Abnormalities of the Ovaries
Mares
Abnormally Small Ovaries
The most common causes of bilaterally small ovaries in the mare are (1) seasonal anestrus, (2) hypothalamopituitary dysfunction, (3) severe malnutrition, (4) immaturity, (5) advanced age, (6) use of anabolic steroids, and (7) gonadal dysgenesis.
Clinical signs and treatment of seasonal anestrus, hypothalamopituitary dysfunction, and malnutrition are discussed elsewhere in this chapter.Immaturity and Advanced Age
The average age at which fillies reach puberty is 18 months, with a wide range of 10 to 24 months. Fillies younger than 2 years of age with inactive ovaries and a flaccid and relaxed reproductive tract may be too young to cycle and should be reexamined later. The condition should be differentiated from gonadal dysgenesis, and karyotyping may be indicated if puberty is delayed beyond 24 months.
Older mares (>20 years) not only frequently begin cycling later in the season than do younger mares but also often have a longer follicular phase and, subsequently, a longer interovulatory interval.12,13 Equine serum AMH levels that are related to antral follicle count have been shown to increase with age.14 Some mares reach ovarian senescence when they grow older 12,15,16 and typically have small, inactive ovaries (follicles both estrous behavior and ovarian size and function. The treatment of mares with low doses of anabolic steroids can cause aggressive or stallion-like behavior, whereas high doses can inhibit ovarian activity and result in failure of follicular development and ovulation.18 Prolonged treatment of prepubertal mares with anabolic steroids results in hypertrophy of the clitoris.19 Ovarian inactivity in mares treated with anabolic steroids is often reversible, and pituitary and ovarian function eventually return to normal in most mares after withdrawal of the treatment.
However, mares intended for breeding should not be treated with anabolic steroids.Progestins are commonly given to cycling mares for the suppression of estrus or synchronization of ovulation. Mares may continue to ovulate during progestin administration, especially if treatment is started late in the luteal phase. A high incidence of persistent CL formation has been observed in mares that ovulate during progestin treatment.20 Administration of the potent GnRH agonist deslorelin acetate to induce ovulation has been associated with delayed follicular development and a prolonged interovulatory interval.21,22 Deslorelin acetate is effective in inducing ovulation, but treatment appears to cause a temporary downregulation of FSH secretion. The low FSH concentrations have been associated with a prolonged period of decreased follicular growth. Administration of PGF2α 7 to 8 days after ovulation appears to increase the risk of delayed follicular development. It has been suggested that PGF2α administration “resets” the timing of the estrous cycle during a period when limited follicular activity is present.
■ Treatment and Prognosis Removal of the deslorelin implant after ovulation has been detected to decrease the incidence of prolonged interovulatory intervals.23
GONADAL DYSGENESIS. Chromosomal abnormalities occur in all breeds of horses. Mares are usually small and phenotypi- cally female. The ovaries are small, firm, smooth, and inactive. The tubular tract is thin and flaccid. Endometrial hypoplasia is a common finding. Diagnosis is confirmed by physical findings and karyotype. Mares with gonadal dysgenesis are sterile, and there is no treatment.
PITUITARY PARS INTERMEDIA DYSFUNCTION. Mares with hypertrophy, hyperplasia, or adenoma formation in the pars intermedia of the pituitary (pituitary pars intermedia dysfunction [PPID]) have been reported to have abnormal estrous cycles, infertility, or both.24,25 The mechanisms by which PPID causes reproductive abnormalities have not been determined.
Potential causes may be destruction of the gonadotrophs of the anterior pituitary owing to compression by the enlarged pars intermedia and/or suppression of gonadotropin secretion owing to elevated levels of glucocorticoids or androgens produced by the adrenal cortex.26 In support of the glucocorticoid hypothesis, administration of dexamethasone to intact mares results in reduced estrous behavior, LH concentrations, follicular growth, and incidence of ovulation.27 In addition, administration of dexamethasone to ovariectomized mares results in suppression of pituitary LH and FSH secretion,28 and treatment of pony mares with dexamethasone during the winter eliminates estrous behavior.29 However, others have shown that abnormally high levels of cortisol secretion has a minimal effect on fertility.30 Many PPID horses are insulin resistant, and insulin is believed to play a role in the regulation of ovarian steroidogenesis and follicular development.31 Obese mares with reduced insulin sensitivity have been shown to have prolonged interovulatory periods. Insulin resistance therefore may be one mechanism by which PPID mares exhibit abnormal ovarian function.32 Most horses diagnosed with PPID are older, with the average age being approximately 20 years. Consequently the decrease in reproductive efficiency in mares with PPID may be partly a result of advanced age.Clinical signs of PPID include hirsutism and abnormal hair-coat shedding patterns, polyuria, polydipsia, and hyperhidrosis.33 Diagnostic tests for PPID include measurements of serum glucose, insulin, adrenocorticotropic hormone (ACTH), and cortisol levels; dexamethasone suppression; ACTH stimulation; and thyrotropin-releasing hormone response.34 The measurement of single samples for basal cortisol or ACTH concentrations is of limited value in the diagnosis of PPID.
■ Treatment and Prognosis The medical management of PPID includes the administration of pergolide mesylate, a dopamine receptor agonist, at a dose of 0.002 to 0.01 mg/kg every 24 hours (1 to 5 mg/500 kg) in an adult horse.
Because of its dopaminergic agonist effect, treatment with pergolide mesylate should be avoided in late pregnant and lactating mares. Treatment of pregnant mares can be discontinued at 30 days before expected foaling until 1 month postpartum, and the mares should be monitored for adequate milk production. Foals should be supplemented with a milk replacer when insufficient milk production is suspected in the dam. The serotonin antagonist cyproheptadine has also been used, but it may not be as efficacious as pergolide. The dose of cyproheptadine is 0.25 mg/kg every 24 hours, given once in the morning.EQUINE METABOLIC SYNDROME. Equine metabolic syndrome (EMS) is not clearly defined, and intense research in this area is expected to shed further light on the understanding of this condition in horses. Altered circulating concentrations of leptin and adiponectin have been observed in horses with EMS, and an effect on reproductive cycles in mares has been suggested, but existing data are not conclusive.35-37 In fact, moderately obese mares are more likely to cycle year-round compared to lean mares.38
EMS has been associated with regional obesity, insulin resistance, and laminitis.39 A presumptive diagnosis is often based on body condition score and signs of regional obesity, history of laminitis, and insulin resistance.40
■ Treatment and Prognosis Controlled diet and exercise are important components in the management of mares with suspected EMS. Medical treatment with metformin at a dose of 15 to 30 mg/kg and levothyroxin sodium at a total dose of 48 mg has been suggested.39 However, scientific evidence of the safety and efficacy of these drugs is insufficient in horses. Metformin has not been evaluated for safety in pregnant mares, but it is considered safe to use in pregnant women.41 The effect of human maternal hyperthyroidism on the fetus should be considered before levothyroxin is used in pregnant mares.
Abnormally Enlarged Ovaries

FIG. 43.3 Granulosa cell tumor removed from a mare.
mare (Fig. 43.3), and 10% of all neoplasms in horses are GCTs. It is usually slow growing, unilateral, and benign; however, malignant tumors have been reported. It occurs in mares of all ages and parity2,4 and is occasionally found in pregnant mares.2,5 The tumor arises from the steroidogenic cells of the follicle, resulting in abnormal secretion of inhibin and testosterone.
■ Clinical Signs and Diagnosis Diagnosis of GCTs is made based on ultrasonographic findings, histologic evaluation, hormone profile analysis, and behavioral observations. Tran- srectal ultrasonographic examination of the affected ovary often reveals a multicystic or honeycombed structure, but the tumor may also occur as a solid mass or as a single large cyst. In most cases the GCT affects only one ovary, and the contralateral ovary is usually small and inactive, although mares with a GCT on one ovary and a functional contralateral ovary have been reported.
GCTs are hormonally active, and clinical diagnostic assays for the detection of a GCT include the measurement of inhibin (α-inhibin), testosterone, progesterone, and AMH.7-11 α-Inhibin is elevated in approximately 90% of the mares with a GCT.8,10 It has been hypothesized that inhibin produced by the GCT is responsible for inactivity of the contralateral ovary through the suppression of pituitary FSH release, but the poor correlation between dimeric inhibin and the presence of GCT raises questions about the mechanism by which the contralateral ovary is suppressed in affected mares.10,13 Serum testosterone in a single blood sample can be expected to be elevated (100 to 200 pg/mL) in approximately 50% to 60% of affected mares. Daily fluctuations in testosterone concentrations have been reported, and repeated samples may have to be obtained on different days in order to detect elevated testosterone.
Progesterone concentrations in mares with a GCT are almost always below 1 ng/mL because normal follicular development, ovulation, and CL formation do not occur. Serum levels of AMH in mares with GCTs are consistently higher than in normal cyclic and pregnant mares, and this provides an excellent tool in the diagnosis of GCT. As a result of hormone secretion from the tumor, mares may show anestrus, constant estrus, irregular estrus, or stallion-like behavior. Physical changes such as an enlarged clitoris, increased muscle mass, and the development of a crested neck have been associated with GCTs, and other clinical signs such as colic, lameness, and weight loss have been observed.2■ Treatment and Prognosis Treatment for GCTs is removal of the affected ovary. Surgical approaches for tumor removal include colpotomy, flank and ventral midline laparotomy, and laparoscopy. The prognoses for both life and reproductive use are good. The time from surgery to return to cyclicity varies, but most mares cycle in the year after ovariectomy.
CYSTADENOMAS. The most common tumor of the surface epithelium of the equine ovary is cystadenoma. They are rare, benign, normally hormonally inactive tumors from the surface epithelium of the ovulation fossa. The tumor is unilateral, and the contralateral ovary is normal.
■ Clinical Signs and Diagnosis Mares with cystadenomas cycle normally from the opposite ovary and may become pregnant if bred. Rectal palpation and ultrasonography reveal the presence of one enlarged multicystic ovary, which may appear similar to a GCT, and one normal ovary; however, final diagnosis is histologic.
■ Treatment and Prognosis Although cystadenomas are benign tumors and do not affect the reproductive performance of the mare, they are usually surgically removed if diagnosed. The prognoses for both life and reproductive performance are excellent.
GERM CELL TUMORS. Dysgerminomas and teratomas are rare ovarian tumors of germ cell origin. Both tumors are unilateral and hormonally inactive.
■ Clinical Signs and Diagnosis Both tumors make the affected ovary unilaterally enlarged and multicystic. Dysger- minomas are malignant and do often metastasize to the peritoneal and thoracic cavities. Teratomas may arise from all three germinal layers, and the neoplastic ovary may contain bone, cartilage, teeth, hair, muscle, and nerves. Teratomas do not cause clinical signs, interrupt the estrous cycle, or alter the behavior of the mare. Diagnosis of dysgerminomas and teratomas is made using ultrasonography and histologic evaluation of the affected ovary.
■ Treatment and Prognosis Surgical removal is recommended for both dysgerminomas and teratomas. The prognosis for teratomas is usually good, but it is poor for mares diagnosed with dysgerminomas.
■ Anovulatory Follicles
Clinical Signs and Diagnosis
Ovulation failure is a normal physiologic event for the mare during the spring and fall transition periods, but it may also occur occasionally during the physiologic breeding season. Persistent anovulatory follicles (PAFs) may be quite large (5 to 15 cm in diameter), persist for up to 2 months, and result in abnormal estrous behavior and prolonged interovulatory intervals. The cause of ovulation failure is still being determined, but it has been suggested to be due to gonadotropic stimulation insufficient for ovulation, reduced estrogen production by the follicle, blockage of the ovulation fossa, repeated use of ovulation-inducing drugs, alterations of the matrix metalloproteinase system, and defects in the normal ovarian proangiogenic activity. PAFs have been reported to occur in approximately 8.2% of estrous cycles, and significantly more mares 16 to 20 years of age developed anovulatory follicles than mares 6 to 10 years of age. The formation of an anovulatory follicle was preceded by development of normal endometrial folds or edema in 78.3% of these cases. Initial growth patterns of follicles destined to become anovulatory were usually normal, and the first indication of a problem was the detection of echogenic particles within the follicular fluid.22
PAFs may contain blood and have been called hemorrhagic anovulatory follicles. The hemorrhage can be detected ultrasonically
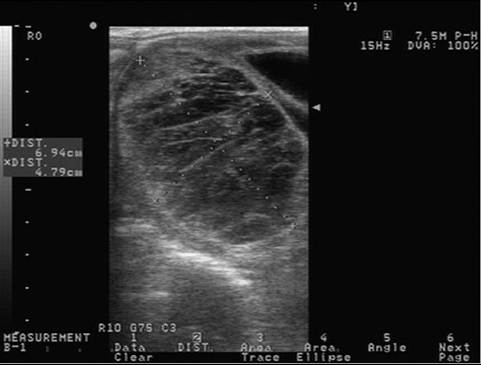
FIG. 43.4 Transrectal ultrasonographic image of a persistent anovulatory follicle in a mare.
as scattered free-floating echogenic spots within the follicular fluid. The follicular fluid may form a gelatinous, hemorrhagic mass within the follicular lumen. Ultrasonographically these structures may contain echogenic fibrous bands traversing the follicular lumen (Fig. 43.4). 2 3 6 * * * * * * * * * * * * A thickening of the follicular wall may be observed in anovulatory follicles. This thickening is often associated with luteinization of the follicular wall, and 85.7% of PAFs were found to be luteal structures based on elevations in plasma progesterone concentrations.22
■ Treatment and Prognosis Treatment with hCG or a GnRH agonist to induce ovulation or luteinization of the anovulatory follicle is generally not effective. The administration of prostaglandins may result in the destruction of the luteal cells in mares with luteinized PAFs. Most nonluteinized PAFs spontaneously regress in 1 to 4 weeks. Pregnancy does not usually occur if a persistent follicle eventually spontaneously ovulates or is induced to ovulate. This is likely a result of degeneration of the oocyte over time. Pregnancy obviously will not occur if the follicle becomes hemorrhagic or luteinized without ovulation.
Ovarian Hematoma
■ Clinical Signs and Diagnosis Hemorrhage into the follicular cavity is a normal occurrence at ovulation. Occasionally hemorrhage is severe, resulting in the formation of an ovarian hematoma that may be 10 cm in diameter or larger. Diagnosis can be made using transrectal palpation and ultrasonography, and the condition presents as an enlarged ovary that is initially irregularly hypoechoic and then echogenic with organization of the hematoma. Ovarian hematoma should not be mistaken for a GCT, since the ovulation fossa usually remains distinguishable on the affected ovary, and the contralateral ovary remains active.
■ Treatment and Prognosis Ovarian hematomas regress spontaneously over a period of weeks or months. The functional life span of the luteal tissue in a hematoma is normal, and ovarian activity is unaffected. Because the affected ovary is not permanently damaged and the contralateral ovary is unaffected, the prognosis for fertility is undiminished.
Pregnancy
Multiple secondary CLs form in pregnant mares at 40 to 180 days of gestation, resulting in bilaterally enlarged ovaries that may be mistaken for ovarian pathology.
■ Clinical Signs and Diagnosis Ovarian enlargement is commonly bilateral. Pregnant mares may show stallion-like behavior associated with increased testosterone production from the fetus during midgestation. Pregnancy should always be considered in a mare with stallion-like behavior, elevated serum testosterone concentrations, and enlarged ovaries. Pregnancy is diagnosed by rectal palpation and ultrasonographic examination.
Persistent Corpus Luteum
■ TABLE 43.4
Unilaterally Large Ovary: Differential Diagnosis
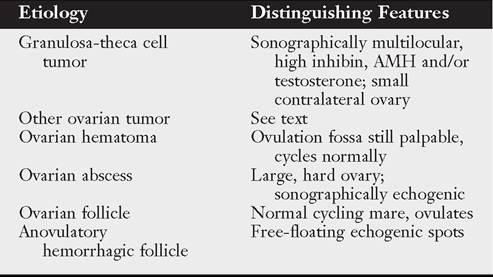
AMH, Anti-mullerian hormone.
ultrasonographic or rectal examination of ovarian follicular activity should therefore always be performed before PGF2α is administered to induce estrus.
Shortened Luteal Phase (Premature Luteolysis)
Premature (the uterine pole is flat and triangular and shows converging striations. The affected part is devoid of follicles. Animals with partial ovarian hypoplasia can be expected to have a reduced superovulatory response to gonadotropin treatment. Heifers with abnormal karyotypes are also affected by ovarian hypoplasia. The condition should be differentiated from nonfunctional ovaries and anestrus associated with malnutrition or debilitating diseases. Treatment of ovarian hypoplasia is not successful.
Ovarian Tumors is based on transabdominal or transrectal ultrasonographic evaluation of the ovaries. Treatment is ovariectomy.
DOE. Ovarian neoplasia appears to be rare in does as well. Granulosa cell tumors and dysgerminomas have been reported.
Ovarian Hemorrhage
Cow
Ovulation tags develop after ovulation, resulting from blood loss associated with rupture of the follicle. Fine adhesions may develop between the ovarian surface and surrounding structures. Most ovulation tags resolve spontaneously and have no effect on fertility. Severe ovarian hemorrhage may follow attempts to manually enucleate the CL. Adhesions between the ovary and its bursa interfere with their normal function. Enucleation of CLs for treatment of anestrus and pyometra has been superseded by treatment with PGF2α products.
Oophoritis
Cow
Inflammation of the ovary may follow traumatic manipulations, such as enucleation of CLs and attempts to drain fluid from ovarian cysts, and ascending infections from the uterus. Oophoritis may also accompany brucellosis, mycoplasmosis, and tuberculosis.