Smallintestine
1.3.5.1 Ileus
Ileus is a failure of the intestinal contents to be transported and is recognized radiographically by the presence of dilated bowel segments. Survey abdominal radiographs should always be performed in animals suspected of having ileus.
Ultrasound alone in such instances does not allow a global view of the abdomen, is much more time-consuming, and non-gastrointestinal causes of the patient’s clinical signs as well as any secondary abnormalities may be overlooked. The radiographic appearance of ileus is dependent on its duration, location, and type. Acute or very proximal obstructions may show little intestinal dilation radiographically, whereas chronic or more distally located obstructions will show more severely dilated bowel segments. The two major types of ileus are obstructive (mechanical) and functional. Obstructive ileus may be partial or complete, and can be due to foreign bodies, torsion, volvulus, herniation, intussusception, adhesions, granulomas, and neoplasms.Barium passage through the small intestines can be used to identify intraluminal, mural, or extramural obstructive as well as non-obstructive or partially obstructive lesions. However, it is a lengthy procedure and depending on the technique and experience of the clinician, may be difficult to interpret. Barium is also contraindicated prior to endoscopy or ultrasound, as it causes significant attenuation of sound and acoustic shadowing.
a
c
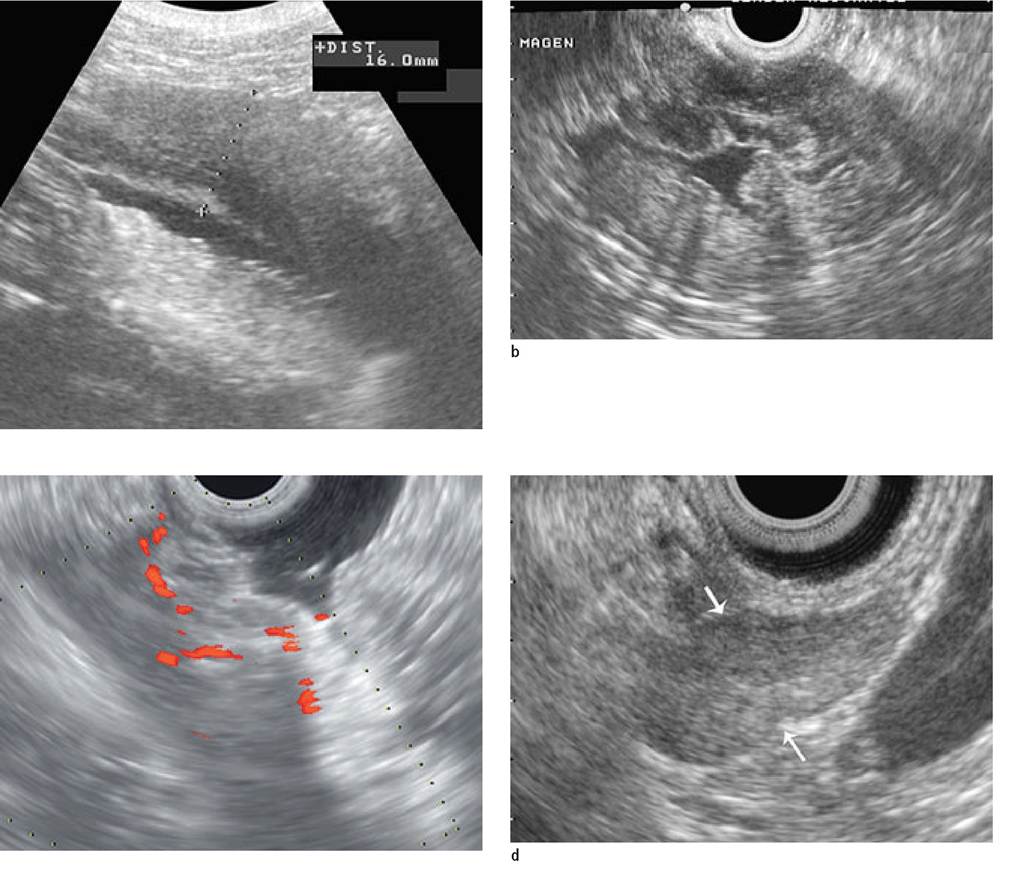
Figure 1.22a-d:
Gastric carcinoma.
(a) Transabdominal ultrasound image using a 7.5-MHz curved array transducer in a 45-kg Leonberger dog with chronic vomiting and weight loss. Localized thickening (1.6 cm) of the gastric wall with disruption of wall layering was identified.
(b) The dog underwent anesthesia for gastroscopy and an endoscopic ultrasound examination of the stomach was performed.
The infiltration could be better localized to the lesser curvature of the stomach.(c) In addition, Doppler showed the lesion to be well vascularized.
(d) The gastric lymph nodes were found to be enlarged and rounded (between arrows). Intraoperatively, the mass was non-resectable. Diagnosis: gastric carcinoma.
1.3.5.2 Partial obstructions
Fasted (>12 hours) or anorectic animals should not have small bowel segments containing granular material resembling that of food. Granular or more opaque small bowel contents may be detected in patients with a partial obstruction. The intestines in such cases may be mildly dilated (1-1.5 times the width of the second lumbar vertebral body [L2]) proximal to the obstruction or may be of normal diameter (Figure 1.23). Because fluid passes through the narrowed lumen, the contents remaining proximal to the partial obstruction become more dense and, therefore, radiographically more opaque (Figure 1.24).
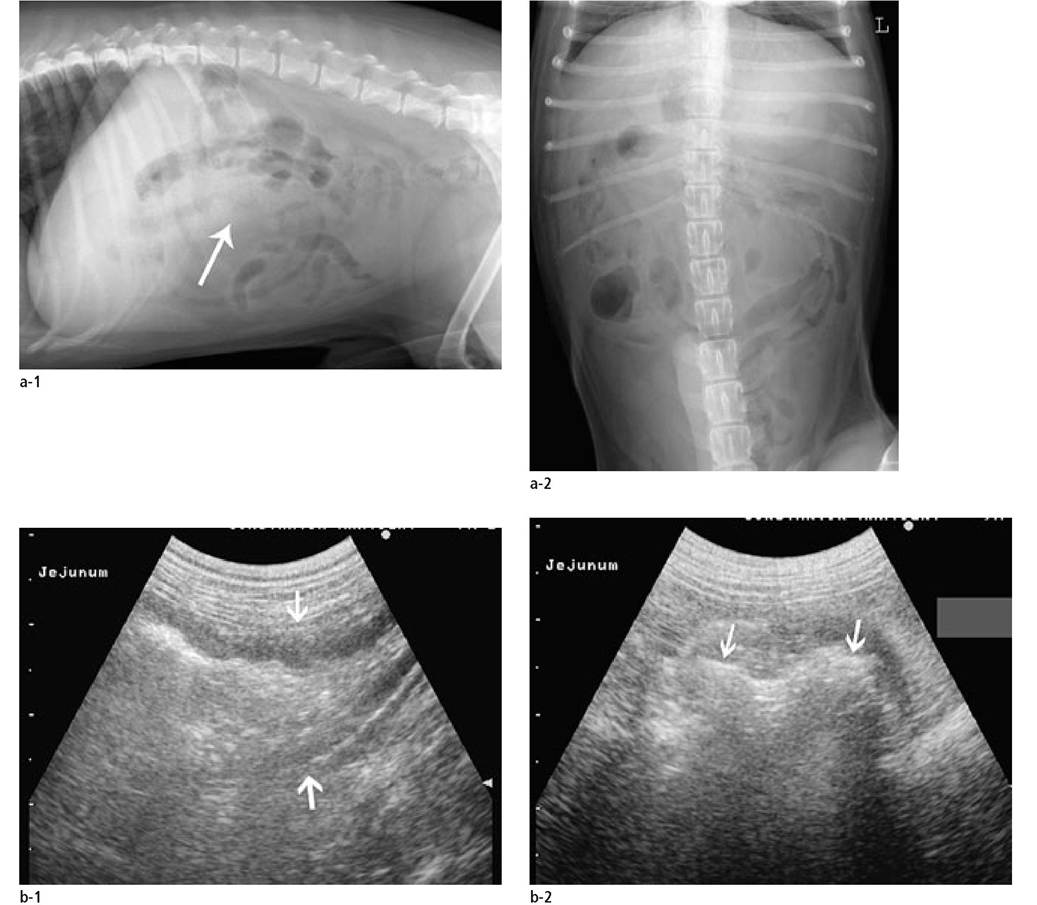
Figure 1.23a, b:
Small intestinal foreign body. Radiographic and ultrasonographic investigation of a 6-year-old West Highland White Terrier with a 1-month history of vomiting and weight loss. Upon clinical examination the dog's abdomen was painful.
(a) Lateral and ventrodorsal abdominal digital radiographs. There is a loss of mid-abdominal detail (white arrow) with mildly dilated small intestines. Although the dog was fasted over 12 hours, some of the small intestines have a granular content, which is difficult to differentiate from feces in the colon in this dog.
(b) An ultrasound examination showed dilated and fluid-filled jejunal segments proximal to an intraluminal structure with a hyperechoic wavy surface and acoustic shadowing. An unidentifiable foreign body was removed from the site surgically.

Figure 1.24a-c:
Small intestinal neoplasia.
(a) Lateral (left) and ventrodorsal (right) abdominal digital radiographs of the abdomen of a 9-year-old, castrated male European short-haired cat with a 5month history of anorexia and weight loss. The cat's condition worsened 3 days prior to admission. The radiographs show cachexia with loss of abdominal detail. The majority of the small intestinal segments are severely dilated and air-filled. In the caudoventral abdomen there are multiple mineral opaque structures clumped together. Note that the descending colon is visible and filled with feces.
(b) Dilated and fluid-filled distal jejunal segment (between arrows). The wall is thickened (x-x) with disrupted wall layering. The irregular hyperechoic structures with clean distal shadowing are the stones that have collected proximal to the long-standing obstruction.
(c) The site of stenosis shows that the wall is thickened with an outer hypoechoic and inner hyperechoic wall layering. The regional lymph nodes (not shown) were enlarged and inhomogeneous. Histological diagnosis: adenocarcinoma.

b
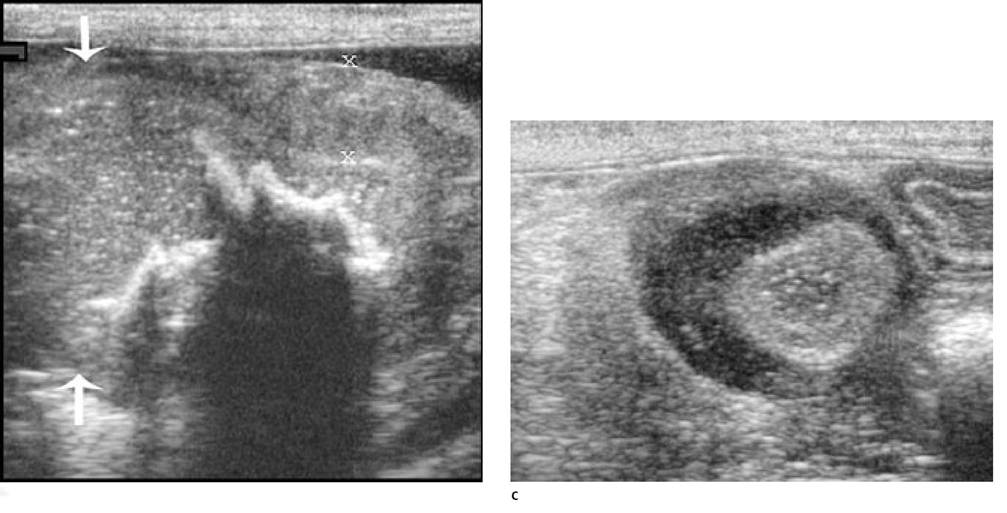
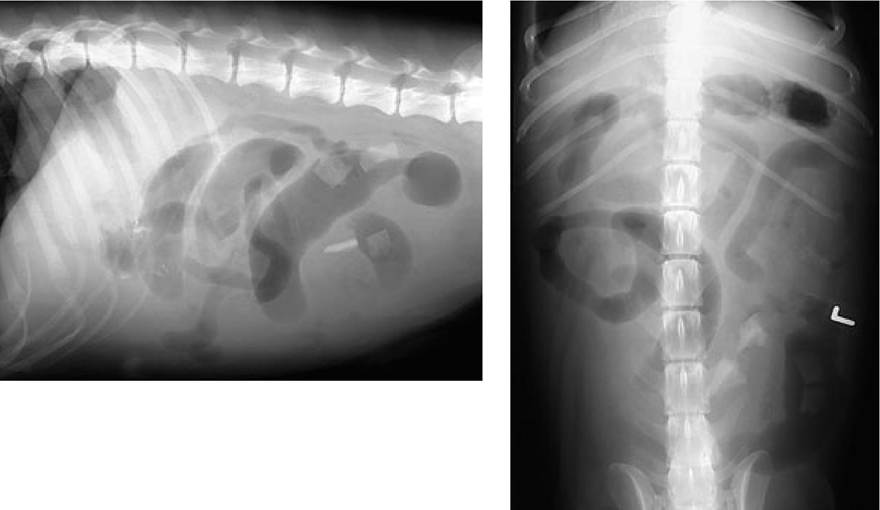
Figure 1.25:
Intestinal obstruction. Lateral and ventrodorsal abdominal radiographs in a dog with vomiting. Note that a few segments of small intestine are severely dilated and gas-filled while others are only mildly dilated. Foreign material with mineral opacity within the jejunal segments is also seen but was not the cause of obstruction. Diagnosis: mid-jejunal mechanical ileus due to radiolucent foreign body.
1.3.5.2 Complete obstructions
More severe dilation, usually with air, is seen in patients with complete obstructions (Figure 1.25). Dilation (1.5-2 times the width of the body of L2) is seen proximal to the site of obstruction and the segments distal to it usually appear empty and contracted.
Due to this, the jejunal segments appear to have highly variable diameters. This is due to the continued peristaltic activity in the distal segments. Feces may still be present in the colon depending on the duration of the obstruction. Proximal duodenal or pyloric obstructions may show no radiographic abnormalities. Distal jejunal obstructions may cause generalized dilation and resemble a functional ileus radiographically.1.3.5.3 Functional ileus
Another form of ileus that can be detected is a generalized and uniform mild intestinal dilation due to lack of peristaltic activity (Figure 1.26). This is known as adynamic, functional, or paralytic ileus. Functional ileus results in obstruction since the intestinal contents pool in the dependent areas of the gastrointestinal tract. It may affect the stomach, small and large intestines. Radiographically, the bowels may have a homogeneous soft tissue opacity when they are fluid-filled or a mixed pattern of air and fluid may also be present. Such an adynamic intestinal pattern can be due to the administration of pharmaceutical agents such as parasympatholytics or sedatives. Other causes are peritonitis, blunt abdominal trauma, electrolyte imbalance, or enteritis of various causes. Dysautonomia is a disorder of the autonomic nervous system that can also lead to generalized dilation of the gastrointestinal tract in both dogs and cats.28 A complete obstruction in the distal jejunum or at the ileocecal level may also lead to the same radiographic appearance. Decreased peristalsis may be limited to the duodenum in patients with pancreatitis.
1.3.5.4 Detecting ileus with ultrasound
Generally, the clinical state of the animal in conjunction with radiographic findings provides adequate information to make a determination as to whether there is obstructive disease requiring surgery or not. However, when abdominal radiographic findings are unclear, an obstruction cannot be ruled out, or the radiographic findings do not explain the severity of the clinical signs, further diagnostic procedures are warranted.
Ultrasonography has the advantage that it does not require ionizing radiation and can be used to inspect the small intestines for wall layering, thickness, dilation, and peristalsis as well as for intraluminal, intramural, and extraluminal causes of obstruction. Lack of peristalsis occurring together with generalized dilation of the small intestines can be seen with functional ileus.29 Contractions can be observed in two-dimensional real time imaging and approximately 5 contractions per minute are considered normal for the stomach and 1-3 are considered normal for the small intestine.
Radiolucent intestinal foreign bodies may be detected by ultrasound, especially when they cause mechanical obstruction. Solid material generally appears as a hyperechoic interface, which casts an acoustic shadow from the intestinal lumen.30 Balls will have a round or curvilinear surface, peach pits are irregular, and bones generally have a smooth regular surface. Linear foreign bodies can sometimes be identified in plicated segments of small bowel. Foreign bodies tend to remain fixed in the same position and a repeat examination a short time later shows that they have not moved. The finding of severe dilation of one or more segments of the jejunum and the stomach together with empty, contracted bowel segments distally may indicate complete or partial obstruction. Care should be taken not to misinterpret a gas-liquid interface in dilated bowel segments as an obstruction. These appear as linear, hy- perechoic intraluminal structures with acoustic shadowing. However, the bowel will often have a similar diameter proximally and distally to this artefact. This is usually not the case with intraluminal foreign bodies causing obstruction.
Localized mural infiltrations due to inflammation or neoplasia can slowly narrow the intestinal lumen. Some degree of intestinal dilation is present and solid foreign material such as small stones can collect proximal to the stricture.
Ultrasonographically, neoplastic infiltrates produce intestinal wall thickening often with a loss of wall layering.31 Lymphoma is the most common intestinal tumor in cats but also occurs frequently in dogs. It commonly leads to either a symmetrical or asymmetrical, transmural, circumferential thickening. The wall layers are difficult to identify and the entire wall appears hypo- to anechoic. The infiltration of the intestinal wall may be solitary, diffuse, or multifocal and regional lymph nodes may be enlarged. Complete intestinal obstructions often do not occur. Intestinal carcinoma often produces a solitary intestinal mass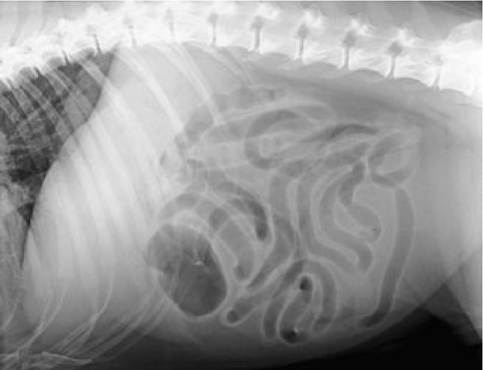
Figure 1.26:
Functional ileus. Lateral abdominal digital radiograph of a dog with vomiting and diarrhea for 2 days. The small intestines are moderately dilated, of uniform diameter, and air-filled. Diagnosis: functional ileus.
as can polyps, leiomyomas, or leiomyosarcomas. Carcinomas tend to be annular, irregular infiltrations that invade the lumen and cause obstructions.32 Regional lymphadenopathy can also commonly be identified. Granulomatous infiltrations due to fungal infections may also cause diffuse or focal infiltration of the bowel wall and are difficult to distinguish from neoplasia ultrasonographically.33 Histoplasmosis, for example, can produce localized and severe wall infiltrations that resemble lymphoma. Jejunal smooth muscle hypertrophy has been described in the cat and can also cause focal wall thickening but the wall layering is maintained.34 Because the ultrasonographic appearance of the bowel wall alone is not sufficient for a definitive diagnosis, either full thickness biopsies, ultrasound-guided percutaneous biopsies, or fine-needle aspirates of the bowel wall are required for a definitive diagnosis of fungal disease.
1.3.5.5 Complicated ileus
Complicated forms of ileus include bowel perforation with peritonitis, free air in the abdominal cavity, and bowel ischemia due to thromboembolism, intussusception, or volvulus at the root of the mesentery. Linear foreign bodies can also lead to a complicated form of ileus. The presence of pneumoperitoneum together with abdominal effusion on an abdominal radiograph should alert the clinician to the fact that bowel perforation has occurred. The detection of free intra-abdominal air may require the use of ventrodorsal horizontal beam radiography with the patient in left lateral recumbency. Free air


Figure 1.27a, b:
Linear foreign body.
(a) Lateral and ventrodorsal abdominal radiographs of a dog presented for vomiting. Note the “ribbon candy” appearance of the dilated and air-filled small intestinal segments. Irregularly shaped gas opacities can be seen in adjacent intestinal segments.
(b) Ultrasound image of a linear foreign body. The intestines appear plicated and pulled together. Although not always visible, in this case a string was identified sonographically (arrow).
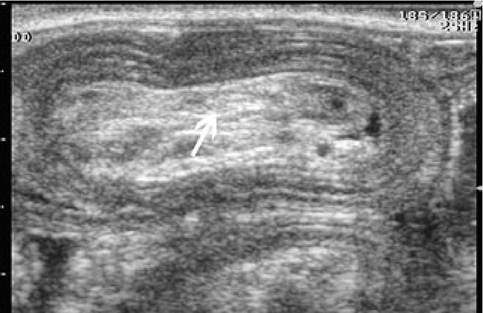
Figure 1.28:
Intussusception. Ultrasound image of a jejunal intussusception in a young dog with diarrhea. Note the concentric intestinal layers. The hyperechoic center represents invaginated fat.
can be detected just under the right abdominal wall and lateral to the duodenum. Volvulus or mesenteric thromboembolism are recognized by the presence of generalized, severely dilated and air-filled jejunal segments. Linear foreign bodies produce characteristic changes on abdominal radiographs in both dogs and cats (Figure 1.27). The small intestinal loops appear convoluted and gathered or clumped together at one site (usually in the mid-right abdomen) and intraluminal gas bubbles appear asymmetrical and irregularly shaped. Ultrasonographically, the small intestinal segments will appear gathered up with the linear foreign material binding them together. The surrounding mesenterium should be examined for increased echogenicity and free fluid, which could be indicative of rupture.
Intestinal intussusception can usually be quickly diagnosed with ultrasound. Multilayered, concentric rings of bowel can be identified (Figure 1.28). The outer bowel segment is often thickened, edematous, and hypoechoic. More normal appearing inner segments can also be identified. Hyperechoic tissue representing invaginated mesenteric fat may also be detected. In older animals, careful examination of the affected bowel for nodular infiltrations of the bowel wall and regional lymphad- enomegaly is important since underlying neoplastic disease may be responsible for the intussusception.
1.3.5.7 Chronic diarrhea
Chronic diarrhea due to small intestinal disease is common in dogs and cats. Survey radiographs are often nonspecific and gastrointestinal contrast studies are often unrewarding in patients with chronic diarrhea without vomiting. For detecting intestinal wall infiltrates, ultrasound is superior to survey and contrast radiography. Abdominal ultrasound allows for an assessment of wall thickness and layering, localization of lesions, motility, and potential involvement of regional lymph nodes. Recently, investigators have tried to correlate intestinal wall thickness in healthy dogs with body weight.35 In that report the authors suggested normal values for jejunal wall thickness of ≤4.1 mm for dogs up to 20 kg, ≤4.4 mm for dogs between 20 and 39.9 kg, and ≤4.7 mm for dogs over 40 kg. Normal duodenal wall thickness was reported to be ≤5.1 mm for dogs up to 20 kg, ≤5.3 kg for dogs between 20 and 29.9 kg, and ≤6.0 mm for dogs over 30 kg.
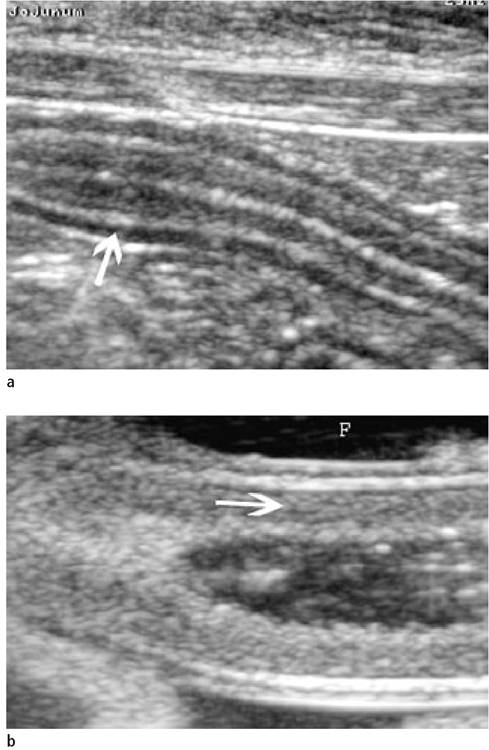
Figure 1.29a, b:
Eosinophilic enteritis and protein-losing enteropathy.
(a) Ultrasound image of a jejunal segment of a cat with an eosinophilic inflammatory infiltrate of the small intestine. The muscularis layer (arrow) was found to be very prominent.
(b) Ultrasound image of a jejunal segment of a dog with protein-losing enteropathy due to lymphangiectasia. The wall thickness is normal (3.8 mm), but the mucosa is hyperechoic and there is free fluid in the abdomen. The entire jejunum was affected. These sonographic findings are common in dogs with this syndrome.
1.3.5.8 Diffuse bowel wall infiltration
A number of gastrointestinal diseases lead to diffuse infiltration of the small intestinal wall. There are no known specific sonographic features that allow differentiation of the different infiltrative diseases. However, ultrasonography is important for localizing lesions within the gastrointestinal tract and allowing further characterization of the degree of infiltration inferred by wall thickness and the appearance of wall layering. The
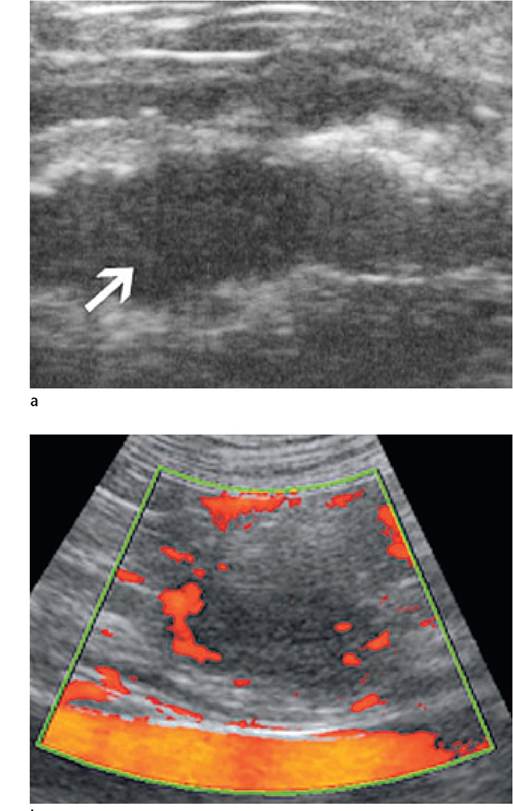
Figure 1.30a, b:
Intestinal lymphoma.
(a) Ultrasound images of a 9-year-old mixed-breed dog with chronic diarrhea, anemia, and weakness. Multifocal, hypoechoic, 1.2 cm diameter intestinal wall infiltrations were identified throughout much of the jejunum.
(b) Although Doppler examination initially showed no vascularity, following intravenous injection of 1 ml of Sonovue® ultrasound contrast medium, numerous peri- lesional and intralesional vessels were seen. Percutaneous, ultrasound-guided fine- needle aspiration of the intestinal wall was performed. Diagnosis: Lymphoma.
mucosal, submucosal, and muscularis layers are most commonly affected (Figure 1.29). The mucosa may also exhibit alterations in echogenicity varying in severity from diffuse pinpoint hy- perechogenic foci to generalized hyperechogenicity. Severe mucosal thickening with increased echogenicity may be seen in animals with PLE and lymphangiectasia. In addition, the small intestine generally shows some dilation with fluid and gas and may have a decreased motility or a rigid appearance.
Thickening of the intestinal wall or a single layer due to inflammatory disease is difficult to differentiate from neoplastic infiltration. For example, a thickened muscularis layer alone can occur with either inflammatory or neoplastic infiltrates or can be due to smooth muscle hypertrophy. Lymph nodes may appear rounded, heterogenous, and possibly show target lesions in patients with either disease. Mycotic diseases such as histoplasmosis, pythiosis, and cryptococcosis can produce localized infiltrative disease that is sonographically similar to that of localized neoplasia.33 However, neoplasia is considered to produce more disruption of the wall layering compared to inflammatory disease.36 Sonographic changes in patients with alimentary lymphosarcoma may include thickening of the stomach or intestinal wall, loss of normal layering, a hypoe- choic mass associated with the intestinal wall (Figure 1.30), and abdominal lymphadenomegaly.37,38
1.3.5.9 Gastrointestinal hemodynamic assessment with Doppler ultrasound
Dogs presenting with chronic diarrhea may be examined with Doppler ultrasound. Spectral Doppler waveforms of the celiac and cranial mesenteric arteries are generated at fasting and at 20, 40, 60, and 90 minutes postprandially.39 Resistive (RI) and pulsatility indices (PI) calculated from these waveforms infer the degree of resistance to blood flow in the distal vascular bed of the intestinal tract. In a colony of Soft-coated Wheaten Terriers with food allergy, a prolonged lowered resistance (lowered RI and PI values) to blood flow was identified in response to stimulation with mucosal allergens.40 More work will need to be carried out in this field in order to judge the clinical utility of this method in the assessment of dogs with chronic gastrointestinal disease.
1.3.6