Largeintestine
Lateral and ventrodorsal radiographs of the pelvic region can provide helpful information in dogs and cats with constipation, hematochezia, or painful defecation. Abnormalities of the colon such as obstruction, megacolon, and obstipation can usually be recognized radiographically.
Since a large quantity of feces may be present in the colon prior to defecation in a normal animal, the finding of a radiographically distended co-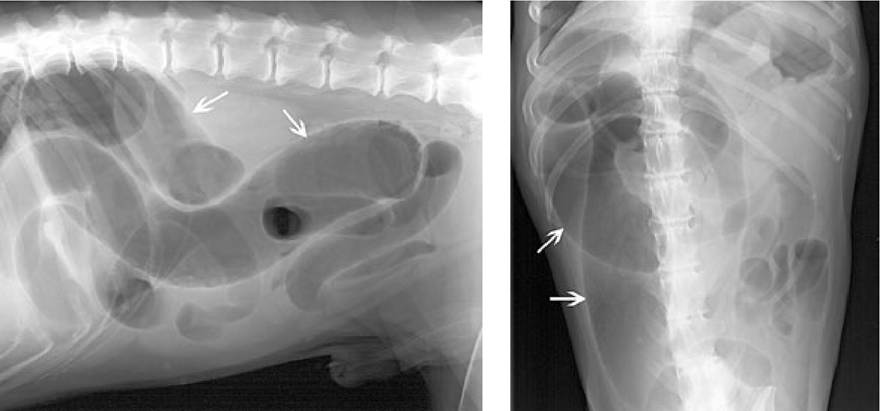
Figure 1.31:
Colonic torsion. Lateral and ventrodorsal abdominal digital radiographs of a 13-year-old German Shepherd dog with anorexia for 5 days and weakness in the hind limbs. Borborygmus and a tympanic abdomen were additional findings. Most of the gastrointestinal tract is dilated and air-filled. The entire colon (arrows) is severely dilated and air-filled. At the pelvic inlet, the gas pattern of the colon ends abruptly. Diagnosis: colonic torsion.
lon must be evaluated relative to the patient’s clinical signs. Although not common, colonic torsion can occur causing severe dilation and displacement of the colon from its normal location (Figure 1.31). Mechanical obstruction due to previous pelvic trauma or space-occupying lesions can be ruled out radiographically. Sublumbar lymph node enlargement, extension of retroperitoneal masses, prostatomegaly in male dogs and uterine masses in females, and the presence of perineal herniation can also be detected radiographically. Dilation of the colon (greater than the length of a lumbar vertebra) with impaction of feces with increased radiopacity can be due to constipation, obstipation, or megacolon. Increased soft tissue opacities or displacement or compression of the colon within the pelvic canal indicate the need for further imaging procedures such as ultrasonography.
Ultrasonographically, the ileum, ileocecal junction, cecum, and ascending, transverse, and descending colon can be identified. When distended, the wall should have the appearance of having three layers and a thickness of 1-2 mm. The empty colon will appear contracted and many layers can be appreciated. This should not be misinterpreted as colonic wall thickening. Due to the presence of air and feces, it is often difficult to examine the entire colon by ultrasound. The bony pelvis also limits examination of the colon, but the rectum as well as the perirectal and perineal regions can be examined via a perineal approach. However, a certain length of rectum within the pelvic canal cannot be examined in both dogs and cats. If the region of interest within the pelvic canal cannot be assessed due to overlying bone, radiographic contrast studies can be helpful in determining the origin of soft tissue masses causing displacement or compression of the colon. Negative and positive contrast studies of the colon may be performed, but they may be difficult to interpret due to the presence of intestinal contents or lack of experience with the procedure. Barium enemas can be useful in the diagnosis of ileocolic intussusceptions, cecal inversions, strictures, or wall infiltrations.
In dogs with diarrhea due to colitis, the colon may appear normal or irregular in form and may be air or fluid filled. Colitis due to diffuse, mild to moderate inflammatory infiltration will often show no radiographic or ultrasonographic changes and colonoscopy is the diagnostic method of choice in both dogs and cats. Soft tissue lesions such as neoplasia of the colon can be recognized radiographically as localized increased soft tissue opacities. However, they are not always evident on survey radiographs, and either a positive or negative contrast study of the colon may be required. Sonographically, focal infiltrations or intramural masses of the colonic wall may be detected and are associated with either neoplasms or granulomas (Figure 1.32).
Both MRI and CT are alternative methods for examining the pelvic region or determining the involvement of the colon and surrounding tissues, especially when space-occupying lesions are present in that region.
Figure 1.32:
Colonic neoplasia. Ultrasound image of the descending colon of a 12-year-old European short-haired cat with a history of tenesmus and hematochezia. Ultrasonographically, an irregular localized infiltration (4 mm) of the wall of the colon just cranial to the pelvis can be identified. The wall layering is disrupted and the echotexture is complex. The regional lymph nodes were found to be enlarged and rounded. Histological diagnosis: mucinous carcinoma.
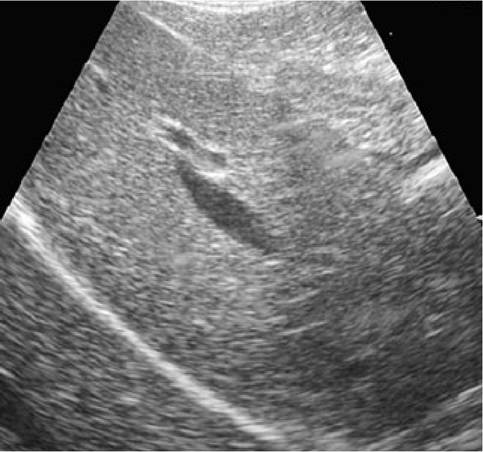
Figure 1.33:
Normal canine liver. The liver has a medium echogenicity. Both portal (hyperechoic walls) and hepatic (no walls) veins are visible.
1.3.6