.112 It was concluded that intrauterine treatment with 250 μg/mL rhLF may assist susceptible mares to resolve the breeding-induced inflammation in a timely fashion. Clinical trials are needed to confirm this observation. Electroacupuncture has been used clinically to increase uterine contractility in mares with delayed uterine clearance. Anecdotal reports are encouraging, and further research is necessary. It is important for the clinician to keep in mind that a transient inflammatory response to semen is normal. Postbreeding treatment of these mares most likely will not improve fertility but may cause even further contamination and interfere with pregnancy. Only 10% to 25% of all broodmares develop a pathologic, persistent form of breeding-induced endometritis.19-21 Attention should be given to identifying and managing these mares appropriately in order to optimize reproductive efficiency. CHRONIC DEGENERATIVE ENDOMETRITIS (ENDOMETRIOSIS). Degenerative changes of the endometrium such as periglandular fibrosis and glandular dilation are often seen in older multiparous mares. The condition is associated with susceptibility to persistent endometritis68 and may result from repeated uterine inflammation. However, the condition has also been observed in older mares without any known history of endometritis, suggesting that degenerative fibrosis of the endometrium can be a process of aging rather than inflam- mation.113 Because of the possibility of a noninfectious cause of the disease, it was suggested that the condition should be called endometriosis, rather than degenerative endometritis.113 It is not clear why mares with fibrotic degenerative changes to the endometrium have an impaired physical uterine clearance mechanism. Sclerotic changes in the uterine vascular bed impair blood flow to both the endometrium and the myometrium, which may explain the effect on uterine clearance.114 Several treatments have been suggested for degenerative fibrosis of the endometrium, but consistent results have not been reported. Infusion of dimethyl sulfoxide (DMSO) into the uterine lumen has produced inconsistent results in mares with chronic degenerative endometritis.115,116 The use of mesenchymal autologous stem cells and autologous conditioned serum has been explored in experimental models as potential treatment alternatives for susceptible mares and mares with degenerative endometrosis.117-119 A modulation of the inflammatory response to semen was reported as was an indication that regenerative treatment strategies have the potential to restore degenerative changes to the endometrium. Prognosis and Prevention. Prognosis for fertility after endometritis varies with the severity of inflammation and fibrosis and the inciting cause. Prognosis should take into account the age of the mare, the level of reproductive management, the cause (if known), and the most probable response to treatment. Metritis Metritis is classically defined as inflammation of all layers of the uterine wall. Metritis occurs in the first 2 weeks after foaling and commonly follows abortion, dystocia, and RFMs. Equine metritis is often accompanied by endotoxemia and laminitis. Transluminal adhesions between endometrial folds may follow severe metritis. ■ Clinical Signs and Diagnosis Metritis is characterized by uterine accumulation of postpartum secretions, bacteria, and the products of inflammation, with discharge from the cervix and possibly the vulva. Discharge is usually fluid and red-brown and may be fetid. Systemic signs of depression accompanied by neutropenia and leukopenia are apparent with development of endotoxemia. Differential diagnoses include normal lochia and causes of profound depression in the postpartum period as a result of uterine tears and acute abdominal disorders. ■ Treatment and Prognosis Treatment is directed toward removing contamination and microorganisms from the uterus while providing systemic treatment for endotoxemia. Broad-spectrum systemic antibiotics, antiinflammatory drugs, and fluid therapy are indicated. Uterine contamination may be removed by gentle intraluminal infusion of warm water or saline and siphoning off of uterine contents. Vigorous lavage should be avoided, particularly during acute systemic disease. Prognosis depends on severity of clinical signs. If metritis is diagnosed quickly and treatment is instituted, prognosis for fertility and systemic health is good. Prognosis is guarded once endotoxemia and laminitis develop. Pyometra Pyometra in mares is an accumulation of purulent exudate in the lumen of the uterus. Impedance to mechanical uterine outflow, such as cervical fibrosis and adhesions of cranial parts of the tract ventrally into the abdomen, often contributes to the development of pyometra. If endometrial irritation causes release of endogenous endometrial PGF2α, diestrus will be shortened. In some mares, endometrial destruction is so severe that PGF2α release is inadequate and luteal life is prolonged.27 A variety of bacteria may be involved, including E. coli, Pseudomonas spp., and Streptococcus spp. Cultures may also be negative. ■ Clinical Signs and Diagnosis A purulent vaginal or cervical discharge may be seen. The mare may demonstrate a short diestrus, a normal interestrous interval, or a prolonged diestrus. Some mares with pyometra have mild leukopenia and normocytic-normochromic anemia, secondary to mild suppression of erythropoiesis. Transrectal palpation and ultrasonography reveal a fluid-filled uterus. The uterine wall may be thin and flaccid or thick. ■ Treatment and Prognosis Treatment should involve correction of predisposing causes, fluid evacuation, and local antibiotic treatment. Evacuation of large amounts of fluid from the uterus may result in redistribution of fluid and circulatory shock. The mare should be monitored for signs of circulatory shock, and intravenous fluid may be administered during evacuation of large amounts of fluid from the uterus. The prognosis for life is excellent; however, the prognosis for return to normal fertility is guarded to poor because the conditions that predispose to development of pyometra in mares (cervical stenosis and adhesions) are difficult to treat and because severe endometrial destruction may develop. Endometrial biopsy should precede vigorous treatment. Hysterectomy should be considered if treatment is unsuccessful and if discharge is unacceptable or if adhesions impair athletic ability. ■ Ruminants Bovine Uterine Infection Deliveries complicated by dystocia or RFMs may be followed by severe bacterial infections of the uterus. The most sanitary environment possible should be provided for calving. The use of a clean pasture may be most appropriate on some farms, whereas the use of roomy, well-bedded, indoor maternity pens that are cleaned after each delivery may be appropriate on others. Cows with abnormalities such as hypocalcemia, dystocia, and RFMs around the time of calving are more likely to develop uterine infections than are cows that calve normally. Routine treatment of cows with antibacterial drugs and chemicals has not been shown to be beneficial and may in fact reduce fertility. Postpartum uterine infections may be prevented, or the number of such infections reduced, by strict attention to sanitation in the calving environment and during assistance with delivery, along with proper management during the dry period.1 Bovine uteri are normally contaminated by a wide variety of microorganisms during the puerperium. Most of the organisms are transient residents of the reproductive tract and are soon eliminated from the involuting uteri of normal cows. T. pyogenes can persist in the uteri of cows and act with Fusobac- terium necrophorum and Prevotella (formerly Bacteroides) spp. to cause uterine infections. Coliforms, P aeruginosa, hemolytic streptococci, and gram-positive and gram-negative anaerobic bacteria are also frequently isolated from animals with postpartum uterine disease. T. pyogenes and Clostridium spp. occasionally colonize the postpartum uterus synergistically, causing severe gangrenous metritis. Other organisms that appear to have little effect on fertility may colonize the uterus and produce penicillinase, thus influencing the selection and route of administration of drugs used to treat uterine infections.2,3 ■ Clinical Signs and Diagnosis Lochia is normally expelled during the first 2 weeks after calving and may range from dark red or brown to white to clear. If uterine involution is delayed, discharge of lochia may continue until 30 days after calving. Discharge of lochia is not abnormal unless the fluid is fetid or the cow develops other abnormal clinical signs. Abnormalities of uterine involution cannot be diagnosed by palpation per rectum during the first several days after calving when both normal and abnormal uteri are out of reach and cannot be safely retracted. By 10 to 15 days after calving, the entire uterus can be palpated if involution is normal. Fluid should not be palpable within the uterine lumen by 14 to 18 days after calving. Gross reduction in size and histologic repair of the endometrium are complete in dairy cows by 40 to 50 days after calving. Postpartum metritis in cows is characterized by the presence of variable amounts of lochia within the uterine lumen that may be discerned by palpation per rectum. A vaginal discharge is usually present, but it may become obvious during palpation. Septic or puerperal metritis is characterized by clinical signs of toxemia that may include fever, depression, partial or complete anorexia, and laminitis. Milk yield is depressed, and cows may be unwilling or unable to rise. Some cases may be complicated by tenesmus. Vaginitis and cervicitis may accompany metritis. Discharges associated with septic metritis vary from scanty white mucus to copious amounts of red to red-black, watery, malodorous fluid. In some cases inflammation may spread through the uterine wall and cause perimetritis and peritonitis.4 Septic metritis in ewes and does is characterized by fever, depression, anorexia, and tenesmus. Endometritis in cattle is usually observed between 2 and 8 weeks after calving. Discharge can range from white pus to estrual mucus. Purulent exudate may be observed only with palpation or may be found in the cranial vagina and cervical canal on examination with a speculum. The history may indicate that the cow has failed to conceive after several services but the patient is otherwise healthy. Culture of endometrial fluid is not usually done in individual cases of bovine uterine infection but may be indicated to determine the antibiotic susceptibility of microorganisms on a particular farm or as a part of the diagnostic plan when the incidence of postpartum metritis or endometritis increases suddenly. Endometrial biopsies are rarely used in cows but have been recommended when complete evaluation is required of the reproductive tracts of cows that do not conceive or that conceive but do not complete their pregnancies. ■ Treatment and Prognosis To be useful in treating uterine infections in cows, an antibiotic must be active against the primary uterine pathogens (T. pyogenes and gram-negative anaerobes), in the presence of organic debris, and in the anaerobic environment of the postpartum bovine uterus.5 Oxytetracycline is active against many of the microorganisms that infect the bovine uterus, and its activity is only slightly reduced by organic debris and absence of oxygen. Intrauterine treatment with administration of 4 to 6 g of oxytetracycline per day has been used; however, some preparations of oxytetracycline irritate the endometrium, cervix, and vagina. Intrauterine antibiotic treatment of dairy cows results in residues in their milk.6 For example, oxytetracycline has been found in milk from 447 to 968 hours after intrauterine administration, and thus an appropriate withdrawal period should be enforced and milk residue testing should be conducted. Penicillin by systemic administration is effective for treatment of uterine infections in cows. Doses of penicillin required to reach the minimum inhibitory concentration of T.pyogenes are 10,000 to 20,000 IU/kg/day. Systemic ceftiofur (2.2 mg/kg IM or SC q24h for 3 to 5 days) achieves adequate concentrations in the uterus and is effective in treating bovine metritis.9,10 Treatment of septic or puerperal metritis should be directed toward controlling septicemia. Large doses of broad-spectrum systemic antibiotics are indicated, along with fluids and other supportive therapy. Attempts to remove RFMs or irrigate the uterus are contraindicated during the acute phase of the disease. After the patient has recovered from acute septicemia, intrauterine therapy may be considered. ANTISEPTIC CHEMICALS. A variety of antiseptic chemicals have been infused into the uterine lumen of cows in attempts to treat metritis and endometritis, but few controlled trial evaluations are available. The potential for endometrial damage by these chemicals needs to be considered carefully. UTERINE LAVAGE. Lavage of the uterine lumen with large volumes of warm saline (40° to 45° C [104° to 118° F]) removes accumulated fluid and debris. Uterine lavage has been used as an adjunct to antibiotic, antiseptic, and plasma treatment. Catheters designed for nonsurgical embryo recovery are suitable for uterine lavage. Saline is infused into the endometrial cavity in 0.5- to 1-L increments, allowed to reflux through the catheter, and collected for inspection. A milk hose and larger fluid volumes may be used in cattle with larger postpartum uteri, but care must be taken not to enter far into the uterus because it is friable and easily perforated. Massage or partial retraction of the uterus by palpation per rectum may be necessary to increase fluid recovery. The uterine lumen is lavaged repeatedly until the fluid returning through the catheter is no longer turbid. PROSTAGLANDINS. In cows, repeated administration of PGF2α results in shortened estrous cycles and may mimic the shortened luteal phase of patients with acute endometritis. PGF2α therapy alone may be sufficient in mild cases of endometritis, or it may be used in combination with intrauterine or systemic therapy. In cases of chronic bovine endometritis, treatment with PGF2α one or two times at 10- to 14-day intervals decreased the number of days open.11 The prognosis in cows for recovery from endometritis is usually good if the condition does not progress to a more severe form of uterine disease. Septic metritis after dystocia or RFMs may result in permanent impairment of reproductive function, laminitis, or death of the patient despite aggressive therapy. Pyometra In dairy cows, pyometra is likely to develop in cows that ovulate before microorganisms that infect the uterus during the postpartum period are eliminated. The CL that develops after the first postpartum ovulation at approximately 15 to 18 days after calving persists, possibly because the abnormal uterine contents suspend release of PGF2α from the endometrium or sequester it within the uterine lumen. The uterus is brought under the influence of progesterone, which depresses phagocytic activity of uterine neutrophils and closes the cervix, allowing the bacterial infection to persist.12 Pyometra rarely endangers the general health or life of affected cows. Postcoital pyometra may be caused by T. foetus in natural breeding dairy and beef herds.13 PGF2α is the treatment of choice for bovine pyometra. Treatment is followed in 3 to 6 days by uterine evacuation in 85% to 90% of treated cows. Response to PGF2α treatment may be bolstered with a repeat injection in 6 to 12 hours. After endometrial lesions are allowed to heal for 30 days, fertility is restored in most patients. Treatment of cows with GnRH after calving is controversial. In herds with a high prevalence of postpartum uterine infections, treatment with GnRH may decrease fertility by inducing ovulation and CL development; thus the uterus is brought under the influence of progesterone before contaminating bacteria are removed, leading to pyometra. Perimetritis Perimetritis may occur in all species as a sequela to severe uterine infections, uterine rupture, penetration of the vagina during mating, traumatic insemination or obstetric procedures, and cesarean section.14 Perimetritis is characterized by inflammation of the peritoneal surface of the uterus and may be accompanied by localized or diffuse peritonitis. Adhesions then develop between the uterus and other pelvic and abdominal organs. ■ Clinical Signs and Diagnosis The clinical signs of perimetritis are those of peritonitis and may include fever, depression, partial or complete anorexia, stasis of the gastrointestinal tract, and evidence of abdominal pain. Abdominal pain is typified by colic in mares and by grinding the teeth (odontoprisis) in cows. In cows the condition should be differentiated from traumatic reticuloperitonitis, displacements of parts of the digestive tract, abomasal ulcers, postpartum metritis, and abdominal fat necrosis. Perimetritis in mares must be differentiated from other causes of colic. Antemortem diagnosis of perimetritis is difficult in sheep and goats that are presented mainly with fever, depression, anorexia, and odontoprisis. ■ Clinical Pathology Cases of acute perimetritis are accompanied by leukopenia, neutropenia, and a degenerative left shift. Further evidence of peritonitis is obtained when peritoneal fluid is obtained by paracentesis and examined for its cellular and microbiologic content. ■ Treatment and Prognosis The cause of perimetritis should be treated if possible. Cases of severe metritis should be treated appropriately, and uterine ruptures sutured if possible. Repair of uterine ruptures inaccessible by flank incisions may be facilitated by intentional prolapse of the uterus after administration of epinephrine, provided the tear is not too close to the cervix (see next section). Treatment with broadspectrum systemic antibiotics is indicated. Lavage to remove peritoneal exudate has been recommended but is difficult to accomplish, especially in cows in which the rumen, abomasum, and greater omentum make ventral drainage almost impossible and in which fibrinous peritonitis with loculation of infection occurs rapidly. Other supportive treatments such as intravenous fluids and antiinflammatory drugs should be administered. The prognosis depends on the severity of lesions. Fatalities can occur despite prompt treatment, and surviving animals may be infertile because of mechanical interference with gamete transport caused by adhesions between the genital organs and other pelvic and abdominal tissues. In general, the prognosis for fertility in affected animals is fair at best. ■ Prevention and Control Perimetritis occurs sporadically in individual animals; therefore prevention depends on avoiding the causes. Immature females, especially heifers and fillies, should not be allowed at pasture with adult males to prevent undesired mating complicated by penetration of the vagina. Traumatic obstetric, insemination, and uterine lavage procedures must be avoided. Uterine tears that occur at parturition must be sutured immediately. Postpartum metritis must be treated promptly and appropriately before it progresses to perimetritis. ■ Small Ruminants Uterine infections may follow dystocia and RFMs in sheep and goats, but these infections are not frequently a cause of infertility because in most cases parturition is followed by a few months of sexual rest before the next breeding season. In ewes, RFMs and metritis follow abortion caused by Listeria monocytogenes, Campylobacter spp., and Chlamydophila abortus. Ewes and does affected with metritis are usually treated with systemic antibiotics such as penicillin, sulfamethazine, oxytetracycline, or ceftiofur. Early and aggressive treatment is indicated. ■ Camelids Metritis and Endometritis When camelids breed, the penis is inserted through the cervix and deep into the uterine horns. Unnecessary mating, or overbreeding, is the most important factor causing damage to and contamination of the uterus.15 Other major contributing factors include RFMs, rectal vaginal tears, and unsanitary obstetric manipulations.15 Chronic endometritis will often not cause evident clinical signs, whereas acute, postpartum endometritis may cause fever, depression, and signs of shock. A thick, mucoid lochial discharge is normal in the postpartum female for up to a week postpartum. In contrast, thin, watery, fetid discharge is a sign of endometritis.15 Transrectal ultrasonography and vaginoscopy are helpful in diagnosing endometritis and metritis. Inflamed, thickened uterine walls and hyperechoic, intraluminal fluid may be present on ultrasound examination. Vaginoscopy may reveal cervical discharge. Transrectal ultrasonography may usually be performed in llamas. In alpacas, because of smaller size, an extension probe is necessary to facilitate transrectal ultrasonographic evaluation. Uterine culture and cytology samples from the llama may be obtained using methods similar to those used in the mare and cow. A double-guarded swab prevents environmental contamination. In the alpaca, the swab should be passed through the cervix via visualization using a vaginoscope. These diagnostics should be performed during the peak follicular phase to ensure ease of passage through the open cervix and more reliable test results.15 The most common bacteria isolated from the uteri of camelids with endometritis are E. coli, S. zooepi- demicus, β-hemolytic streptococci, Enterococcus, coagulasenegative Staphylococcus, Proteus spp., Enterobacter aerogenes, K. pneumoniae, and T. pyogenes.15 Uterine biopsy can be a useful diagnostic tool for evaluation of metritis and endometritis in camelids. Endometrial biopsy samples in llamas may be obtained as in the mare. The left horn is perhaps better to target unless a particular pathology is suspected in the right horn, because camelid pregnancies almost always occur in the left horn.15 Pathologic changes, evaluation, and prognosis are all assumed to be similar to those in the mare. Treatment for endometritis and metritis is also similar to that described for the mare. Uterine lavage with a warm, isotonic saline solution and oxytocin injection (5 to 10 IU) are the major components of treatment. Intrauterine antibiotic infusion is done after uterine lavage. The most common antibiotics used are penicillin K (1.5 ? 106 U), gentamicin sulfate (200 to 300 mg), and ceftiofur sodium (250 to 500 mg).15 Antibiotics should be diluted in sterile water or saline (saline should not be used with ceftiofur) and given once daily for 5 to 7 days. Females should be evaluated after cessation of treatment and completion of 2 weeks of sexual rest. Prevention of endometritis often requires a “minimum contamination breeding technique.”15 This entails monitoring follicular growth via transrectal ultrasound until the follicle is of preovulatory size, breeding only once, following breeding with an injection of hCG (750 IU) or GnRH, and administering an intrauterine infusion of antibiotics 24 hours after breeding. Females should be evaluated for pregnancy 12 to 14 days after breeding. Further preventative measures include performing prebreeding examinations on all maiden animals to avoid breeding animals that are too young or do not have follicular activity; breeding only females that exhibit strong receptive behavior (as opposed to mere submissive behavior); performing complete gynecologic examinations on all females with a history of infertility, obstetric problems, or postpartum complications; and observing strict rules of hygiene during breeding and obstetric manipulations.15 Pyometra Pyometra caused by delayed uterine involution may be observed shortly after parturition. Chronic pyometra is often associated with vaginal or cervical adhesions that may be sequelae to trauma after dystocia or aggressive obstetric manipulation.15 Anatomic Defects as a Cause of Uterine Infection The most common anatomic defect associated with genital infections in camelids is pneumovagina. Other defects include urovagina and perineal lacerations. These defects should be corrected to prevent contamination with environmental and fecal organisms. Endometrial Cysts and Lacunae ■ Mares Endometrial cysts and lymphatic lacunae are common degenerative changes of the endometrium that are more prevalent in mares older than 11 years of age than in younger mares.16 Endometrial cysts can originate from endometrial glands or obstructed lymphatics. Glandular cysts are small (and Prognosis The prolapsed uterus should be washed with clean saline and replaced manually in the standing mare as rapidly as possible. Replacement is aided by sedating the mare and administering epidural anesthesia. The uterus should be supported on a clean sheet held at the level of the pelvis. The uterus should be replaced, beginning with the uterine body and working gradually, replacing the tip of the horns last. Correct positioning of the uterus is important to prevent the prolapse from recurring. Replacement should be followed by treatment with broad-spectrum antibiotics, antiinflammatory drugs, and intravenous isotonic fluids. Treatment with oxytocin (10 to 20 IU IM) facilitates uterine involution. Prognosis is related to development of sequelae such as uterine tears, metritis, and endometrial damage.18 ■ Ruminants In cows, most cases of uterine prolapse occur within a few hours after calving. The condition is invariably associated with hypocalcemia, which results in lack of uterine tone and delayed cervical involution. In addition, dystocia frequently precedes uterine prolapse. Elective uterine prolapse can be induced within 6 to 12 hours after calving by administering epinephrine to relax the uterus for the repair of uterine tears. A 10-mL amount of epinephrine (1:1000) is diluted to 250 mL in sterile saline and administered slowly IV. After 100 mL of the solution has been given, the operator reaches through the cervix, grasps the uterine wall and caruncles, and everts the uterine horn toward the cervix. When sufficient uterine tissue has entered the cervical canal, the patient responds by straining, which assists in completion of the prolapse. Epidural anesthesia is administered to abolish further straining after the prolapse is complete. Uterine prolapse in does has been associated with dystocia, hypocalcemia, and lack of exercise. The predisposing factors are probably similar for ewes. ■ Clinical Signs and Diagnosis Clinical signs of uterine prolapse are obvious, with maternal caruncles exposed on the uterine endometrium. The membranes may remain attached. Immediately after prolapse occurs the tissues are nearly normal, but within a few hours they become enlarged and edematous. The endometrium is usually contaminated with feces and bedding material. In some cases the prolapsed tissue may be lacerated or severely traumatized and may contain loops of intestines. Clinical signs that may accompany uterine prolapse include straining, abdominal pain, restlessness, anorexia, and increased pulse and respiratory rates. Parturient paresis is common in affected dairy cows. In most patients these signs are transitory, but shock may complicate some cases. ■ Clinical Pathology Uterine prolapse in cows is frequently accompanied by hypocalcemia and a significant increase in the packed cell volume.19 ■ Treatment and Prognosis The prolapsed tissue should be protected from further damage by wrapping it in wet towels or covering it with a plastic bag. Beef cows should be restrained where they are found, to prevent trauma to the uterus or rupture of the large uterine vessels should an animal try to escape on arrival of the clinician. Treatment of hypocalcemia is usually indicated before replacement of the uterus if the cow is recumbent and semicomatose; otherwise calcium gluconate is administered after replacement. Epidural anesthesia (3 to 5 cc of 2% lidocaine) is frequently, but not always, required. The prolapsed tissue is washed with a mild presurgical scrub. The membranes are removed if they can be easily separated from the endometrium but are left in place if removal is difficult. Some clinicians recommend that cows stand during replacement, whereas others have found that the organ can be replaced in recumbent cows if the patient is placed on her sternum with the hind legs drawn straight out behind. The prolapse is placed between the extended limbs. In fresh cases, replacement is relatively easy and is begun at the cervical pole of the organ; the dorsal and ventral parts are massaged alternately back into their normal position. After the ovarian pole has been replaced, the previously prolapsed horn must be straightened and eversion of the uterus corrected; this can be done manually or by intrauterine infusion of warm saline. Administration of clen- buterol is reported to relax the uterus, facilitate replacement, and reduce the need for epidural anesthesia, but its use is illegal in the United States. If the patient has been neglected, accumulated fluid must be reduced by lubricating the tissue with an emollient ointment and then carefully but vigorously massaging the tissue from the ovarian pole toward the cervical pole. The hygroscopic action of sugar when applied liberally to prolapsed uteri is of questionable value. Oxytocin (5 to 40 IU IM or IV) is frequently administered to stimulate myometrial contractions after the uterus has been replaced. Metritis is a frequent sequela, and appropriate antibiotic treatment is indicated in most cases. Temporary closure of the vulva with heavy sutures after replacement may not be necessary but is practiced by many clinicians. If replacement of the prolapsed uterus is impossible or the tissue is severely traumatized, amputation may be indicated; in this case it is important that the uterine arteries be double ligated.20 Euthanasia may also be considered in such instances. The prognosis varies but is generally favorable if there has been no serious damage to the uterus. Fatalities can occur in cases complicated by shock or by rupture of large uterine vessels. The culling rate from infertility of cows with uterine prolapse is higher than that of their herdmates, and the calving interval is prolonged in affected cows. Barring hypocalcemia, the risk of uterine prolapse at a subsequent calving is no greater than for other cows in the herd. ■ Prevention and Control Because the condition is associated with hypocalcemia in cows, provision of a properly balanced ration before calving is indicated. Although uterine prolapse can occur after an apparently normal delivery, it is more commonly associated with dystocia and forced extraction; therefore prolapse should be anticipated, and the dam observed so that affected patients may receive prompt treatment. Oxytocin (5 to 40 IU IV or IM) may be administered after a dystocia to increase uterine tone and potentially prevent prolapse. ■ Camelids Uterine prolapse in camelids is usually a consequence of dystocia, RFMs, or excessive obstetric manipulation. Treatment is the same as described for other species. Uterine Tumors Neoplasia uncommonly affects the uterus of domestic animals. Leiomyomas are usually benign and arise from the outer smooth muscle of the uterus without need for a preparatory event. Leiomyomas are not necessarily associated with reproductive failure, and tumors and fetuses can coexist. The multicentric form of lymphosarcoma may affect the uterus of cattle. Lymphosarcoma also affects does, but a predilection for the uterus is not apparent. Uterine walls affected by lymphosarcoma may contain discrete neoplastic nodules or be diffusely infiltrated. Carcinomas, chorionepitheliomas, fibromas, fibrosarcomas, rhabdomyosarcomas, and adenosarcomas are rarely reported. Regardless of tumor type, tumors must be differentiated from normal fetuses, mummified or macerated fetuses, placentomes, abscesses, and fat necrosis. Segmental Defects Segmental aplasia (white heifer disease) occurs sporadically in all breeds of cattle. In most cases the cranial parts of the genital tract (ovaries, uterine tubes, and cranial part of the uterine horns) are normal, and endometrial secretions from the parts of the uterine horns accumulate because normal drainage through the cervix is impeded. Various defects may be found in affected animals, ranging from nearly complete absence of tubular genital organs to an imperforate hymen that blocks secretion drainage from a normal genital tract. ■ Clinical Signs and Diagnosis Segmental aplasia may be associated with a history of anestrus if fluid accumulation within the uterine horns interferes with release of PGF2α and luteolysis. Other presenting history may involve infertility or difficulty in AI. On palpation per rectum, various degrees of aplasia may be recognized. Fluid-filled parts of the uterine horns may suggest pregnancy, from which they must be differentiated. An imperforate hymen may bulge from the vulvar cleft and may be confused with vaginal prolapse, prolapse or eversion of the urinary bladder, cystic vestibular glands, or neoplasia of the vulva or vagina. ■ Treatment and Prognosis The only form of segmental aplasia amenable to treatment is that in which an imperforate hymen occludes an otherwise normal tract. Incision of the hymen is followed by drainage of accumulated secretions and may allow the tract to function normally. Paramesonephric Duct Aplasia Aplasia of one paramesonephric duct leads to development of one uterine horn (uterus unicornis). The condition is found in cattle but is rare. Subfertility is the result of prolonged periods of anestrus caused by a persistent CL on the ovary ipsilateral to the missing uterine horn (no local luteolytic signal). The condition can be managed with exogenous PGF2α in the hope that ovulation will occur on the intact side. Alternatively, the unaccompanied ovary can be surgically removed. Uterus Didelphis The caudal parts of the paramesonephric ducts may not fuse properly in cattle, causing duplication of various parts of the caudal tubular tract. Abnormalities of fusion are most common in and around the cervix. The entire cervix may be duplicated, or the cervix and vagina may be normal, with the exception of the presence of a band of tissue extending dorsal to ventral across the external os of the cervix. Partial failure of fusion may involve a part of the cervix, and the affected animal may possess a single uterine body and internal cervical os, duplication of a part of the cervical canal, and a doubled external cervical os. Uterus didelphis results when the cervix and uterine body are completely duplicated. Affected cows may conceive after natural service or if artificially inseminated through the cervix and uterine horn ipsilateral to the ovary about to ovulate. Affected animals may be unable to carry a pregnancy to term because of lack of placental attachment in the nongravid horn. Hydrometra (Pseudopregnancy in Small Ruminants) Hydrometra occurs sporadically in sheep and goats and is characterized by accumulation of several liters of clear fluid within the uterus, abdominal distention, persistence of a CL, and subsequent anestrus.20 Previous breeding is not necessary, but the condition may develop after mating, and does are frequently assumed to be pregnant. It can also occur after early embryonic loss in goats or sheep. The cause of hydrometra is unknown, but a deficiency in production or release of PGF2α from the endometrium has been postulated, as has exposure to phytoestrogens. The clinical signs of hydrometra mimic those of pregnancy. The diagnosis is suspected if the goat fails to show estrus when it cannot possibly have been bred but is in a herd where heat detection is good. Serum progesterone concentrations are elevated, and abdominal enlargement suggestive of pregnancy may occur. Blood-based biochemical pregnancy markers will be negative. Amplitude-depth ultrasound for pregnancy is positive because of fluid in the uterus. Transabdominal ultrasound reveals anechoic fluid but no fetus or caruncles in the uterus. The animal should be rechecked if fewer than 40 days have elapsed since the last possible breeding, as early pregnancy is possible in such cases. In advanced hydrometra, large anechoic fluid-filled compartments are seen separated by undulating tissue walls, which represent the uterus coiled back on itself. Spontaneous correction is common and varies from red discharge suggestive of early abortion to expulsion of accumulated fluid approximately 150 days after an infertile mating, so-called cloudburst. No fetus or placenta is passed. Treatment of false pregnancy is with prostaglandin. The clinician needs to keep in mind that this will induce abortion if the ewe or doe has a true pregnancy. An initial dose of 5 to 10 mg of dinoprost (Lutalyse) or 125 to 250 μg of cloprostenol (Estrumate) is given and repeated in 12 days. Estrus and emptying of the uterus occur in 1.5 to 4 days. Oxytocin (50 IU bid for 4 days) is normally reserved for females that retain fluid in the uterus after prostaglandin therapy. The doe frequently becomes pregnant within a few days to weeks after termination of a false pregnancy if a buck is available. Sometimes hydrometra recurs. Suggestions for prevention have included selenium supplementation and breeding on the first heat of the season. The prevalence is surmised to be increased in herds where breeding is delayed in order to obtain winter milk and in does manipulated hormonally to breed out of season.20 Routine pregnancy diagnosis of sheep and goats with transabdominal ultrasound should be advised to permit rebreeding during the same season. Cervical Abnormalities Cervicitis Inflammation of the cervix usually accompanies endometritis and vaginitis and is frequently secondary to trauma associated with dystocia and obstetric operations. The mucus-secreting epithelium of the cervix is more resistant to bacterial infection than is the epithelium of the uterus and vagina. ■ Mares The equine cervix is a straight tube made up of layered circular and longitudinal muscle. During estrus it relaxes, and the external os lies on the floor of the anterior vagina. During diestrus or pregnancy, under the influence of progesterone, the cervix is closed and the external os is elevated off the vaginal floor. Cervicitis or inflammation of the cervix may be iatrogenic or may occur secondary to trauma associated with parturition or dystocia or as an extension of vaginitis or endometritis. Endometritis and infertility follow if the cervix lacks anatomic integrity. ■ Clinical Signs and Diagnosis Infertility and history of an inciting cause such as urine pooling or dystocia may be the only signs of cervicitis in the mare. Cervical hyperemia and edema may be apparent on speculum examination in acute cervicitis. In more chronic injuries, direct digital examination of the cervix of the mare in diestrus may reveal transluminal adhesions or anatomic defects. For treatment and prognosis in mares, see discussion under Ruminants. ■ Ruminants Similarly, in cows cervicitis is secondary to uterine infections and follows trauma associated with parturition and obstetric manipulations. Infection is usually caused by microorganisms normally present in the cranial vagina such as E. coli, streptococci, staphylococci, and T. pyogenes. Cervicitis in does and ewes is uncommon but may occur secondary to vaginal and uterine infections and obstetric trauma. ■ Clinical Signs and Diagnosis Examination of cows with a vaginal speculum reveals swelling and edema of the external cervical os. The mucous membrane is hyperemic and inflamed. Mucopurulent exudate may be present in the cervical canal or in the cranial vagina. Hypertrophy of the cervix is common in Bos indicus breeds and their crosses and may be a normal finding; therefore cervical size as detected by palpation per rectum may or may not indicate inflammation. Inflammation of the cervix without contemporary endometritis may not affect fertility. Cervicitis may occur in pregnant cows. The clinical signs of cervicitis in does and ewes are similar to those in cattle and must be observed with a small vaginal speculum. ■ Treatment and Prognosis Most cases of cervicitis resolve spontaneously when coexisting endometritis and vaginitis improve. Exudate can be flushed from the cervical canal and cranial vagina with warm saline lavages, and a nonirritating antibiotic ointment applied to the affected tissue. Caustic chemicals should not be placed in contact with the cervical mucosa. Aggressive treatment with systemic antibiotics is indicated in cases complicated by infection with anaerobic bacteria. The prognosis for most cases of simple cervicitis is fair to good. However, inflammation of the cervix in mares may progress to more severe cervical abnormalities. Cervical damage is a serious threat to future reproductive performance in mares. Anaerobic infections of the cervix may be fatal. ■ Prevention and Control Obstetric manipulations and operations must be temperate. When the cervix does not dilate properly during parturition, a cesarean section is preferred over forced extraction. Cervical Lacerations ■ Mares Cervical lacerations are most often seen after dystocia. The condition may result in adhesions and a nonpatent cervix or in failure to seal the uterus during diestrus or pregnancy. Cervical adhesions in combination with endometritis are a common cause of pyometra in the mare. ■ Clinical Signs and Diagnosis Cervical lacerations can be diagnosed by vaginoscopy and digital examination of the cervix. A digital examination of the cervix is often necessary to evaluate the degree and severity of the laceration. Evaluation of the ability of the cervix to close adequately is best performed during diestrus. ■ Treatment and Prognosis If cervical lacerations are diagnosed shortly after parturition, antimicrobial ointment should be applied frequently to the lesion. Early signs of adhesions should be broken down until the tissue is healed. If the laceration results in an incompetent cervix, it should be corrected surgically. Although surgical repair of cervical lacerations has resulted in restored fertility in many mares, the condition is likely to recur at the time of the next parturition. Embryo transfer should be considered if allowed by the breed registry. Vaginal Abnormalities Pneumovagina MARES. Pneumovagina is characterized by aspiration of air, often containing microorganisms, into the vagina. Pneumovagina is secondary to changes in perineal conformation, which include cranioventral displacement of the reproductive tract, loss of integrity of the vestibulovaginal sphincter, and loss of integrity of the vulvar labia. These changes occur more commonly in older, multiparous mares and those that have had perineal lacerations. Pneumovagina is a common antecedent to infertility. ■ Clinical Signs and Diagnosis In the normal mare, the anus is positioned directly dorsal to the vulva. The perineal body between the dorsal vulva and the anus is thick, muscular, and well formed. The vestibulovaginal sphincter is well formed, and the vulva has a vertical alignment, with 80% of the vulval labia situated below the floor of the pelvis. The vulvar labia form a seal in the normal mare. Mares prone to pneumovagina are those in which the vulva tilts horizontally at its dorsal aspect, the perineal body is thin, the vulval labia do not form a seal, and the anus lies cranial to the vulva. A scoring system has been developed to evaluate the perineal conformation in mares.1 The system uses Caslick's index, which equals the distance (in cm) between the dorsal commissure of the vulva and the pelvic floor multiplied by the degrees of declination of the vulvar lips. Mares with a Caslick's index above 150 were found to have subnormal pregnancy rates. Affected mares aspirate air on exercise or when the vulval labia are parted. Aspirated air may be noted on transrectal palpation or vaginal speculum examination. Signs of secondary changes such as vaginitis, cervicitis, or endometritis may be apparent. ■ Treatment and Prognosis Treatment of pneumovagina should be directed toward correcting defective perineal conformation. Cranioventral displacement of the reproductive tract in aged mares may be irreversible. Perineal confirmation in thin mares is often improved by increasing the mare's body condition. Pneumovagina is often successfully corrected by surgical closure of the dorsal vagina via Caslick's surgery. Secondary changes should be treated as described elsewhere. Prognosis for correction of pneumovagina is excellent; however, prognosis for fertility depends on the extent of secondary changes. Urovagina MARES. The normal vagina in young mares slopes cra- niodorsally and is largely contained within the pelvis. With aging and repeated pregnancy, the cranial vagina may slope cranioventrally and fall below the level of the pelvic floor. Under these conditions urine collects in the anterior vagina. Urine is spermicidal, and the condition is often associated with subfertility. ■ Clinical Signs and Diagnosis In mild cases, a history of infertility may be the only indicator of urovagina. In more severe cases, urine dribbles from the vulva at rest or during exercise and may accumulate on the skin of the hindlimbs. Speculum examination reveals a cranioventral slope of the vagina, variable inflammation of the cranial vagina and cervix, and a pool of urine in the ventral vaginal fornix. Urovagina may occur intermittently or only during estrus. ■ Treatment and Prognosis Surgical procedures to prevent the anterior flow of urine include urethral extension2 and vaginoplasty. Prognosis depends on the severity of secondary endometritis and the success of surgery. Vaginitis Vaginitis may occur as a result of ascending infection or exposure to irritants, or secondary to pneumovagina, urovagina, perineal laceration, rectovaginal fistulas, breeding, endometritis, abortion, parturition, or dystocia. Occasionally, traumatic wounds may be infected with clostridial or anaerobic organisms; however, most infection is nonspecific. ■ Clinical Signs and Diagnosis Signs may vary from hyperemia evident on speculum examination to mucopurulent exudation from the vulva. Severe trauma and infection may be followed by necrotic vaginitis with tenesmus, fetid discharge, elevated tail, swollen vulva, and systemic signs. Rapid formation of adhesions follows necrotic vaginitis. Metritis, RFMs, and uterine tears also may show systemic signs and vaginal discharge. ■ Treatment and Prognosis The inciting cause should be treated. Animals with mild vaginitis may recover spontaneously, whereas moderate cases require lavage with dilute antiseptic or antibiotic solutions. Fertility is unaffected in mild vaginitis without extension, and prognosis is good. Severe, necrotic vaginitis is treated with systemic antibiotics, analgesics, and antiinflammatory agents. Caslick's surgery may be necessary to prevent aspiration of air. Local application of antibiotic and steroid-impregnated ointments may help prevent adhesions. Prognosis for severe vaginitis is guarded. Vaginal stenosis and adhesions may follow vaginitis. ■ Prevention and Control Nonspecific vaginitis may be prevented by reducing trauma to the vagina during foaling. Clinicians should elect appropriate methods for relief of dystocia and apply extractive force to fetuses judiciously. Infectious Pustular Vulvovaginitis COWS. Infectious pustular vulvovaginitis (IPV) affects cattle and is caused by bovine herpesvirus 1, also the cause of infectious bovine rhinotracheitis (IBR), although the two strains are genetically distinct.4 Therefore the respiratory and genital forms of the disease rarely occur concurrently, and abortions usually do not follow an outbreak of the genital form of the disease. IPV is spread by coitus and mechanical means and may affect unbred heifers. The incubation period of IPV is short (1 to 3 days), and the infection spreads rapidly through the herd, affecting 60% to 90% of the animals. ■ Clinical Signs and Diagnosis Early in the course of the disease, IPV is characterized by a mucopurulent vaginal discharge, inflammation of the vaginal and vulvar mucosa, and painful urination. Pustules develop over lymphoid follicles and progress from small (to carry both fetuses to term and deliver without dystocia.2 It is much more common for the mare to have a natural reduction to a singleton pregnancy during the embryonic stage or to abort the pregnancy after the fetal stage.3,4 Some breeds are more commonly diagnosed with twins during the embryonic stage (e.g., Thoroughbreds have 20% to 30% double ovulations and 10% to 15% diagnosed twin pregnancies). ■ Clinical Signs and Diagnosis Mares should be evaluated with transrectal ultrasound 13 to 15 days after documented ovulation during a breeding cycle. The ovaries should be examined for more than one active CL, and the uterus should be carefully scanned from the tip of one horn to the other and along the uterine body to the cervix. Equine embryos at this stage are highly mobile within the uterus and may be located anywhere within the uterus. Twin pregnancy should not be ruled out until the entire uterine tract has been scanned for the presence of embryos. After one embryo is found, the remainder of the uterus still must be visualized to ensure the absence of a twin. The embryo proper per se is not visible at this stage of pregnancy, but the embryonic vesicle is easily visualized. Care must be taken not to confuse endometrial cysts with embryos, which sometimes can look deceptively similar. It is helpful to have scanned the mare's uterus using ultrasound before breeding to document the size and location of endometrial cysts. ■ Treatment and Prognosis If twins are confirmed before 16 days of pregnancy, the best way to treat the mare is to manually crush one of the vesicles. This is done by visualizing the twins using transrectal ultrasound and spatially separating them from each other within the uterus. One twin is moved away from the other to the tip of a uterine horn, where it is crushed manually. The remaining embryo should be evaluated 1 to 2 days later to determine its status. Manual reduction of an embryo fixed in the contralateral horn from its twin between days 16 and 20 should be performed at the base of one uterine horn, because embryos are typically “fixed” at this site after day 16. Survival of the remaining embryo is greater than 90% when twin reduction is performed in this manner before day 20.5 ■ TABLE 43.7 Major Causes of Infectious Equine Abortion
PCR, Polymerase chain reaction. It is the established practice of some veterinarians to treat mares with a nonsteroidal antiinflammatory agent (e.g., flunixin) and/or altrenogest after a twin-crush procedure. The reasoning behind this practice is that manual stimulation of the uterus may cause a release of oxytocin, signaling a prostaglandin cascade that will result in luteolysis and complete pregnancy loss. No studies have been performed to support this theory; to the contrary, other studies have shown that the release of prostaglandin after the routine twin-crush procedure does not cause a drop in progesterone and that supplementation with antiinflammatory drugs or progesterone makes no difference in the outcome.5,6 Twins fixed next to each other at the base of the same horn between days 16 and 20 cannot be separated from each other. Manual reduction can still be reliably performed at this stage but will result in the loss of both embryos and the need to breed the mare again on a subsequent cycle. If twins are discovered fixed ipsilaterally between days 16 and 20, the practice of “benign neglect” may be followed for a short time. Since most of these situations will resolve naturally with the resorption of one twin and the persistence of the other, it is a responsible practice to simply monitor the situation to note if one twin regresses. If both twins continue to develop approaching the formation of endometrial cups (day 37 to 38), a decision must be made either to terminate the pregnancy or to refer the mare for advanced, selective twin reduction, which includes transvaginal, ultrasound-guided fetal aspiration7; transcutaneous, ultrasound-guided fetal intracardiac injection of procaine penicillin or potassium chloride8; or craniocervical dislocation.9 The success of these techniques is lower than that of manual crush, and they are performed later in gestation, after the window for manual crushing has been missed. These are all specialty techniques and are beyond the scope of this chapter. Other Noninfectious Causes of Equine Abortion In a survey of causes of equine abortion in the United Kingdom from 1988 to 1997, nearly 39% were caused by umbilical cord pathology.10 Most of the cases (35%) resulted from torsion of the umbilical cord. Twisting of the umbilical cord is common in equine fetuses and often is not pathologic. A diagnosis of abortion caused by umbilical torsion should be made only if localized swelling and discoloration accompany the twisting. Congenital abnormalities may cause abortion. The most common congenital abnormality in equine fetuses is contracted tendons, accounting for 5% of abortions in a study from the United States.1 Fetuses that implant in the uterine body instead of the base of one of the horns develop placental villous atrophy and usually abort, accounting for 2% of abortions in the same study. Infectious Causes Placentitis Placentitis is the leading cause of equine late-term pregnancy loss in the United States.1 Bacterial organisms most commonly cultured from aborted fetuses include Streptococcus spp., E. coli, Pseudomonas spp., Klebsiella spp., Staphylococcus spp., and Leptospira spp. Nocardioform actinomycetes are an important cause of placentitis in central Kentucky and have also been reported in Florida.11-13 Aspergillus fumigatus and Mucor spp. are the most commonly diagnosed causes of mycotic abortion in mares, causing 5% to 30% of infectious equine abortions. The route of placental infection is believed to most commonly be ascending via the cervix, which results in loss of chorionic villi around the cervical star. In addition to loss of chorionic villi, additional allanto chorionic lesions may include nodular cystic allantoic masses, edema, necrotic areas of chorion, and necrotic mucoid exudate coating the chorion. Hematogenous placentitis shows a more generalized, diffuse loss of villi.1 Infection of the placenta results in subsequent infection of the fetus and release of proinflammatory cytokines and prostaglandins from the inflamed placenta, which ultimately leads to mid- to late-term abortion or delivery of a premature foal.14 The distribution of the avillous chorionic lesion classically noted in mares with ascending or hematogenous placentitis does not fit the pattern noted with nocardioform placentitis. Mares with nocardioform placentitis classically show a loss of chorionic microvilli, covered by brownish, thick, and tenacious exudate in a focal area around the ventral aspect of the uterine body and base of the uterine horns. The pathogenesis of nocardioform placentitis is still unresolved. It has been hypothesized that the pathogen is present in the environment or introduced into the mare at the time of breeding and settles in the ventral aspect of the uterus, where infection ensues. Various nocardioform organisms have been reported in soil across the globe, although the pathogenicity of most of these organisms has not been determined. Nocardioform organisms isolated from equine placentas include Amycolatopsis spp. and Crossiella equi.ii∙ii∙i5∙i6 These bacteria have been diagnosed only from clinical cases of placentitis and not from the environment.17 Nocardioform placentitis often results in abortion or premature delivery.1 Bacteria and resulting inflammation are limited to the interface between the chorion and the endometrium. Because no bacterial invasion or signs of inflammation have been observed in the placental and fetal tissues, the abortion is postulated to be due to nutritional deprivation of the fetus resulting from separation between the chorion and endometrium. ■ Clinical Signs and Diagnosis Premature udder development and vaginal discharge are common signs of pending abortion caused by ascending placentitis. However, when these signs are present, the prognosis is poor even when mares are treated. Transrectal ultrasonography of the allantochorion in an area close to the cervix is useful to detect early signs of placentitis and impending abortion (Fig. 43.6).18 Ultrasound evaluations may reveal hyperechoic fetal fluids, placental separation, increased or decreased fetal heart rates (normal range 75 ± 7 bpm19), and thickening of the combined thickness of the uterus and placenta (CTUP). Consistently low or high fetal heart rates are associated with fetal stress. Foals experiencing fetal distress often become bradycardic initially and then become tachycardic in the terminal phase of life.20,21 Serial examinations should be performed to verify fetal well-being or distress. Mares considered “at risk” for pregnancy loss are often examined daily. Fetuses experiencing distress are often evaluated several times a day. Normal measurements of CTUP have been established (Fig. 43.7).18,22 Mares with placentitis may show increased CTUP, edema of the allantochorion, and separation from the endometrium. A 5-MHz linear transducer should be used for transrectal ultrasonography. The transducer should be positioned 1 to 2 inches cranial to the cervical- placental junction and then moved laterally until a major uterine vessel is visible at the ventral aspect of the uterine body.22 The CTUP should then be measured between the vessel and the allantoic fluid (see Fig. 43.6). It is important to obtain all CTUP measurements from the ventral aspect of the uterine body, because physiologic edema of the dorsal aspect of the allantochorion has been noted in normal pregnant mares during the last month of gestation.22 In addition, care should be exercised to be certain that the amniotic membrane is not adjacent to the allantochorion because this may result in a falsely increased CTUP. To examine the placenta from a transabdominal approach, a 3.5-MHz sector transducer is used most frequently. All four quadrants of the placenta should be examined: right cranial, right caudal, left cranial, and left caudal. Measurements of the CTUP can be made with this technique
FIG. 43.6 Transrectal imaging of the combined thickness of the uterus and placenta (CTUP). Measurements of the CTUP (distance between + and +) were recorded from the ventral part of the uterine body, close to the cervix. a, Placenta adjacent to the cervix; b, allantoic fluid; c, amniotic fluid; d, the amnion. (Modified from Renaudin CD, Troedsson MH, Gillis CL, et al.: Ultrasonographic evaluation of the equine placenta by transrectal and transabdominal approach in the normal pregnant mare. Theriogenology, 47:559, 1997.)
FIG. 43.7 Monthly recordings of transrectal ultrasonographic measurements of the combined thickness of the uterus and placenta (CTUP) in normal mares from 4 months of gestation and throughout the pregnancy. Month 4 is 91 to 120 days; month 5 is 121 to 150 days; month 6 is 151 to 180 days; month 7 is 181 to 210 days; month 8 is 211 to 240 days; month 9 is 241 to 270 days; month 10 is 271 to 300 days; month 11 is 301 to 330 days; month 12 is 331 to 360 days. (Modified from Renaudin CD, Troedsson MH, Gillis CL, et al.: Ultrasonographic evaluation of the equine placenta by transrectal and transabdominal approach in the normal pregnant mare. Theriogenology 47:559, 1997.) if the fetus is not in close apposition with the uterine wall. Mares with normal pregnancies should have a minimum CTUP of 7.1 ± 1.6 mm and a maximal CTUP of 11.5 ± 2.4 mm.23 Pregnancies with an increased CTUP have been associated with the delivery of abnormal foals.23 False-positive results have been reported, and clinical judgment should be exercised before treatment is implemented. Placental separation and purulent material at the ventral aspect of the base of the gravid horn and the uterine body can be observed in mares with nocardioform placentitis. This finding can be identified only by using transabdominal ultrasound. The gross lesions of the fetus are not specific. An increased amount of fluid in the thoracic and abdominal cavities and an enlarged liver are frequently observed in aborted fetuses. Placental lesions in cases of ascending placentitis are most severe on the chorionic surface at an area from opposite the cervix (“cervical star”) to the body of the placenta. The affected area is edematous, thickened, and discolored or brown with a mucoid or fibronecrotic exudate on the surface. The placenta is characteristically thickened and leathery in cases of mycotic placentitis, with lesions well demarcated from the rest of the chorionic surface. Microorganisms can be isolated from the placenta and several fetal organs, most consistently from the stomach. Mares with nocardioform placentitis may have premature mammary development but will not have vulvar discharge, owing to the location of the infection. Placental lesions in mares infected with Amycolatopsis spp. and C. equi are located ventrally in the uterine body and at the base of the uterine horns. Affected areas are avillous, thickened, and covered by thick brown or reddish exudate. Differential diagnoses for this clinical presentation include twins and Cellulosimicrobium cellulans 15 placentitis.15 Prevalence of fungal abortions varies greatly with region. The most common route of fungal infection is ascending via the cervix, and fungal infections may be seen with a mixed bacterial infection. Abortions are observed from mid to late gestation. The chorion generally shows marked evidence of placentitis with edema, thick plaques, and a thick, mucoid exudate. In rare cases, amniotic thickening may be noted. The aborted fetus is often small and emaciated owing to chronic placental insufficiency. Culture of the chorion may be diagnostic but takes time. Culture of the fetus is rarely rewarding. Impression smears of the chorion, as well as sometimes the fetal stomach, may reveal hyphae. PROGESTERONE. The equine placenta is part of an endocrine fetal-placental interaction that synthesizes and metabolizes progestagens.24 This endocrine function of the placenta is important for maintenance of pregnancy after the endometrial cups and the secondary corpora lutea disappear at approximately day 120 to 150 of gestation. Fetal-placental progesterone is rapidly metabolized to 5α-pregnanes. Mares with placental pathology may have increased plasma concentrations of progestagens as a result of stress to the fetal placental unit.25,26 Unfortunately, 5α-pregnanes are not readily assayed in a commercial setting, so diagnosis of placental disease using 5α-pregnane concentrations is not possible. There is crossreactivity between 5α-pregnanes and progesterone using some commercial radioimmunoassays for progesterone. Using an experimental model to induce placentitis, it was found that mares that develop a chronic form of placentitis also develop increased plasma progesterone concentrations.26,27 Conversely, mares that developed acute placentitis and abortion soon after infection experienced a rapid drop in plasma progesterone concentrations. It has been suggested that serial measurement of plasma progestin concentrations in mares with placentitis might be a useful method to identify mares that may abort or deliver prematurely.26 However, in a recent prospective study of 700 mares in central Kentucky, with blood collected weekly until the end of pregnancy, progesterone concentrations in the sample obtained during the week preceding abortion were not significantly different from those in mares with normal pregnancy outcome.28 Sensitivity of progesterone assays can be improved when they are combined with evidence of placental thickening as detected using transrectal ultrasonography.27 ESTROGEN. Serum estrogen concentrations are deviated in pregnant mares between 150 and 310 days of gestation.29 The predominant estrogens in pregnant mares are estrone, equilin, equilenin, estradiol-17β, and estradiol-17α. Douglas29 observed that mares aborting from placentitis had serum estrogen concentrations below those normally detected in pregnant mares. These observations were supported by results from a recent prospective study, in which low estradiol-17β sulfate serum concentrations were significantly associated with abnormal pregnancy outcome.28 Based on these findings, it was suggested that supplementation with estradiol cypionate (ECP) or estradiol-17β may prevent abortion in mares with placentitis, but this has not been supported by later research.30 RELAXIN. Relaxin is produced by the equine placenta and can be detected in peripheral blood plasma from day 80 of gestation and then throughout the pregnancy. The role of relaxin during pregnancy is not fully understood, but there is some evidence that placental relaxin production is compromised in mares at risk of aborting their fetuses.31 There currently is no commercial test available for equine relaxin. ADDITIONAL MARKERS FOR PLACENTITIS Acute Phase Proteins. Serum amyloid A (SAA) remains low throughout gestation but shows a significant increase within 12 hours of parturition and returns to baseline within 60 hours postpartum.32 Interestingly, levels of SAA in peripheral blood have also been reported to increase in mares with experimentally induced placentitis.33 However, SAA is a nonspecific marker of inflammation with significant increase observed during other sources of inflammation and even after vaccination. Furthermore, only a weak association was detected between pending abortion and elevated SAA concentrations in a prospective clinical study.28 Serum Alpha-Fetoprotein (AFP). Elevated AFP has been associated with abnormal pregnancy outcome under clinical conditions, and this protein may be used as a marker for mares with placentitis and/or at risk of aborting.28 In summary, no single test appears to have sufficient specificity, sensitivity, or practicality to accurately detect early subclinical cases of placentitis. A panel of estradiol-17β, AFP, and SAA may serve as the best available method to screen mares for unhealthy pregnancies as well as predict the outcome. ■ Treatment and Prognosis Treatment efforts should be directed at combating infection, reducing inflammation, and controlling myometrial activity. Pregnant mares with clinical signs of placentitis should be treated with systemic broadspectrum antimicrobials and antiinflammatories. Commonly used antibiotics such as penicillin G sodium or potassium (22,000 IU/kg IV q6h), gentamicin (6.6 mg/kg IV q24h), and trimethoprim-sulfadiazine (30 mg/kg PO bid) cross the placenta and reach therapeutic concentrations in both placental tissues and the allantoic fluid.34 However, the duration of these elevated concentrations was short and below that in blood plasma. This may explain why more than 60% of mares that had been treated for placentitis still cultured positive on endometrial biopsy after foaling.35 It may also explain why antibiotic treatment appears to be necessary for the remainder of gestation in mares with placentitis. Flunixin meglumine (1.1 mg/kg IV or PO q12h) and pentoxifylline (8.5 mg/kg PO bid) have been used to control proinflammatory cytokines associated with placentitis. Treatment with progestins has long been advocated to promote uterine quiescence in mares with uterine pathology. Presumably the anti-prostaglandin effect of progestins contributes to reduced myometrial activity by interfering with upregulation of prostaglandin and oxytocin receptors.36 Altrenogest at twice the recommended dose (0.088 mg/kg PO q24h) is commonly used. The efficacy of multimodal, long-term therapy for equine placentitis has been investigated in a large-scale clinical trial.37 Investigators examined records of 477 mares over 6 years. Fifteen mares were diagnosed with placentitis. Criteria for treatment included increased thickness of the uteroplacental unit using transrectal ultrasound, placental separation, and/or vulvar discharge and udder development. The average gestational age at diagnosis was 8.6 months. Mares were treated until abortion or delivery of foal with a combination of systemic antibiotics (trimethoprim-sulfa, ceftiofur, or penicillin and gentimicin); pentoxifylline; altrenogest; and nonsteroidal antiinflammatory agents. Twelve of 15 treated mares (80%) carried their foals to term, and 11 of 15 (73%) delivered live foals. Birth weights of surviving foals from mares treated for placentitis were similar to those of foals from nonaffected mares. The benefit of this treatment strategy is supported by more recent data from a controlled study on experimentally induced placentitis.38 Therefore long-term antibiotic, antiinflammatory, and progestin treatment may positively affect pregnancy outcome in mares with placentitis. Although most mares are capable of conceiving and successfully carrying a foal to term in subsequent breedings, reproductive performance may be negatively affected after placentitis, be it induced by the ascending or hematogenous route. Treatments for endometritis, such as uterine lavage and intrauterine infusions of appropriate antibiotics, should be implemented after abortion. Most mares affected by nocardioform placentitis do not require subsequent treatment and show no signs of infertility the following breeding season. Equine Herpesvirus 1 Abortion The most prevalent viral cause of equine pregnancy loss is equine herpesvirus 1 (EHV-1), which causes abortion, paresis, and neonatal foal death. EHV-4 causes abortion in rare cases. The primary route of transmission of EHV-1 is via the respiratory tract. The virus invades the respiratory epithelium and establishes a leukocyte-associated viremia. EHV-1 establishes a chronic, possibly lifelong, latent infection. During the initial infection, placental endothelial cells are infected by the virus and transiently present targets to the immune system as the cells present viral particles. The virus eventually inactivates the major histocompatibility complex 1 (MHC-1) ability of the cells to present viral particles, thus evading the immune system.39 After respiratory infection, EHV-1 causes an episode of viremia and infects the fetus via transplacental migration of virus-bearing leukocytes. Respiratory clinical signs in infected mares may be subclinical. The time between infection and abortion varies greatly from less than 2 weeks to several months.40 Abortion occurs as a result of a rapid separation of the placenta, causing suffocation of the fetus.41 Near-term fetuses may be born alive but will die within days. Aborting mares clear the virus quickly from the reproductive tract, and subsequent fertility is often not affected by the disease. Clinical signs and fetal lesions of abortion caused by EHV-1 and those caused by EHV-4 are indistinguishable from each other.40 As with all herpesviruses, EHV-1 establishes a latent infection that may recrudesce after stressful events, such as weaning, translocation, introduction of a new animal, or other illnesses. It is unclear whether a reactivation event will cause an abortion, but this is considered likely.42 Recrudescent infections are certainly transmissible. Aborted, infected fetal materials are also highly contagious. Both of these sources may be responsible for abortion epizootics. Although epidemic abortions occur, losses may be confined to only a few mares in a herd. ■ Clinical Signs and Diagnosis The primary lesion of EHV-1 is necrotizing vasculitis and thrombosis resulting from lytic infection of the capillary endothelium. The fetus may become infected or remain uninfected, depending on whether the virus crosses the uteroplacental barrier. If transplacental fetal infection occurs late in gestation, a live, infected foal may be born but will not usually survive. Stage of pregnancy during which abortions may occur varies, but the vasculitis is most pronounced from the fifth to ninth months of gestation, and 95% of abortions occur in the last trimester of pregnancy.43 Abortions occur suddenly as sporadic abortions or “abortion storms” without maternal clinical signs. The aborted fetus is fresh, with minimal signs of autolysis. Gross lesions in the fetus include increased fluid in the thoracic and abdominal cavities; congestion and edema of the lungs; hepatomegaly with multifocal, small (~1 mm), yellow-white necrotic foci; subcutaneous edema; and icterus. Histologically, the most characteristic lesion consists of areas of necrosis in lymphoid tissue, liver, adrenal cortex, and the lung, with large intranuclear eosinophilic inclusion bodies. In addition, a hyperplastic necrotizing bronchiolitis is often found. Lymphoid tissues are most commonly affected (nodes, thymus, spleen, and Peyer's patches). Other histopathologic lesions may include mild, multifocal, necrotizing lesions in the liver and adrenal cortex and a hyperplastic, necrotizing bronchiolitis. The placenta may be grossly normal or edematous with no specific microscopic lesions.44 Laboratory diagnosis of EHV-1 abortion is done by either direct demonstration of virus (virus isolation or viral antigen) or viral nucleic acid detection (PCR) or indirectly through serologic evidence of recent infection. The placenta, lung, liver, spleen, and thymus should be collected aseptically in suspected cases of EHV-1 abortion for virus detection. Tissue samples for virus isolation should be kept at 4° C, not frozen at -20° C, until inoculated into cell culture. Samples that cannot be processed within a few hours after collection should be stored at -70° C. The identity of virus isolates recovered from tissue specimens must be confirmed by PCR, indirect immu- nofluorescent assays using EHV-1 specific antisera or monoclonal antibodies, or neutralization assays using EHV-1 specific antisera or monoclonal antibodies. Serologic tests are not considered reliable in EHV-1 diagnosis. It should be kept in mind that serum from mares that aborted may already contain peak levels of antibodies, and no increase in titers will be detectable in subsequently collected sera. Equine fetuses have been found to be capable of producing antibodies to EHV-1 at 200 days of gestation. Maternal serology is of limited diagnostic value because mares may abort several weeks after infection. The rise in serologic titer may have disappeared by the time of the abortion. ■ Treatment and Prognosis Most studies do suggest a beneficial effect of vaccination, and the current recommendation is to vaccinate during the fifth, seventh, and ninth months of gestation.39,43 Both killed and modified live vaccines are available. The vaccines are not fully protective, and abortion may occur in vaccinated mares. However, consistent vaccination of pregnant mares should be expected to decrease the incidence of abortion storms and sporadic abortions in a herd. For the effectiveness of a vaccination program to be maximized, it needs to be combined with a management strategy that minimizes exposure of mares to the virus and prevents activation of a latent viral infection. All horses—young, adult, nonpregnant, and pregnant—should be vaccinated to restrict shedding of the virus. Unnecessary stress such as transportation and overcrowding should be avoided. Pregnant mares should be kept separate from other horses on the farm. Newly arrived horses should be isolated from the resident population for 3 weeks, during which time they should be monitored daily for signs of respiratory disease. After abortion, the fetus and fetal membranes should be transported away from the area without contaminating the surrounding environment. The stall in which the mare aborted should be disinfected with a phenolic or iodinophoric compound, and the bedding should be prevented from contaminating other areas on the farm. All pregnant mares on an infected farm should remain on the farm until they have foaled. No horse should leave the farm until 3 to 4 weeks after the last abortion. Equine Viral Arteritis Equine viral arteritis (EVA) is caused by equine arteritis virus (EAV). The primary target of EAV is the vascular endothelial cells and macrophages. Shortly after infection EAV can be found in the macrophages and later in the lymph nodes. The virus infects circulating monocytes and becomes systemic in distribution by 3 days after the primary infection, resulting in a carrier state (important in stallions). About a week after the primary infection, EAV infects the blood vessel endothelium and causes enough damage by 10 days after the primary infection to cause abortion. Abortion is likely caused by myometritis and vasculitis. Serum progesterone concentrations (produced exclusively by the placenta in the last half of equine pregnancy) fall to baseline levels before the abortion because of placental hypoxia. Although the pathophysiology is not well established, fetal death may occur by fetal anoxia secondary to compression of myometrial vessels by edema and decreased progesterone production by the placenta.45 ■ History and Clinical Signs Clinical signs may be absent or highly variable and may include pyrexia, depression, anorexia, leukopenia, limb edema, stiffness of gait, rhinorrhea and epiphora, conjunctivitis, rhinitis, urticarial rash, localized or diffuse edema, and abortion. Abortion typically occurs at 3 to 10 months of gestation and follows the onset of clinical signs by several days up to 2 months. Abortion rates in outbreaks of EVA have varied from less than 10% to 71%. Less frequently, severe respiratory distress, ataxia, mucosal papular eruptions, submaxillary lymphadenopathy, and intermandibular and shoulder edema may be observed.46 Infection is rarely fatal in adults but is more frequently fatal in neonates due to interstitial pneumonia and secondary bacterial infections. Clinical pathologic findings are variable, inconsistent, and nonspecific and include hypoxia, hypercapnia, respiratory or metabolic acidosis, lymphocytosis or lymphopenia, neutrophilia or neutropenia, thrombocytopenia, and hyperfibrinogenemia. Gross and histologic lesions differ in severity with the virulence of the viral strain. Edema, congestion, and hemorrhage of the subcutaneous and lymphoid tissues and viscera are the most common gross lesions. Histologic lesions may be found in the vasculature, lymphoid tissues, lungs, intestines, adrenal glands, kidneys, and skin.46 Abortion may occur without any clinical signs in the mare, and the fetus may be fresh or autolyzed. Fetal lesions are uncommon. The infected stallions may serve as long-term carriers, and virus may be transmitted in the semen. ■ Laboratory Diagnosis Laboratory diagnosis of EVA is currently based on any combination of virus isolation, viral nucleic acid or antigen detection, and serology. The most appropriate specimens for virus isolation from live horses include nasopharyngeal swabs or washings, conjunctival swabs, and citrated or ethylenediaminetetraacetic acid (EDTA) blood samples for separation of buffy coat cells. Placenta, fetal fluids, lung, spleen, and lymphoid tissues should be collected for virus isolation to confirm cases of EAV-induced abortion. Reverse transcription PCR (RT-PCR)-based assays (standard and real time) have several potential advantages over the current virus isolation procedure. Serologic diagnosis of EVA is based on virus microneutralization and is standardized by the World Organization for Animal Health (still known by the French abbreviation OIE for Office International des Epizooties) and described in the OIE manual. There are no characteristic lesions of EVA infection in the fetus, although autolysis and myocardial arteritis have been reported. An avidin-biotin complex (ABC) for immunoperoxidase staining using monoclonal antibodies to individual EAV proteins has been used successfully to detect viral antigens in formalin-fixed paraffin-embedded samples, as well as in frozen tissue sections. ■ Epidemiology and Control Transmission may occur venereally from persistently infected stallions to mares. Reproductive performance of venereally infected mares is not affected, but contact transmission from venereally infected mares to late gestational mares may cause abortion. Major outbreaks of EVA were reported in 1953, 1984, and 2006 in the United States. Apart from these incidents, occasional outbreaks have occurred, with abortion occurring at low incidence.47 Mares may be isolated after infection but usually do not become carriers. A proportion of naturally infected stallions become persistently infected with EAV and shed the virus constantly in semen. Incidence of seropositive animals is higher in Standardbreds than in Thoroughbreds, and regulatory guidelines may govern the use of seropositive Thoroughbred stallions. Carrier stallions may be the reservoir for the disease between outbreaks and should be isolated and bred only to immune mares. Mares bred in this way should be isolated for 3 weeks. A modified live-virus attenuated vaccine and a killed-virus vaccine are available for prevention of EAV infection in mares and stallions, although some local regulatory restrictions on use may exist. Vaccination of mares up to 3 months before foaling or in the postpartum period appears to be safe. Vaccinating pregnant mares in the final 2 months of gestation is associated with an increased risk of abortion, and decisions to vaccinate in this period must be weighed against concerns for widespread disease in naturally infected herds.48 Control in stallions involves vaccination of seronegative stallions under the guidance of regulatory authorities. Leptospirosis Abortion Leptospirosis causes bacterial abortions in some areas and was reported to be responsible for 2.2% of abortions in a Kentucky study.49 The serovar responsible shows regional variability. Serovar Leptospirapomona has most commonly been associated with leptospirosis abortion in mares, but Leptospira grippotyphosa, Leptospira hardjo, Leptospira bratislava, and Leptospira icterohemor- rhagiae have also been isolated from sporadic abortions.49 Wet environmental conditions are considered important in the dissemination of the disease from wildlife to horses. Infected animals shed the spirochete in their urine, which contaminates groundwater and serves as a source for further infections. Many horses are seropositive for leptospires but are subclinical. ■ Clinical Signs and Diagnosis Clinical signs may include pyrexia, hemoglobinuria, jaundice, and abortion. Aborted chorioallantoic lesions are similar to those of other bacterial placentitis cases (nodular cystic allantoic masses, edema, necrotic areas of chorion, and necrotic mucoid exudate coating the chorion) but may show a diffuse pattern of distribution, indicating a hematogenous source of placental infection. Funisitis has been reported in leptospiral cases of abortion, and examination, both gross and histologic, of the umbilical cord should always be a part of every abortion investigation.50 Serologic antibody conversion lasts for years, so serologic diagnoses are not helpful. Gross lesions are nonspecific. Diagnosis is best done by fluorescent antibody (FA) tests or Warthin-Starry (WS) silver stain of the allantochorion and umbilical cord. Demonstration of leptospirosis could aid in rapid diagnosis and have important clinical and therapeutic indications in the case of live-born, weak foals.50 ■ Treatment and Control Horses may shed spirochetes in urine for up to 90 days; therefore affected animals should be isolated and treated with antibiotics. Aborting mares should be isolated, and the stalls should be disinfected. Infected mares may be treated with streptomycin (10 mg/kg twice daily), penicillin (22,000 to 44,000 IU/kg IM twice daily), or oxytetracycline (5 to 10 IV mg/kg) for a period of 1 week. Because L. pomona is the most common isolate in the United States, mares should be separated from other leptospiral hosts such as ruminants and pigs. A vaccine against L. pomona is available for horses. Vaccines for cattle are not effective in horses. Protozoal Abortion Pregnant mares with equine monocytic ehrlichiosis (Potomac horse fever), caused by the protozoa Neorickettsia risticii, may abort. Abortions caused by N. risticii have been documented in both natural and experimental cases.51,52 Mares were infected at 90 to 180 days of gestation and aborted at around 217 days of gestation. ■ Clinical Signs and Diagnosis Abortions have been observed 2 to 3 months after clinical signs of ehrlichiosis.53 Abortions were associated with placentitis and RFMs. Fetal histologic lesions include enterocolitis, periportal hepatitis, myocarditis, and lymphoid hyperplasia with necrosis of the mesenteric lymph nodes and spleen. Recovery of the protozoan may be from fetal bone marrow, spleen, lymph node, colon, or liver.51,52 The diagnosis can be confirmed by identifying a small number of rickettsiae by PCR assay. ■ Treatment and Prevention Treatment with oxytetracycline (6.6 mg/kg IV once daily) for 5 days in pregnant mares with clinical signs of ehrlichial colitis may prevent or reduce the incidence of abortion. Commercial vaccines against equine ehrlichiosis are available, but the protective effect of vaccines against abortion is unknown. Neospora caninum is a known protozoal abortifacient in cattle. This protozoan has not been definitively shown to cause abortion in the mare, but its presence has been documented in aborted foals, suggesting the need for further investigation.54 Insect-Related Abortion In the equine breeding season of 2001, central Kentucky horses experienced pregnancy losses estimated to have affected more than 3000 mares (>60% of mares on some farms55) and to have resulted in more than $330 million in losses.56 The syndrome was named mare reproductive loss syndrome (MRLS). On a much smaller scale, MRLS was documented in mare abortions in north central Florida during the 2006 breeding season. Epidemiologic studies noted abnormal weather patterns (sudden freezing in mid-April followed by unusually warm springtime temperatures) and positive correlations with the presence of black cherry trees (Prunus serotina) and abnormally large numbers of the eastern tent caterpillar (Malacosoma america- num).i5 Pregnancy loss was later linked to ingestion of the caterpillars themselves, with the toxic agent related to the larval exoskeleton. ■ Clinical Signs and Diagnosis Clinical signs preceding early embryonic death or abortion are typically not observed. Both early (40 to 150 days' gestation) and late (near-term) pregnancies are affected. Hyperechoic amniotic and allantoic fluids can be noted on ultrasonographic examination, along with a dead or dying fetus (slow heart rate, bgcolor=white>Pathology, virus isolation, fetal serology | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| BVD virus, pestivirus | Any stage | Anomalies of skeletal, nervous, cardiovascular, respiratory, or other systems | Pathology, FA test on fetal tissues, fetal serology (virus neutralization, ELISA), serologic survey in herd | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| EBA, foothill abortion, deltaproteobacterium | Third trimester | Lymphadenopathy, splenomegaly, hepatopathy | Pathology, PCR | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Brucella abortus, brucellosis, | Third trimester | Placentitis, fibrinous serositis, | Culture, maternal serology (card | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bang’s disease | bronchopneumonia | test, plate, or tube agglutination) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Campylobacter fetus subsp. | Usually early | Placentitis, fibrinous serositis, | Pathology, dark-field examination, | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| venerealis, | embryonic | bronchopneumonia, hepatitis | culture (Clark media), smegma | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| campylobacteriosis, vibriosis | death | (Clark media) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Histophilus somni (formerly | Any stage | Placentitis | Histopathology, culture | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Haemophilus somnus) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Leptospira interrogans, | Fifth to ninth | Icterus, edema, renal | Fetal and maternal serology, FA in | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| leptospirosis | months | degeneration and inflammation | urine | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Leptospira interrogans, listeriosis | Eighth or ninth month | Placentitis | Histopathology, culture | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Salmonella Dublin, Salmonella | Third trimester | Placentitis | Culture | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Typhimurium | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Aspergillus fumigatus and all fungal species, mycotic | Third trimester | Placentitis, bronchopneumonia, dermatitis | Histopathology, fungal culture | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| abortion | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Sarcocystis cruzi | Third trimester | Protozoa in caruncles | Histopathology or FA of caruncles | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Tritrichomonas foetus, trichomoniasis | First half | Placentitis, bronchopneumonia | Microscopic demonstration of organism, culture (Diamond media), PCR | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bovine neosporosis | Mid-gestation | Similar to those found in toxoplasma-aborted sheep fetuses | Histopathology, seroepidemiology | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
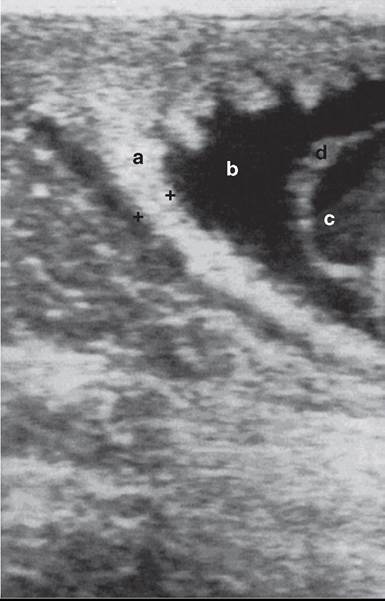
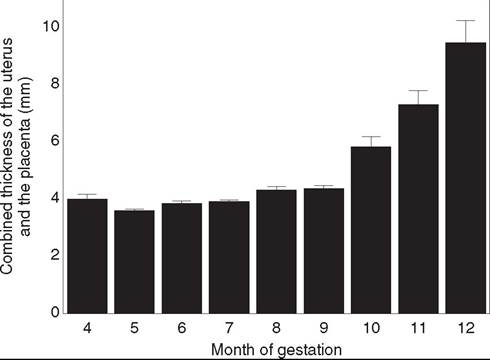
BVD, Bovine virus diarrhea; EBA, epizootic bovine abortion; ELISA, enzyme-linked immunosorbent assay; FA, fluorescent antibody; IBR, infectious bovine rhinotracheitis; PCR, polymerase chain reaction.
■ TABLE 43.9
Major Causes of Abortion in Sheep and Goats
| Cause and Common Names | Usual Stage of Gestation | Major Fetal Lesions | Diagnostic Tests |
| Bluetongue, orbivirus | Any stage | Anomalies of skeletal or nervous systems | Pathology, IFA, serology |
| Border disease, pestivirus, | Any stage | Dysplasia of skeleton, CNS, | Pathology, virus isolation, serology |
| hairy shaker disease | and fleece | (cross-reacts with BVD) | |
| Coxiella burnetii, Q fever | Near term | Necrotizing placentitis | Histopathology, microscopic demonstration of rickettsiae, complement fixation, ELISA |
| Chlamydia psittaci, EAE | Fourth or fifth month | Necrotizing placentitis | Histopathology, microscopic demonstration of organism, fluorescent antibody on fetal tissues or cultures, paired sera |
| Campylobacter fetus subsp. | Last 6 weeks | Placentitis, serositis, | Pathology, microscopic demonstration of |
| fetus, vibriosis | multifocal hepatic necrosis | organism, culture | |
| Toxoplasma gondii, | Any stage | Necrosis and calcification in | Pathology, demonstration of organism, |
| toxoplasmosis | cotyledons | serology (e.g., agglutination, ELISA) |
BVD, Bovine virus diarrhea; CNS, central nervous system; EAE, enzootic abortion of ewes; ELISA, enzyme-linked immunosorbent assay; IFA, immunofluorescent antibody.
immunohistochemistry, or serum neutralization testing. If the latter is to be used, at least two samples must be taken days apart. The first must be negative and the second positive, or the first must be positive and the second titer must show a fourfold increase. Serum testing may not be helpful because the dam may have been infected months before the abortion and the titer after the abortion may actually be falling.
Prevention of disease is by vaccination (though infection and latency may occur despite vaccination). It is recommended to vaccinate heifers at 6 months and administer a booster 3 to 4 weeks before breeding. Vaccination too close to breeding can result in lowered conception rates due to normal, transient inflammation of the reproductive tract. A modified live virus is commonly used in pregnant cows from the third to eighth months of gestation, but its safety is questionable. A killed viral vaccine is available for pregnant cow use; a modified live virus vaccine labeled for intranasal administration is also available.1
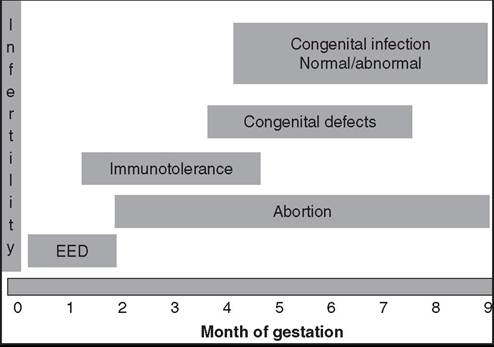
FIG. 43.8 Potential clinical reproductive outcomes after infection with bovine viral diarrhea virus. EED, Early embryonic death. (From Smith KC, Blunden AS, Whitwell KE, et al.: A survey of equine abortion, stillbirth and neonatal death tn the UKfrom 1988 to 1997. Equine Vet J 35:496, 2003.)
Bovine Viral Diarrhea Virus
Bovine viral diarrhea virus (BVDV) is a pestivirus that can produce early embryonic death, fetal anomalies, or abortion (see Chapter 32 for complete discussion).1
■ History and Clinical Signs Although fetal death is most common during the first trimester, abortion can occur at any stage of gestation.2,3 Pathogenicity of the disease depends on gestational time of infection, the viral strain, viral biotype (cytopathic or noncytopathic), and fetal immunocompetence.4 Often there is a history of repeat breeding and a recent episode of febrile disease in the herd before the onset of abortions.
■ Laboratory Diagnosis Fetal loss generally occurs 10 to 27 days after exposure, with expulsion of the fetus up to 50 days later.4 As a result the fetus is most often autolyzed, although in some cases it may be mummified or fresh. The aborted fetus may have a variety of dysplastic lesions, including cerebellar hypoplasia; cerebral malformations (hydrencephaly, porencephaly, microencephaly); cataracts; brachygnathia; arthrogryposis; alopecia; thymic hypoplasia; and intrauterine growth restriction.2,5 Microscopic lesions include a mild nonsuppurative placentitis. Nonsuppurative vasculitis may be observed in the placenta, liver, or lymph nodes.
Virus isolation from fetal tissue is seldom successful, likely because of the protracted time before fetal expulsion generally occurs after infection. Viral antigen may be detected by FA test on kidney, lung, or lymph node. Virus neutralization and enzyme-linked immunosorbent assay are used to detect antibodies in fetal thoracic fluid, which indicate prenatal exposure to the virus but do not necessarily incriminate BVDV as the cause of abortion. Maternal titers are seldom of diagnostic value because a rise in titer generally occurs before abortion.
■ Pathophysiology BVDV may be shed in most body secretions. The effects of exposure to BVDV vary greatly depending on the gestational time during which exposure occurred (Fig. 43.8).6 In seronegative cows, exposure to BVDV at the time of breeding prevents conception. Placental attachment at approximately 35 days' gestation seemingly must precede fetal infection. During the first 4 months of gestation, infection usually causes fetal death and abortion. Fetuses that survive infection with noncytopathic strains between 18 and 125 days of gestation will be persistently infected (PI), are typically seronegative at birth, and subsequently shed BVDV continuously.4 They may develop mucosal disease later in life from superinfection with cytopathic BVDV.7,8 Fetuses infected at between 100 and 150 days of gestation, considered congenitally infected (CI), are at risk for the development of dysplastic lesions, including teratologic defects in the brain, skin, or bronchioles. Fetuses infected after 150 days usually recover without dysplastic lesions.2 Recent evidence, however, suggests that those fetuses born with neutralizing titers to BVDV are more likely to develop a serious illness within the first 10 months of life and less likely to conceive as heifers than those calves born without neutralizing titers to BVDV.9,10
■ Epidemiology Most cattle have serum antibodies to the virus. The abortion rate may approach 25% with new infection of a susceptible herd.
■ Control Killed and modified-live vaccines are available and are an important component of BVDV control, but BVDV is not fully controlled with vaccination. Herd health plans must focus on elimination of PI animals and prevention of new PI animals being introduced into the herd.
Leptospirosis
Leptospirosis is a spectrum of diseases caused by multiple serovars of Leptospira interrogans. Leptospira hardjo is the major serovar associated with bovine leptospiral abortion, although isolations of serovars pomona, canicola, icterohemorrhagiae, grippotyphosa, and szwajizak have also been reported.11 Two serologically indistinguishable but genetically distinct types of serovar hardjo have been identified: L. interrogans serovar hardjo (type hardjo-prajitno) and Leptospira borgpetersenii serovar hardjo (type hardjo-bovis). Serovar hardjo type hardjo-bovis is cosmopolitan in cattle populations, whereas type hardjo-prajitno is isolated primarily from cattle in the United Kingdom.
■ History and Clinical Signs In cattle, infection with serovar hardjo is associated with infertility, early embryonic death, abortions from 4 months of gestation to term, and birth of weak calves. Abortion rate is usually less than 10% but may approach 50% in some areas.12 L. interrogans serovar pomona abortion usually occurs in the last 3 months of gestation, with an abortion rate as high as 50%. Clinical signs of leptospirosis in the cow may include icterus, hemoglobinuria, anemia, fever, and mastitis that is characterized by a flaccid udder and thick ropy secretions from all four quarters, but usually cows abort without clinical illness. Dead or weak calves may be delivered at term.12 Abortions caused by serovar hardjo tend to occur sporadically rather than in storms (as may be seen with serovars pomona and grippotyphosa).
■ Laboratory Diagnosis The aborted fetus is usually autolyzed, icteric, and edematous. Histologically, renal tubular necrosis is accompanied by lymphocytic interstitial nephritis, pneumonia, and placentitis.
Leptospires are rapidly destroyed by autolysis or freezing. Isolation from fetal liver, kidney, or brain is possible but slow and impractical. Leptospires may be isolated or demonstrated by dark-field microscopy, FA staining, or histologic techniques in fetal or placental tissues or in the urine of the aborting dam within approximately 2 weeks after abortion.
Diagnosis is usually based on serology. A few infected fetuses develop microagglutination titers of 1:10 or more. It is difficult to distinguish among vaccinated, acutely infected, and recovered animals, but titers to serovarpomona greater than 1:12,800 in the dam suggest leptospiral abortion. Maternal titer has usually peaked by the time of abortion. Single titers of 1:800 or more in unvaccinated animals, seroconversion, or fourfold changes in titers in paired sera indicate leptospirosis in the herd. Titers to serovar hardjo are often less than 1:100 in affected cows and seldom exceed 1:1600.
■ Pathophysiology Hematogenously spread leptospires colonize the gravid uterus up to 142 days after infection. Abortion occurs 1 to 6 weeks after acute disease with L. pomona infection and 1 to 3 months with L. hardjo. L. hardjo remains in the oviducts of infected cows for up to 22 days after calving.12
■ Epidemiology Leptospira organisms are ubiquitous and an important cause of abortion in all cattle-producing regions. Leptospira organisms persist in the genital tract and kidneys. The organisms localized in the kidneys of infected animals are shed in the urine and serve as a source of infection for other animals. The organisms localized in the female reproductive tract are responsible for abortions. Aborted tissues are infectious to other animals and humans and should be handled with caution.13,14
■ Treatment and Control In abortion outbreaks, pregnant cows can be vaccinated with killed bacterin and treated with oxytetracycline (antibiotic treatment can be limited to sick cows in dairy herds).15 Aborting cows should be isolated from the rest of the herd, and aborted fetuses and placentas should be removed from the premises.16 Preventing exposure to swine, rodents, and contaminated water lessens the opportunities for infection. L. interrogans serovarpomona usually has no permanent effect on fertility, but infection with serovar hardjo has been associated with persistent herd infection and recurring abortions.
Herd vaccination is recommended at 6-month intervals or more frequently in areas with heavy exposure to leptospires, such as dairies or beef operations with wet environments. Vaccination programs are aimed at reducing urinary shedding of leptospires and decreasing fetal loss. Vaccination is discussed in detail in the Leptospirosis section in Chapter 34.
Epizootic Bovine Abortion (Foothill Abortion)
Epizootic bovine abortion (EBA), or foothill abortion, is a syndrome of late abortions in cattle in the foothills bordering the central valley of California.17 Once thought to be caused by Chlamydia psittaci or a spirochete-like organism, studies have demonstrated that EBA differs from chlamydial abortion.17 After decades of research, a novel deltaproteobacterium, Pajarellobacter abortibovis, was identified as the causative agent of EBA in 2005.18,19
■ History and Clinical Signs Late abortion or delivery of weak calves occurs in affected herds. Many fetuses in the sixth to seventh month of gestation may be aborted, especially from naive heifers that have not had natural exposure to the causative agent. Older native cows show no clinical signs of infection.
■ Laboratory Diagnosis A 3-month period is required for full development of pathologic changes in the fetus. Superficial cervical lymph nodes are enlarged up to 16 g, the spleen is enlarged up to 250 g, the thymus is slightly smaller than normal, and the liver may be enlarged and nodular.17,20 Histologically there is loss of thymic cortical lymphocytes; remaining lymphocytes are enlarged and poorly differentiated. Follicular hyperplasia, histiocytosis, vasculitis, necrosis, and pyogranulomas occur in lymph nodes and spleen. Lympho- histiocytic proliferation may also occur around vessels in the liver, lung, and meninges.
EBA has been diagnosed mainly by pathologic examination of the fetus along with a compatible clinical scenario. Studies have demonstrated high levels of immunoglobulin G (IgG; 3 mg/mL or more) in fetal blood.17 This deltaproteobacterium is detectable in fetal tissues with PCR, with reported sensitivity and specificity values of 88% and 100%, respectively.18 Recent advances in real-time PCR assays are promising for diagnosis and may become the standard in the future.21 Currently, serologic testing for EBA has promising results for identifying fetal infection, especially with fetal serum or precolostral serum in live calves. It may be difficult to distinguish immunity and recent exposure in adult cows and heifers.
■ Pathophysiology Infection is transmitted by the soft- shell tick Ornithodoros coriaceus (pajaroello tick).20,22 The disease can also be transmitted with fresh or frozen fetal tissue.17 Transformation and proliferation of fetal lymphocytes and macrophages occur by 50 days but are not severe enough for diagnosis until 100 days after maternal exposure to the tick vector. IgG and IgM are deposited in vascular lesions, but an increase in fetal serum immunoglobulin is not detectable until at least 80 days after tick exposure.17,21 Repeated superinfection may be necessary to result in fetal death.20 Because at least 90 days are required for development of fetal lesions, infection after 6 months' gestation is not likely to result in abortion.
■ Epidemiology EBA was limited to the range of the tick vector in the foothills bordering the central valley of California; however, it has also been identified in regions of Oregon and Nevada.17,19 Of the annual calf loss in California, 5% to 10% is attributed to EBA.22 The prevalence of infection by the spirochete is far greater than the prevalence of abortion.20 Abortion occurs 3 to 4 months after exposure to ticks but almost always late in gestation, regardless of the time of tick exposure.23 Older native cows from enzootic areas usually do not abort, and introduced cows and heifers generally abort only once.17 The abortion rate may be 30% to 80% in sus-
23
ceptible animals.23
■ Treatment and Control Currently no commercially available vaccine exists for EBA, but abortions can be controlled by exposing heifers to the tick vector before breeding or by changing from spring to fall calving, which takes advantage of limiting exposure to the last trimester of gestation in some management systems. Therefore exposure of susceptible pregnant cattle to the tick only after the sixth month of pregnancy is a practical solution for ranchers using summer foothill pastures and fall calving. The tick lives in ground duff (e.g., leaves) and is not found on cattle that graze in irrigated pastures and most other areas outside of brushy foothills. Although chlortetracycline in feed has been used previously to reduce the rate of abortion,22 such off-label use of antimicrobials in feed for cattle is no longer legal in the United States.
Brucella abortus Abortion
Brucella abortus is a gram-negative coccobacillus that is a facultative intracellular pathogen. Infection (Bang's disease) causes abortion in cattle and, less commonly, in sheep and goats.24 Horses may be infected with B. abortus, which has been associated with fistulous withers, but usually experience no infertility or abortion. Bang's disease is an important zoonotic disease worldwide, particularly in developing nations.24
■ History and Clinical Signs Abortion is the chief clinical sign of bovine brucellosis and usually occurs in the last trimester of gestation. Because of its highly contagious nature, outbreaks of abortion can occur in grouped pregnant cattle. Lameness, mastitis, epididymitis, and/or orchitis may be present in infected herds.24 A foul-smelling, yellow to brownish exudate containing fibrin and necrotic debris may be expressed from the uterine lumen. Placentitis is a consistent finding. Cotyledons are necrotic; the intercotyledonary placenta is thickened and opaque with accumulation of odorless, flocculent, yellow-brown exudate between maternal and fetal membranes. Importantly, the affected placenta may show some normal placentomes and others with severe necrosis and hemorrhage.24
■ Laboratory Diagnosis Histologically there is suppurative placentitis (and endometritis in the dam). Suppurative bronchopneumonia, serositis, and lymphoreticular hyperplasia are frequent histologic findings in the fetus.
Diagnosis depends on culture of B. abortus from fetal lung, abomasum, or placenta or from maternal uterine or mammary secretions. Organisms and Brucella antigen can be detected in fetal tissues or placenta by immunofluorescent techniques. PCR and culture can be applied as well. Fetal abomasal fluid may be the optimal sample for PCR diagnosis.25,26 A variety of serologic tests can be used to diagnose the disease in clinically or latently infected adults, including serum agglutination, card and buffered plate agglutination, complement fixation, and direct and indirect enzyme-linked immunosorbent assay (ELISA); the performance of these tests in infected and vaccinated herds has been reviewed recently.26
■ Pathophysiology Initial replication of B. abortus occurs in regional lymph nodes. Bacteremia is followed by colonization of supramammary lymph nodes, the mammary gland, and the gravid uterus. Uterine infection occurs during the second trimester.27 In the placenta the bacteria appear first in phagosomes of erythrophagocytic trophoblasts. Replication occurs in the rough endoplasmic reticulum of chorioallantoic trophoblasts.27 Preferential replication in chorioallantoic trophoblasts has been attributed to their erythritol content.24,28 The organism also occurs in fetal placental endothelial cells and capillary lumina, where it is associated with vasculitis and destruction of chorionic villi. Placental inflammation spreads along the allantochorion to involve additional cotyledons with resultant chorioallantoic ulceration, necrosis of trophoblasts, and ulcerative endometritis. Fetal death results from placental disruption and endotoxemia.27 The fetus is frequently retained 1 to 3 days in utero. Numerous bacteria are expelled from the genital tract at parturition, but shedding usually stops by 3 weeks after abortion.
■ Epidemiology Infection with B. abortus occurs naturally by inhalation or ingestion of bacteria present in aborted fetal membranes, fetuses, or postabortion vaginal discharge.24 Contaminated materials are infectious for humans and should be handled with caution. Infection is not easily transmitted between cattle separated by fences or roads. Most calves infected at birth clear the infection, but persistent congenital infection has been documented.29-31
Bovine brucellosis has been nearly eradicated in the United States by test and slaughter of seropositive cattle and vaccination. However, a reservoir remains in bison and elk, especially in the greater Yellowstone area.
■ Treatment and Control Treatment of brucellosis is usually not effective. Combination therapy with long-acting oxytetracycline and streptomycin has been shown to reduce shedding in most cows and potentially eliminate infection in some,32 but because eradication is typically a priority in most countries, infected cows are rarely treated. In the United States, infected individuals are destroyed, and exposed herdmates are quarantined to the herd until slaughter or the herd is recertified as brucellosis free.
In the past, strain 19 vaccine was used as part of the eradication program. However, vaccinated and field strain-infected cattle could not be differentiated. A newer vaccine for B. abortus, vaccine strain RB51, was developed to overcome the serologic problems associated with the strain 19 vaccine.33 Animals vaccinated with RB51 lack antibodies to the O-polysaccharide chain and can thus be differentiated from field-infected cattle. Strain RB51 is also less abortifacient for cattle than strain 19, although vaccination of pregnant heifers may result in abortion and subsequent zoonotic exposure if obstetric assistance is necessary,34 so the vaccine is to be administered only to young heifers before pregnancy.
Campylobacter fetus subspecies venerealis Abortion
C. fetus subsp. venerealis is a gram-negative flagellated bacterium that is the main cause of bovine campylobacteriosis (vibriosis, bovine genital campylobacteriosis).35 The organism is an obligate parasite of the bovine genital tract and is not known to cause disease in other species.35
■ History and Clinical Signs Infection with C. fetus subsp. venerealis mainly causes temporary infertility or early embryonic death, but sporadic abortions from the fourth to eighth months of gestation are possible.1 The usual history includes a high percentage of cows exposed for the first time returning to estrus or found nonpregnant after the breeding season and cows calving late because they returned to estrus one or more times.
■ Laboratory Diagnosis Autolysis is usually minimal, and the lungs of the term fetus may be partially inflated. Dehydration, fibrinous serositis, and necrotizing placentitis may be apparent grossly. Histologically, bronchopneumonia and hepatitis may also be evident. Diagnosis is based on demonstration or isolation of the organism. Using dark-field microscopy, the bacterium appears as a curved rod with darting corkscrew motility and can be differentiated from other Campylobacter spp. by immunohistochemistry.1 Cows that abort may have serum antibody titers; however, they may not be diagnostic because they are not specific for C. fetus subsp. venerealis. Culture from placenta or fetal abomasal contents requires at least 72 hours. The vaginal mucus agglutination test is used to survey herds for infection. Alternatively, the penis and preputial mucosa of infected bulls may be swabbed and cultured, although culture is difficult because the organism is slow growing and often overwhelmed by saprophytes.
■ Pathophysiology The bull is the primary reservoir of the organism; it resides subclinically in the crypts of the penis and prepuce.35 Transmission is venereal. Within a week of vaginal infection the organism is established in the uterus, causing mucopurulent endometritis, which persists 3 to 4 months. Intrauterine infection either prevents conception or causes embryonic death, and infected heifers typically return to estrus by 40 days. Less commonly, abortions occur at up to 8 months of gestation.
■ Epidemiology C. fetus subsp. venerealis is ubiquitous. Venereal transmission from infected bulls to virgin heifers approaches 100%. Cows with previous exposure to infected bulls develop immunity and therefore are less likely to experience infertility than heifers. The abortion rate can range from 10% to 50%.35 Because persistent vaginal infection can occur, vaginal carriage into the next breeding season is possible.35
■ Treatment and Control Infected cows usually recover spontaneously within 5 months and resist reinfection. Recovery is hastened by intrauterine infusions of streptomycin and penicillin. Infertility may be permanent if endometritis or salpingitis is severe. Heifers should be vaccinated with a bacterin before breeding. Most vaccines are administered 1 month before breeding and require a booster vaccination 2 weeks later. Cows and bulls must be vaccinated annually. Exclusive use of C. fetus subsp. venerealis-negative semen via AI controls the disease by preventing transmission.
Histophilus somni Abortion
Histophilus somni (formerly Haemophilus somnus) has been associated with vulvitis, vaginitis, endometritis, weak calf syndrome, stillbirths, and occasional abortion in cattle.36-41
■ Laboratory Diagnosis Aborted fetuses have been free of gross lesions. Necrotizing placentitis is associated with fibrinoid necrosis of placental arteries. Diagnosis is based on recovery of large numbers of the organisms in relatively pure culture from placenta or fetus, histologic evidence of placentitis, and lack of other apparent causes.
Interpretation of maternal titers to H. somni is difficult, and it is best to take paired serum samples. Titers between 1:256 and 1:512 in nonvaccinated herds may be the result of early active or chronic infection. Titers between 1:1040 and 1:4096 indicate recent active infection. A fourfold change in titer in paired sera is the best indicator of active infection.
■ Pathophysiology Although H. somni can be isolated from the genital tract of clinically normal cows, the rate of isolation is higher in cows with endometritis or cervicitis.41 Experimentally, H. somni can adhere to zona pellucida-intact embryos and cause degeneration.38 Vaginitis can be induced by inoculation with H. somni,39 and abortion has been induced by intraamniotic, intravenous, or intrabronchial challenge with the organism.40
■ Treatment and Control Antibiotic treatment and vaccination anecdotally increase fertility in herds affected with H. somni-induced vulvovaginitis.
Listeria monocytogenes Abortion
Listeriosis is caused by Listeria monocytogenes, a ubiquitous, gram-positive, facultative intracellular bacterium.42 Encephalitis, abortions, uveitis, and septicemia are other manifestations of infection in ruminants.
■ History and Clinical Signs Bovine abortions usually occur in the last 2 months of gestation. Infected ewes and does typically abort in the last month. Fever, depression, RFMs, or endometritis may occur, but often the dam shows no clinical signs of infection.
■ Laboratory Diagnosis In less severely autolyzed fetuses, fibrinous polyserositis may be apparent. Most aborted fetuses have gray-white hepatic foci up to 2 mm in diameter. Similar foci may be visible in cotyledons; exudation occurs between cotyledons. Abomasal erosions have been reported in aborted lambs. Histologically, suppurative placentitis and endometritis are consistent findings.
Listeria is readily cultured from abortuses without cold enrichment. Listeria appears in impression smears as grampositive pleomorphic coccobacilli.
■ Pathophysiology Listerial abortion can be induced experimentally in cattle 6 to 8 days after infection and in sheep 3 to 11 days after infection. Fetuses die from placentitis and septicemia and are often retained in utero several days before expulsion.
■ Epidemiology Listerial abortion is usually sporadic, and incidence seldom exceeds 15%. Many outbreaks of abortion and encephalitis have been associated with feeding of silage.42 The elevated pH of spoiled silage enhances multiplication of the organism.42 However, nonensiled forages can be contaminated by L. monocytogenes originating in soil, wildlife or bird feces, or livestock manure, so exposure to silage should not be considered a necessary cause of this disease.42 Aborted tissues are infectious for humans and should be handled with care.
■ Treatment and Control The effect on fertility is usually transient, and aborting animals tend to resist reinfection. Tetracycline may be used in remaining pregnant animals in the herd. Aborting animals should be segregated, and fetuses and placentas should be removed from the premises with strict hygienic protocols to limit human risk. Treatment and prevention of listeriosis is covered in detail in Chapter 8.
Mycoplasma Abortion
Mycoplasmal isolations from the bovine genital tract have been mainly M. bovigenitalium and Mycoplasma bovis. M. bovis is probably the more important cause of abortion.43 Mycoplasma mycoides subsp. mycoides (see Chapter 31 for complete discussion) and Mycoplasma capricolum subsp. capricolum have been associated with caprine abortions.44
■ History and Clinical Signs M. bovigenitalium is associated with granular vulvovaginitis and less commonly with endometritis, especially in heifers. Infertility is more common than abortion. M. bovis causes mastitis and abortion.43 In goats, mycoplasmal infection is associated with septicemia, arthritis, pneumonia, mastitis, and abortion.44,45
■ Laboratory Diagnosis Placentitis and fetal pneumonia have been associated with bovine mycoplasmal abortion.43,45 Isolation of Mycoplasma from the genital tract, milk, placenta, or fetus indicates infection. However, mycoplasmosis should not be considered the cause of abortion unless placentitis or fetal inflammation is present and other more likely causes of abortion have been eliminated.
■ Pathophysiology M. bovigenitalium can be isolated from the vagina in up to 12% of clinically normal cows, but M. bovis is isolated from less than 1%. Vulvitis can be induced by inoculation with mucosal scarification with M. bovigenitalium; therefore venereal transmission may be the natural route of infection.43 Experimental inoculation with M. bovis induces abortion with placentitis and fetal pneumonia.43,45 M. bovigenitalium is rarely isolated from abortuses or normal fetuses.
■ Epidemiology Mycoplasma spp. are ubiquitous, but mycoplasmal abortions are not commonly documented.
■ Treatment and Control Tetracycline, florfenicol, or macrolide antibiotics may limit losses in pregnant animals when Mycoplasma is implicated as the cause of abortion or granular vulvitis in herdmates.
Salmonella Abortion
A variety of Salmonella serotypes have been isolated from aborted fetuses of cattle, sheep, goats, and horses. A complete discussion of salmonellosis is presented in Chapter 32. Infection is acquired by ingestion or inhalation. Maternal septicemia is followed by localization of salmonellae in tissues, including the pregnant uterus, where placentitis and fetal septicemia occur. Salmonellosis accompanied by endotoxemia causes early pregnancy loss without colonization of the uterus because the infection and endotoxemia cause endogenous prostaglandin release.
■ History and Clinical Signs The animal may show systemic signs before abortion. Although abortion may occur at any stage of gestation, it typically occurs in the second half and is characterized by placental necrosis, edema, and hemorrhage. RFMs and fetal autolysis may occur. Abortion may be accompanied by diarrhea, fever, or vaginal discharge, particularly in the ewe, but often infection is not clinically apparent in the dam.46,47 Fetuses also may be lost as a result of stillbirth or perinatal septicemia.
■ Laboratory Diagnosis The fetus is frequently autolyzed. Placentitis is usually present. Diagnosis is based on isolation of the organism and evidence of placentitis or inflammation of fetal tissues. Immunofluorescent techniques can identify the bacteria in impression smears or sections of placenta or fetal tissue. The dam can be tested serologically for evidence of recent active infection.
■ Pathophysiology Infected adult animals are often short-term carriers and shed salmonellae in the feces or milk. True long-term asymptomatic carriers occur mainly with the host-adapted serotypes: Salmonella dublin in cattle, Salmonella abortus ovis in sheep, and S. abortivoequina (or Salmonella abortus equi) in horses. Salmonellosis caused by S. abortus equi has been eradicated in the United States. Occasionally long-term carriers of other serotypes are seen; these are usually intestinal carriers and fecal shedders. Infection usually occurs by ingestion; there is no evidence of venereal transmission.46 Maternal septicemia is followed by localization of the organism in a variety of tissues, including the pregnant uterus. The bacteria multiply in and cause necrosis of connective tissues of the cotyledon. The incubation period between infection and abortion varies from approximately 1 week to 1 month. Fetal death results from placentitis and fetal septicemia.48 In most cases, maternal shedding of the organism in cattle ceases by 5 weeks after calving,46 although longer-term shedding may occur with certain serotypes.
If infection and the resulting endotoxemia induce release of endogenous PGF2α, luteolysis and abortion will occur, but the fetus and placenta will not culture positive for Salmonella spp.
■ Epidemiology Bovine abortion resulting from salmonellosis is caused mainly by Salmonella dublin and Salmonella typhimurium. Abortion is sporadic and most common in the summer and fall.46
Ovine abortion is associated with S. typhimurium, S. dublin, Salmonella arizona, and S. abortus ovis. S. abortus ovis is enzootic in parts of England and Europe but is not reported in the United States. Young ewes in late gestation are most susceptible, and the abortion rate may approach 50%.47
■ Treatment and Control Aborting animals should be isolated; the fetus, placenta, and contaminated material should be removed from the premises. Salmonella spp. are infectious for humans; therefore aborted tissues should be handled with caution. Metritis is a rare complication of salmonellosis that can be fatal. Usually there is no lasting effect on fertility, but animals infected with host-adapted serotypes may become carriers and should be cultured and tested serologically and culled if positive. Salmonellosis can be controlled by hygiene and by avoiding the introduction of carrier animals.
Ureaplasma Abortion
Ureaplasma is a small, ureolytic bacterium that lacks a cell wall. U. diversum has been associated with granular vulvitis and abortion in cattle.
■ History and Clinical Signs Granular vulvitis appears as reddish nodules in the vulvar mucosa, with mucopurulent discharge in the early stages. The discharge is usually more copious and protracted than with IPV induced by herpesvirus.43 Affected cows are not systemically ill. The organism has been recovered from embryo flushing media and can adhere to the zona pellucida, resisting removal by washing. It may reduce the pregnancy rate in embryo recipients when the transfer medium contains the organism.
■ Laboratory Diagnosis Gross lesions include thickening of placental membranes with foci of hemorrhage and fibrinous exudate. Gross lesions are seldom apparent in the fetus. Microscopically the placenta is fibrotic, with heavy mononuclear cell infiltration, multifocal necrosis, fibrin deposition, and mineralization. Cuffs of lymphocytes surround fetal intrapul- monary airways. Diagnosis is based on isolation of the organism from genital mucosa, placenta, or fetal stomach or lung and the presence of genital or fetal inflammation.
■ Pathophysiology Ureaplasma can be isolated from the genital tract of normal cows and from normal fetuses.49 Vulvitis has been induced by inoculation of virgin heifers with U. diversum.49 Intraamniotic inoculation of U. diversum caused placentitis, abortion, and fetal alveolitis in two of four experimental cows.49 One cow delivered a weak calf at term. Experimental infection in ewes did not decrease fertility.50
■ Epidemiology Bovine infection is common, but documented abortions caused by Ureaplasma are rare.43 Infertility is more common in heifers than in cows.
■ Treatment and Control Nonirritating tetracyclines by intrauterine infusion are recommended for treatment. Uterine contamination can be avoided by use of the double-rod technique of AI.
Miscellaneous Bacterial Abortions
In addition to the aforementioned bacteria, other bacteria occasionally produce maternal septicemia and hematogenous abortion, as well as potential ascending infection of the gravid uterus. Many of these bacteria are ubiquitous, frequently contaminate aborted fetuses and placentas, and should not be considered the cause of abortion unless (1) they are isolated from the placenta and fetus in large numbers and relatively pure culture, (2) placentitis or fetal inflammation is evident, and (3) other more likely causes of abortion have been eliminated.
Tritrichomonas foetus
Trichomoniasis is a venereal infection of cattle caused by the flagellated protozoan T. foetus, which subclinically inhabits the prepuce, penis, and occasionally the urethral orifice of infected bulls; transmission to cows results in clinical disease.51-53
■ History and Clinical Signs Infertility characterized by a high percentage of cows returning to estrus or found nonpregnant after the breeding season and cows calving late plus occasional pyometras and abortions are the most common clinical signs of trichomoniasis. Pyometra in postcoital heifers or cows suggests that trichomoniasis may be the cause and should be ruled out first. Abortions generally occur in the first half of gestation at a rate of 5% to 30%.51 The placenta may be expelled or retained.
■ Laboratory Diagnosis Diagnosis in the female is made by culturing trichomonads or using PCR to detect Tritrichomonas from cervicovaginal mucus, uterine exudate, placental fluids, or fetal abomasal contents.53 Preputial smegma collected from bulls by using a plastic pipette or commercially available sampling device run against the mucosa can also be cultured for trichomonads (sensitivity is 84% to 96% under experimental conditions53). Diamond's medium (or modified Pastridge medium) is recommended for cultures from cows, bulls, or aborted fetuses. The organism is sensitive to environmental conditions, and thus samples should be transported at ambient temperature, kept out of sunlight, not refrigerated, and delivered promptly to the diagnostic laboratory. The organisms are identified microscopically by their size (10 μm ? 15 μm), the presence of three anterior flagellae and an undulating membrane, and a characteristic jerky, rolling motion. PCR and quantitative PCR (qPCR) are often used now for identification of T. foetus because of their ability to differentiate T. foetus from contaminant, nonpathologic trichomonads. Due to the ability of T. foetus to degrade its DNA postmortem, improper sample handling may lead to false-negative results on both culture and PCR testing.54 Diagnostic testing of bulls using both culture and PCR may maximize sensitivity and specificity.53
There are no specific gross lesions in aborted fetuses. However, placentitis is a consistent microscopic lesion, and trichomonads can frequently be recognized in the placental stroma in histologic sections. Organisms may also be observed in the fetal lung in association with pyogranulomatous bronchopneumonia.55
■ Pathophysiology Trichomoniasis is transmitted venere- ally from infected bulls to cows or vice versa. The organisms colonize the vagina, cervix, uterus, and oviducts; cervicitis and endometritis ensue. Embryonic death frequently occurs within the first 2 months of infection, followed by a 2- to 6-month period of immunity to reinfection. Clearance of infection in cows commonly occurs within 95 days; infection rarely persists for as long as 6 months.51 However, infection in bulls older than 3 to 4 years of age is typically permanent and the main source of carryover from one breeding season to the next in beef cattle. Infection in younger bulls may be transient and related to the development of deeper mucosal folds in the prepuce as bulls age.53
■ Treatment and Control Systemic treatment of infected animals with imidazole compounds (ipronidazole, dimetridazole) is effective, but these compounds are prohibited in food animals in the United States.56,57 Infected cows should be either culled or given at least 3 months of sexual rest. The use of AI with semen from T foetus-negative bulls controls the disease once infected natural service bulls have been removed from the herd. In natural breeding situations, use of young virgin bulls and testing and culling of positive bulls older than 3 years of age will allow herd owners to gain control over the incidence of trichomoniasis. Vaccination of bulls and cows has shown some experimental benefit in limiting infection risk, but when all current research is evaluated extensively, vaccination appears to have very limited effect in reducing the risk of abortion.53
Neospora caninum Abortion
Abortion in cattle caused by N. caninum is relatively common and of economic importance, especially in dairy cattle. Congenital infection with limb paresis or dysfunction at birth as a result of encephalomyelitis may also occur. Canids are the definitive hosts and shed oocysts in their feces after ingestion of infected tissues from intermediate hosts (Fig. 43.9). Both the domestic dog and the coyote have been shown to transmit the oocysts in their feces.58-60 Along with cattle, deer have been shown to serve as intermediate hosts.60 The role of birds and wild rodents as intermediate hosts is suspected but has not yet been definitively demonstrated.60 Aborted, infected fetal tissues ingested by canids will also result in massive shedding of oocysts in feces.61 Transmission may be vertical (dam to fetus in utero) or via point-source horizontal transmission (ingestion of feed contaminated with feces containing oocysts).62,63 Horizontal transmission from cow to cow does not occur. Bovine fetal lesions are distinctive and may include nonsuppurative encephalitis with foci of necrosis and gliosis, nonsuppurative myositis, hepatitis, and, most consistently, myocarditis.37 Most abortions occur in the early second trimester, but they may occur throughout gestation. Diagnosis is based on characteristic lesions in aborted fetuses and seroepidemiologic study of an equal number of aborting and nonaborting herdmate cows if the proportion of seropositives is statistically higher in those that have aborted.64 Finding one aborting cow to be seropositive does not confirm N. caninum as the cause, and cows that abort once because of N. caninum are not protected from future abortion caused by this organism.
Sarcocystis Abortion
Sarcocystosis may cause abortion in cattle, sheep, and goats. Cattle are infected by Sarcocystis cruzi, sheep by Sarcocystis ovicanis, and goats by Sarcocystis capracanis.
■ History and Clinical Signs Most cattle are infected with Sarcocystis but do not show clinical signs of infection; however, massive or repeated infections may elicit depression, anorexia, weight loss, lameness, hair loss, emaciation, or death. Abortions occur in late gestation, usually in severely affected animals.65,66
■ Laboratory Diagnosis There are no specific gross lesions in the aborted fetus. Histologically, protozoa may be observed in villi and small arteries of the cotyledon or (more likely) the caruncle but are seldom seen in the bovine, ovine, or caprine fetus. Parasites are more likely to be observed in the fetal brain than in other tissues.65 Nonsuppurative inflammation may occur in the placenta or, less commonly, in fetal tissues, particularly the brain, heart, lung, liver, or kidney.65,66
FA demonstration of numerous developing protozoa in the cotyledon or caruncle is considered diagnostic. Caruncles are atrophied.65
■ Pathophysiology The pathogenesis of abortion in sarcocystosis is unclear. Generally, numerous spores are required to induce abortion experimentally. Fetal invasion by Sarcocystis is rare, and abortion may result from maternal fever, anemia, or placental insufficiency.65 Pregnant does apparently have diminished immunity to Sarcocystis, because low doses of S. capracanis result in fetal death without maternal illness if given in early pregnancy.67
■ Epidemiology Ruminants are infected by consumption of canid feces that contain oocysts. Sarcocystis occurs in the skeletal and cardiac muscle of most cows without associated lesions or clinical evidence of illness.
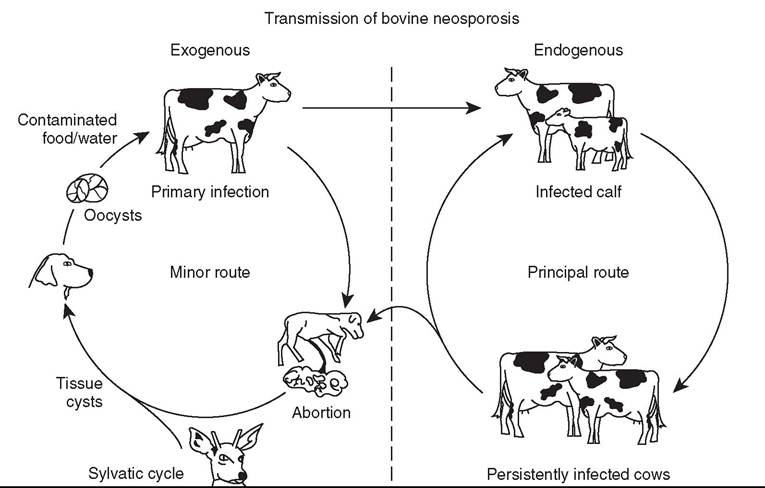
FIG. 43.9 Transmission of bovine neosporosis. Oocysts are produced by the canine definitive host, and their subsequent ingestion by a susceptible pregnant cow leads to infection of the fetus (exogenous transplacental transmission). Liveborn infected heifer calves would be expected to remain infected into adulthood, when they in turn may pass infection to their fetuses (endogenous transplacental transmission). Spread of Neospora caninum in this second way is the principal route whereby the parasite is propagated in a herd.
■ Control Effective therapeutic regimens for clinically ill animals have not been developed. For the life cycle of Sarcocystis to be broken, feeds should be kept free of dog or cat feces. These carnivores should not be allowed to eat aborted fetuses, placentas, or other ruminant carcasses.
Fungal Abortions
Mycotic Diseases That Cause Abortion
Fungal causes of bovine abortion include Aspergillus, Absidia, Mucor, Rhizopus, Candida, and Mortierella.69'69 Mycotic abortion is uncommon in sheep and goats.
■ History and Clinical Signs Mycotic abortions usually occur in the latter half of gestation (often near term) and seldom are associated with prodromal or postabortion clinical signs in the dam.
■ Laboratory Diagnosis The most consistent lesion is placentitis with necrosis and thickening of fetal membranes. In ruminants, both cotyledons and the intercotyledonary placenta are affected. Histologically, necrotizing inflammation of the chorionic villi is associated with vasculitis and thrombosis. Gross lesions may not be apparent in the fetus, but granulomatous bronchopneumonia is frequently observed histologically.69 In bovine aspergillosis the fetus is often near term with minimum autolysis and partially inflated lungs. Emaciation and dehydration with multifocal dry, scaly skin lesions occur in approximately 25% of affected fetuses. The fungus can be isolated from the fetus and placenta or demonstrated on histologic sections with special stains.
■ Pathophysiology The route of fungal infection in the bovine uterus is thought to be hematogenous.
■ Epidemiology Mycotic abortion generally affects only one or two animals in a herd and is more common in the winter. Fungi cause 3% to 10% of bovine abortions.70,71 Aspergillus spp. appear to be the most common fungal agent identified in mycotic abortion of cattle.
■ Control The only means of control of mycotic abortion is reduction of exposure to fungal agents.
■ Does and Ewes
Infectious Causes
See Table 43.9.
Bluetongue Abortion
Bluetongue is an orbivirus infection that can result in embryonic death, abortion, and fetal anomalies in sheep, cattle, or other ruminants. Twenty-six serotypes of bluetongue virus have been recognized; five of these (serotypes 2, 10, 11, 13, and 17) occur in the United States (see Chapter 32 for complete discussion).72
Border Disease (Hairy Shaker Disease)
Border disease or hairy shaker disease is an ovine pestivirus infection that causes embryonic and fetal death; stillbirths; dysplasia of the central nervous system, skeleton, and fleece; and birth of weak lambs with low viability.
Coxiella burnetii (Coxiellosis)
Coxiella burnetii is an obligate intracellular, pleomorphic bacterium that is related to the rickettsial family of bacteria.73,74 It is the causative agent of Q fever, which is the disease in human beings; the disease in livestock is called coxiellosis.74 Late-term abortions in sheep and goats, and rarely in cattle, are the primary clinical manifestation of disease. It is an important zoonosis worldwide. Subclinically infected ruminants 7374
are considered the primary reservoir of the agent., A variety of domesticated animals, including dogs, cats, and pigs, can also be infected, most often subclinically.
■ History and Clinical Signs Late-term abortions or delivery of stillborn or weak kids and lambs may occur in an affected herd or flock. Affected dams show little to no clinical signs of infection and are typically not ill prior to or after abortion. In cattle the most common manifestation of infection is conception failure and abortion.74
■ Laboratory Diagnosis Hygienic measures, including barrier gowns, eye protection, and respiratory protection, are prudent when handling suspect animals, fetuses, fetal membranes, and contaminated bedding. There are no specific gross lesions in the fetus, but the placenta is thickened with white, chalky plaques and red-brown exudate, especially in intercotyledonary areas. Diagnosis of Q fever abortion should be based on gross and histologic evidence of severe placentitis with large numbers of organisms visible using modified Koster stain, Stamp's modified Ziehl-Neelsen stain, or Gimenez stain. Culture of the organism is difficult; therefore PCR (ideally qPCR) can be used to detect the organism in the fetus, placenta, milk, or vaginal discharge.73 It is important to note that C. burnetii can be shed in the birthing fluids of normal ruminants; however, it is present in numbers far lower than encountered when this agent causes these animals to abort.74 Therefore, ideally, the diagnosis of Coxeilla abortion includes demonstration of compatible placental lesions, quantification of C. burnetii by qPCR, and documentation of the absence of other abortigenic agents. Serologic testing of aborting ewes and does (by ELISA, immunofluorescence assay, or complement fixation) typically shows seropositivity in aborting individuals, although titers may decline over time.74 Importantly, both seropositive and seronegative small ruminants may shed the organism, so the use of serology in determining infection status is problematic.74
■ Pathophysiology C. burnetii infection can be transmitted by infected ticks or by inhalation or ingestion of infected material. The organism replicates in trophoblasts, resulting in placentitis with late-stage abortion, stillbirth, or birth of weak offspring. Fetuses, fetal membranes, and uterine fluids from aborting animals contain massive numbers of the agent. The agent can persist in the environment as a durable sporelike particle called a small cell variant (SCV). These SCVs can persist in the contaminated environment and serve as a source of infection for naive animals.74
■ Epidemiology Coxiellosis is reported in many countries worldwide. Abortions typically occur over a 2- to 4-week period and may affect 5% to 50% of the flock. Because of the agent's zoonotic potential, pregnant women, immunosuppressed individuals, individuals with preexisting illness, and those with vascular grafts should not handle Coxiella-infected animals or tissues or be exposed to contaminated environments, as risk of Q fever is increased in such individuals. Aerosolization and inhalation of SCVs appears to be the most common means by which humans become infected during ruminant abortion outbreaks.
■ Treatment and Control As mentioned above, appropriate personal protective equipment is prudent when a suspected or confirmed abortion from C. burnetii is encountered. Aborting does and ewes should be segregated, and abortuses and placentas should be removed from the premises to prevent oral transmission. Farm cats and dogs should be kept out of contact with affected animals and their environment, as they may disperse the organism if allowed to feed on aborted materials. Affected animals should be situated on the premises so as to mitigate the risk of airborne transmission of SCVs to animals and people downwind of the area; an enclosed environment is ideal. Pregnant animals can be treated with tetracycline to reduce the chance of abortion, but further research on the efficacy of this measure is needed.
Vaccination of small ruminants is used in certain countries as a control measure. At present, no licensed vaccine is available in the United States or Canada, although provisional use in Canada may be allowed when the need is demonstrated.74 In a recent meta-analysis of the scientific literature conducted by Canadian investigators, use of inactivated vaccine containing a specific phase I antigen of C. burnetti reduced the risk of shedding of the organism in previously exposed goats and reduced the number of organisms shed in birthing fluids in previously unexposed goats.75 No effect on shedding risk was evident in vaccinated sheep.75
Cleaning and disinfection require removal of contaminated bedding and disposal by burial, burning, or composting. Soap and water scrubbing, followed by rinsing and application of an appropriate disinfectant (quaternary ammonium, 1% peroxygen, or 1:100 dilution of bleach), may reduce the environmental burden of SCVs. Appropriate personal protective equipment should be used by the personnel conducting cleaning and disinfection.
The potential for repeated reproductive loss and long-term carriage of the organism is a topic of active ongoing research. In one study goats were demonstrated to be capable of repeated reproductive failure and shedding of C. burnetii in two successive birthings.76 Strategies to manage abortion and mitigate further risk of abortion in affected herds and flocks are included in a 74
recent review.74
Campylobacter fetus subspecies fetus Abortion
C. fetus subsp. fetus is one agent of ovine campylobacteriosis (vibriosis) that causes abortion in sheep and sporadic abortion in cattle and goats.35,77
■ History and Clinical Signs Infection of ewes causes abortion in the last 6 weeks of pregnancy, stillbirths, and birth of premature lambs. Infected ewes may have fever, diarrhea, depression, and vaginal discharge several days before parturition.35,77 In cattle the infection is not associated with infertility (unlike infection with C. fetus subsp. venerealis), but sporadic abortions can occur.35
■ Laboratory Diagnosis Campylobacter causes necrosup- purative placentitis and multiorgan infection of the fetus. The fetus is edematous and may be pot-bellied in appearance. Multifocal, circular, pale foci—resembling donuts or targets— may be visible in the liver of roughly 25% of aborted ovine fetuses, and although these lesions are not pathognomonic, their presence is strongly suggestive of campylobacteriosis.35,77 Diagnosis is based on culture, PCR, or microscopic demonstration of the organism. Dark-field microscopic examination of wet mounts of fetal stomach contents or placenta may demonstrate the organism, which has a characteristic corkscrew shape.35 Histologic changes include suppurative necrotizing placentitis and pneumonia, gastroenteritis, hepatitis, and serositis in the fetus.35
■ Pathophysiology C. fetus subsp. fetus is transmitted by ingestion. It then translocates across the intestinal mucosa into the bloodstream, ultimately infecting the placenta and fetus.35 The incubation period is highly variable, ranging from 13 to 113 days (most commonly 14 to 21 days). The timing of initiation of infection appears to influence the incubation period.
■ Epidemiology Infection with C. fetus subsp. fetus is important in sheep in the United Kingdom, the United States, and New Zealand. Fetal infection is most common during the last 2 months of gestation. Outbreaks of abortion tend to occur in 4- to 6-year cycles.77 Infection is highly contagious in confined ewes, and the abortion rate may approach 70%.
■ Treatment and Control Abortion outbreaks due to C. fetus subsp. fetus may be treated with tetracyclines or macrolides. Tetracycline-class antimicrobials may not be effective against North American strains of Campylobacter jejuni, which is clinically indistinguishable from C. fetus subsp. fetus. Thus speciation of the isolate and antimicrobial susceptibility testing are critical to appropriate antimicrobial treatment.35,77 The efficacy of vaccination prior to the breeding season, as well as in the face of an abortion outbreak, appears to be quite variable and may depend on the degree of similarity between the vaccine and the abortigenic strain of C. fetus subsp. fetus.35
CampylobacteriIejuni Abortion
C. jejuni is the other agent of ovine Campylobacter (Vibrio) abortion. C. jejuni is an enteric pathogen that causes enteritis and diarrhea in many species. Only in sheep is placental and fetal infection common. This organism has been associated occasionally with abortion in cattle and goats.77-79
■ History and Clinical Signs Ovine infection with C. jejuni is clinically indistinguishable from that with C. fetus subsp. fetus.
■ Laboratory Diagnosis Lesions in placental and fetal tissues and diagnostic testing strategies are identical to those for C. fetus subsp. fetus.
■ Pathophysiology Intravenous inoculation of pregnant ewes with C. jejuni at 114 and 123 days of pregnancy consistently induced abortion 7 to 12 days later.80
■ Epidemiology and Control C. jejuni is ubiquitous and can be identified in the gastrointestinal tract of normal sheep.35 Abortion rates in excess of 25% are common, although the rate of abortion appears to vary among strains of this organism.77 Aborted tissue is infectious for humans and should be handled with caution. Treatment and control of ovine infection with C. jejuni are similar to those for C. fetus subsp. fetus. It should be reiterated, however, that most isolates of C. jejuni in North America are tetracycline resistant, so treatment of the remaining pregnant animals with macrolides or florfenicol is advisable.81 The protection afforded by commercially available C. jejuni vaccines appears variable and is not complete.35,81a
Brucella melitensis Abortion
Brucella melitensis causes abortion in goats and sheep and less commonly in cattle.81b Infection is associated with late abortion, stillbirth, or birth of weak kids or lambs. Necropsy findings include severe placentitis and fetal serositis. The disease is diagnosed by culture or demonstration of the organism in tissue or by maternal serology, although immunization is practiced in some countries, and this can interfere with interpretation of serologic tests.81b Infection with B. melitensis is important in Mediterranean countries and in Central and South America. Suspected cases should be reported to state and federal authorities, as this is currently exotic to the United States. Human infection with B. melitensis can be severe.
Brucella ovis Abortion
Brucella ovis infects only sheep. Epididymitis in rams is the most common manifestation of infection.82 Ewes seldom show clinical evidence of infection; late abortions, stillbirths, and delivery of weak lambs can occur but are very rare.82 Fetal and placental lesions resemble those induced by B. abortus. Notably, B. ovis has not been documented to be a zoonotic pathogen.
Chlamydophila abortus Abortion
(Enzootic Abortion of Ewes)
Chlamydophila abortus (formerly known as Chlamydia psittaci) is a gram-negative, obligate intracellular bacterium that is a major cause of abortion in sheep and goats.77,83 Ovine chlamydial abortion is called enzootic abortion of ewes.
■ History and Clinical Signs Late-term abortions or stillbirths with placentitis are characteristic findings. Offspring may be born alive but weak.77 The dam seldom shows signs of illness but may have serosanguineous vaginal discharge several days before and after parturition.
■ Laboratory Diagnosis Placentitis is the most consistent necropsy finding in chlamydial abortion. The placenta is markedly thickened with necrosis in the cotyledon and inter- cotyledonary areas; hemorrhagic exudate may be evident at the edges of these lesions.77 The fetus has no specific gross lesions and may be fresh, necrotic, or, rarely, mummified.77
Diagnosis of Chlamydophila abortion should be based on identification of the organism and the presence of typical placental lesions. Organisms appear in placental impression smears stained with Giemsa, Gimenez, or modified Ziehl-Neelsen stain as spheric bodies in the cytoplasm of trophoblasts. The organism can be positively identified by FA tests or by PCR.
■ Pathophysiology Chlamydophila spp. reside in the intestinal tract and are also shed from the genital tract of infected animals before and after parturition. Ingestion is the main form of transmission, resulting from exposure to aborted tissues, contaminated environment, or vaginal discharge. Transmission by infected rams and bucks appears possible. The incubation period appears to be long (60 to 100 days).77
■ Epidemiology Chlamydophila abortion has been reported in most major sheep- or goat-producing countries. The abortion rate in sheep is usually approximately 5% to 10% but may be up to 30% or more in goats. C. abortus also may infect other animals, including human beings.77,83 Pregnant women or immunosuppressed individuals should not handle infected animals or tissues, and personal protective equipment appropriate for C. burnetii exposure should be considered for individuals handling infected animals, aborted tissues, or contaminated bedding.
■ Treatment and Control Aborting does or ewes should be segregated, and abortuses and placentas should be removed from the premises to avoid oral transmission. Oxytetracycline therapy (80 to 450 mg/head every day in feed or water) has been used where allowed by law.84,85 Long-acting oxytetracycline injected subcutaneously at a dose of 20 mg/kg and repeated every 2 to 3 weeks may prevent further abortions.77 Vaccination may confer variable levels of protection, with the temperature-sensitive mutant vaccine available in Europe appearing to be more promising than the inactivated vaccines currently available in North America.77 Vaccination is described further in Chapter 48.
Toxoplasmosis Abortion
Toxoplasma gondii is a ubiquitous protozoan that is a major abortifacient in sheep and goats but only rarely causes abortion in cattle or horses. Exposure to kittens is an expected component of the history, either through direct contact or fecal contamination of feed or water. The organism is transmitted to sheep and goats by ingestion of oocysts present in feline feces.77 Cats shed heavy numbers of oocysts in the first 2 to 4 weeks after becoming infected by ingestion of infected rodents, birds, carrion, or aborted fetuses and tissues.77
■ History and Clinical Signs Infection does not cause clinical illness in the adult but may result in embryonic death, fetal death and abortion, stillbirth, or birth of weak, nonviable lambs or kids. Mummification of fetuses may occur, and mummified fetuses may be aborted along with stillborn or weak but live newborns.77
■ Laboratory Diagnosis The most characteristic gross lesion of toxoplasmosis is the presence of white, chalky foci of necrosis and calcification up to 2 mm in diameter in cotyledons.86,87 The intercotyledonary areas of the placenta are grossly normal. Specific gross lesions may not consistently exist in the aborted fetus, but histologically most have nonsuppurative encephalomyelitis,87 and many also have pneumonia, myocarditis, or hepatitis. Tachyzoites may be found in placenta or other fetal tissues but are not numerous.88,89 The tachyzoites are oval (2- to 4-mm ? 4- to 8-mm) with a central nucleus and appear larger in impression smears than in paraffin sections. Several serologic tests, including the modified agglutination test, indirect FA test, Sabin-Feldman dye test, indirect hemagglutination test, and ELISA, reliably detect toxoplasmosis in pleural or amniotic fluid or presuckling serum from nondecomposed fetuses.90,91 The modified agglutination test is commercially available, safer, and more sensitive than the dye test. Fetal antibodies to T. gondii can be detected 35 days after infection.86 Absence of fetal antibody does not always preclude a diagnosis of toxoplasmosis. High maternal titers are not diagnostic of toxoplasmal abortion, but lack of titer eliminates toxoplasmosis as the cause for abortion.86 The peroxidaseantiperoxidase method for detecting Toxoplasma antigen in fetal tissues or placenta is reliable even in autolyzed fetuses. Fetal heart, lung, brain, spinal cord, skeletal muscle, and placenta are the preferred specimens for the peroxidase-antiperoxidase method and should not be held in formalin more than 2 days before paraffin embedding.89
■ Pathophysiology Placental infection occurs approximately 14 days after ingestion of oocysts.89 Infection acquired before 50 days' gestation may result in embryonic death and resorption. Infection between 60 and 100 days' gestation usually causes fetal death or birth of weak lambs. Infection during the last month of gestation often has no apparent effect on the fetus.86 In experimental infection of ewes between 6 and 14 weeks of pregnancy, abortions occurred 1 to 2 months after inoculation.91 In natural infections, most abortions occur 1 month before parturition.86
■ Epidemiology Toxoplasmosis is a major cause of ovine abortion in many sheep-raising countries, including the United States.87,88 Sheep are infected by ingestion of oocysts from feed, water, or grass contaminated with cat feces. Aborted tissues may be infectious for humans and should be handled with caution.92
■ Control Infected ewes or does seldom abort from toxoplasmosis in subsequent pregnancies.87 The prevalence of abortion can be reduced by avoiding contamination of foodstuffs with feline feces. Cats should not be allowed to eat placentas or carcasses that may contain tachyzoites or tissue cysts. Farm cats should be spayed or neutered to limit birth of young, susceptible kittens. In endemic areas, exposing replacement ewes to aborting ewes or cat feces before breeding age may induce immunity.
■ Camelids The incidence of abortion in llamas and alpacas is low. Infectious causes in North America include leptospirosis, toxoplasmosis, chlamydophilosis, and other nonspecific uterine infections. Bovine virus diarrhea is considered an emerging disease in alpaca herds and may be responsible for some of the early pregnancy losses and abortions in some herds. Diagnostic work-up for abortion in camelids is similar to that described in this chapter for other species.
■