Liver and biliary tract
Clinical signs of hepatobiliary disease can be nonspecific and include anorexia, apathy, vomiting, diarrhea, polyuria, polydipsia, and icterus. The presence of icterus in the absence of anemia indicates hepatobiliary disease in both dogs and cats.
Abdominal ultrasonography is the most useful non-invasive diagnostic tool for differentiating hepatic vs. post-hepatic causes of icterus. In cats, hepatic causes of icterus such as hepatic lipidosis are more common than pre- or post-hepatic disease. The liver, gallbladder, biliary tract, duodenal papilla, and pancreas should be examined with a high frequency transducer. Generally, curved array transducers with a small foot print are advantageous for examining these structures due to their location just behind and underneath the curvature of the ribs. Ultrasonographically, hepatic size can be estimated and its internal architecture, including its portal, venous, arterial, and biliary vasculature in addition to its echogenicity and echotexture can be evaluated (Figure 1.33). The wall thickness and contents of the gall bladder as well as the size of the cystic and the bile duct can also be assessed. In addition, the proximal duodenal papilla can be assessed for signs of obstruction. Finally, involvement of the pancreas in the disease process can also be assessed.1.3.7.1 Hepatic parenchymal disease
Ultrasonographic changes in patients with hepatic parenchymal disorders are generally either focal or diffuse. Diffuse processes are more difficult to recognize than focal or multifocal ones and a change in the echogenicity of the liver is the main ultrasonographic finding. The liver may appear normal or have an increased, decreased, or mixed echogenicity.
In patients with acute liver disease, the liver may appear normal or enlarged with a generalized decrease in echogenicity. When the echogenicity is decreased, the portal veins appear much more visible, i.e.
more hyperechoic than usual (Figure 1.34). This finding is nonspecific and the differential diagnoses may include toxic injury, infectious hepatitis, metabolic disease, trauma, vascular compromise, cholangiohepatitis, amyloidosis, lymphoma, or passive congestion.Increased echogenicity of the liver can be detected in a number of conditions including fatty infiltration, steroid hepatopathy, and chronic hepatic diseases, such as hepatitis, cirrhosis, malignant histiocytosis, or lymphosarcoma.41,42,43
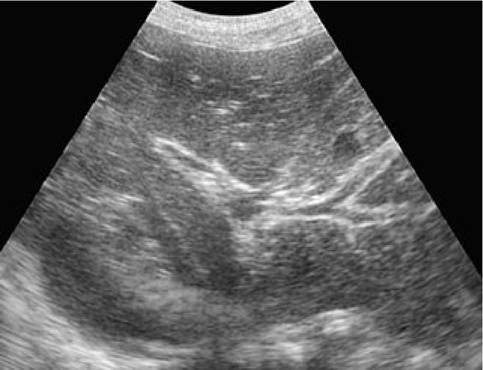
Figure 1.34:
Cholangiohepatitis. Ultrasound image of a hypoechoic liver in a 2.5-year-old male Cairn Terrier with icterus and vomiting. The liver is enlarged, hypoechoic, and the portal veins are very prominent and hyperechoic throughout the entire liver. Histopathologic diagnosis: cholangiohepatitis.
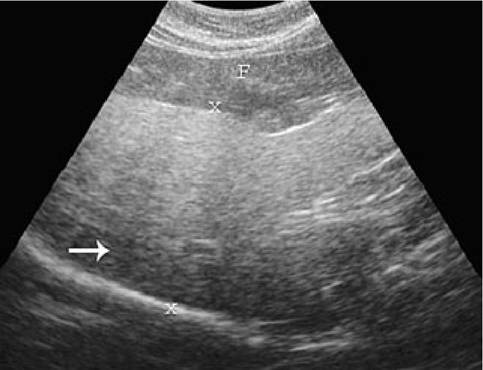
Figure 1.35:
Hepatic lipidosis. Ultrasound image of a hyperechoic liver in a 16-year-old, male European short-haired cat that presented with anorexia. The hyperechoic liver (between x-x) is homogenous and few vessels are visible. The echogenicity is equal to or greater than that of the spleen and surrounding mesentery and falciform fat (F). Note the hypoechoic appearance of the liver dorsally (arrow) due to beam attenuation. Differential diagnoses include hepatic lipidosis, diabetes mel- litus, and neoplasia. Cytologic diagnosis: hepatic lipidosis.
Feline hepatic lipidosis is a common source of intrahepatic cholestasis that can be recognized ultrasonographically (Figure 1.35). The liver of affected cats is enlarged, rounded, shows an increased echogenicity equal to or greater than that of the spleen. In addition, the liver may appear isoechoic or hyper- echoic compared to omental fat and hyperechoic to falciform fat.44 Beam attenuation may also occur and the dorsal region of the liver may be difficult to visualize.
The appearance of vascular structures is also diminished. Cytologic examination of a fine-needle aspirate is usually adequate for diagnosis of hepatic lipidosis.Cirrhosis and end-stage chronic inflammatory disease is rare in cats compared to dogs, but hepatic fibrosis may be seen in cats. Hepatic cirrhosis and chronic hepatitis are difficult to diagnose by ultrasound. Furthermore, they can have a similar appearance as neoplastic disease. The liver may be small or normal in size and may contain nodules. Ascites may or may not be present. The nodules tend to be round and distinct and the surrounding liver may be of normal or increased echogenicity. Ultimately, a biopsy or fine needle aspiration is needed to make a more definitive diagnosis.
In the presence of ascites without venous hepatic congestion, spectral Doppler evaluation of the portal vein can be used to rule out portal hypertension. The velocity of the portal venous flow in patients with cirrhosis is generally reduced.45 In the presence of portal hypertension and ascites, secondary portosystemic shunts may be detected. Secondary shunts can be recognized by the presence of many tortuous vessels in the abdomen. Doppler ultrasound will show the flow within these vessels to be monophasic and of low velocity, identifying them as portal in origin. In such instances, a surgical mesenteric portogram or a scintigraphic portogram is indicated (Figure 1.36).46 Helical CT is a new alternative approach in veterinary patients with suspected portosystemic shunts.47 Also, contrast harmonic ultrasound has been investigated in dogs for the detection of congenital portosystemic shunts.6
Diffuse hepatic changes with mixed echogenicity may also be seen in some patients. Neoplasia is the most common cause when the hepatic parenchyma appears diffusely complex or disrupted with poorly circumscribed areas of both increased and decreased echogenicity. Other possible causes of a complex echostructure in the liver are inflammation, toxicity, or
necrosis.
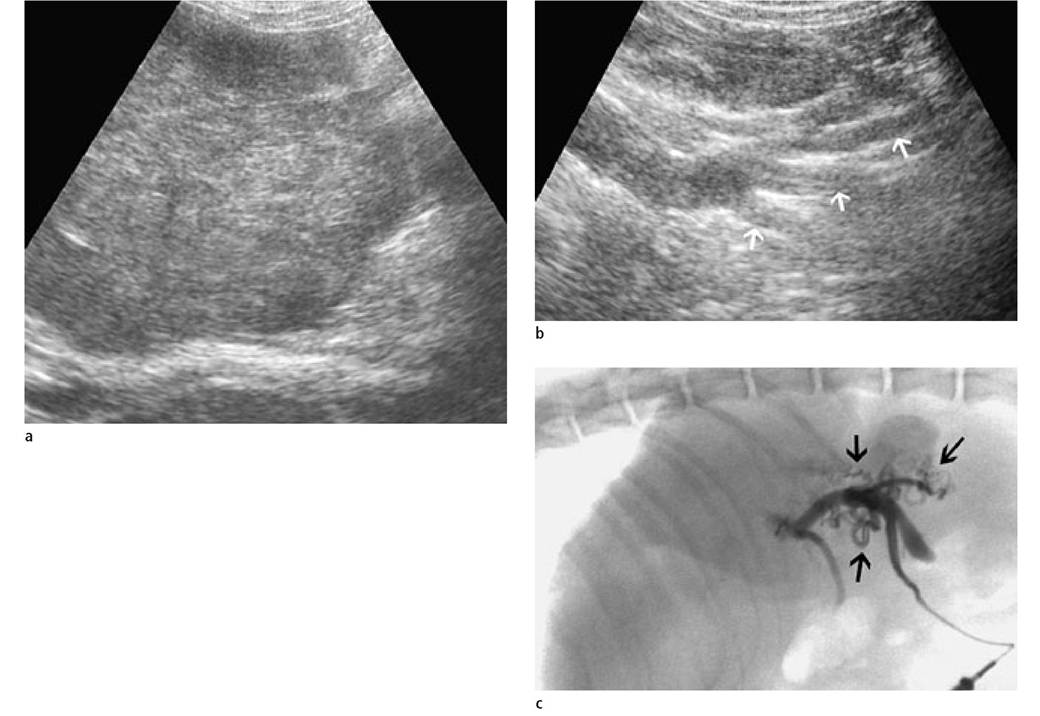
Figure 1.36a-c:
Extrahepatic portosystemic shunts.
A 2-year-old female mixed-breed dog weighing 10 kg was presented with apathy and intermittent diarrhea. The serum chemistry profile showed hypoglycemia, hypoalbuminemia, and elevated pre- and postprandial bile acids concentrations.(a) Ultrasound image of the liver. The liver was rounded, inhomogeneous, and had an irregular surface.
(b) Numerous aberrant vessels (arrows) with low velocity monophasic flow were identified caudal to the stomach and there was free fluid in the abdomen. Portal venous flow was greatly reduced at only 5 cm/sec. In addition, uroliths were identified in the urinary bladder.
(c) Intraoperative mesenteric venous portogram. Multiple, tortuous shunting vessels (arrows) are shown. A normal portal vasculature could not be demonstrated in this liver. Diagnosis: secondary extrahepatic portosystemic shunts due to chronic liver disease.
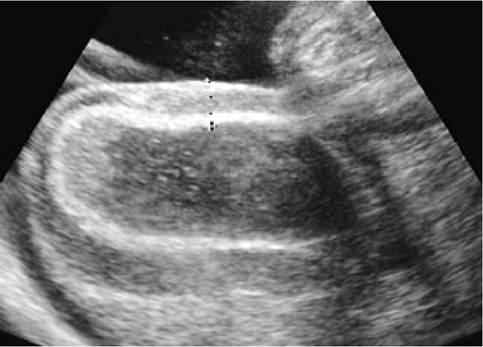
Figure 1.37:
Gall bladder wall edema. Ultrasound image of the gall bladder in a 5-month-old mixed-breed dog that presented with weight loss and inappetence of 3 weeks' duration. Serum hepatic enzyme activities and bilirubin concentration were elevated and there was a clinical suspicion of hepatitis. Ultrasonographically, the liver was hypoechoic with prominent portal vein walls. The gall bladder showed a “double-walled appearance". The gall bladder wall was 8 mm thick and hypoechoic with an inner and outer hyperechoic rim. Ascites was also detected. Note that the double-walled appearance in this instance is not due to the presence of ascites since the thickened wall itself can be visualized. Diagnosis: gall bladder wall edema.

Figure 1.38:
Biliary mucocele. Ultrasound image of the gall bladder in an 8-month-old, male Rhodesian Ridgeback that was presented for vomiting of 2 days' duration and a painful abdomen.
Radiographs of the abdomen showed signs of obstructive ileus and an ultrasound examination was performed. An invagination was diagnosed. In addition the liver and kidneys were enlarged and the gall bladder contents showed a complex echostructure with a thickened wall. The dog was diagnosed with leptospirosis, cholangiohepatitis, and a biliary mucocele. (Image courtesy of Dr. Johann Lang, Division of Radiology, Faculty of Veterinary Medicine, University of Bern, Switzerland.)Contrast-enhanced ultrasonography has been found to be very useful for differentiating benign from malignant hepatic disease in human beings.5,48 However, there are few reports describing its use in the assessment of dogs and cats with hepatic disease.
1.3.7.2 Non-obstructive biliary tract disease
Cholecystitis is a form of non-obstructive biliary disease and is usually seen with inflammation due to bacterial infection. The infection may spread to the liver causing cholangiohepa- titis. If the cholecystitis is necrotizing, the infection may eventually lead to gall bladder rupture and bile peritonitis.
Thickening of the gall bladder wall is a common ultrasonographic finding in patients with cholecystitis and cholan- giohepatitis.49 Varying amounts of gall bladder sediment may be identified but this finding is nonspecific. Choleliths and mineralization of the gall bladder wall may also be seen but their significance is dependant on the clinical findings. The thickened wall is generally hyperechoic, possibly with an irregular inner surface. Polyps may occur in patients with chronic cholecystitis and appear as focal or multifocal wall infiltrations or nodules. Neoplasia could have a similar appearance, but gall bladder tumors are rare.
The gall bladder may also appear to have two echogenic double rims with a hypoechoic space in between (Figure 1.37). This double-walled appearance of the gall bladder can be seen with hypoalbuminemia, ascites, sepsis, acute inflammatory disease, or neoplasia.
The presence of even small amounts of peritoneal fluid can create the appearance of a thickened gall bladder wall. Therefore, caution should be used in the interpretation of the gall bladder wall in patients with ascites.Emphysematous cholecystitis may be detected radiographically as a zone of hyperlucency in the right cranioventral region of the liver. Ultrasonographically, reverberation echoes either within the gall bladder lumen or the wall may be recognized. This type of “dirty” shadowing can be differentiated from the “clean” shadowing that is seen with calculi in the gall bladder.
Gall bladder mucoceles are important findings in patients with hepatobiliary disease and icterus and various sonographic patterns have been described (Figure 1.38).50 Gall bladder mucoceles have the potential to rupture and may cause bile peritonitis. In general, the gallbladder wall is thickened and contents with a complex echostructure and echogenicity can be observed. Ultrasonographic evidence of ascites can indicate the presence of rupture and bile peritonitis.
s∣ooj, DijsouBeia %p
1.3.7.3 Obstructive disease
Ultrasound can be used to detect dilated and tortuous common and hepatic bile ducts, choleliths, or biliary and peri-biliary obstruction. Biliary calculi, pancreatitis, neoplasia, granulomas, or abscesses are possible causes of obstruction.51 Liver flukes in cats are another cause in tropical and subtropical climates. If the patient is anorectic or has been fasted prior to examination, the gall bladder can be very large, which should not be misinterpreted as biliary obstruction. If obstructed, the gall bladder enlarges prior to the intrahepatic bile ducts, which may take days to weeks to dilate. Also, the common bile duct may take days to dilate following obstruction.
The porta hepatis and cranial duodenum can be challenging regions to examine with ultrasound. The presence of food and gas in the gastrointestinal tract is one of the main barriers. With the use of high frequency transducers, however, the duodenal papilla and bile duct can even be seen in normal dogs and cats (Figures 1.39 a and b). Therefore, visualization of the bile duct should not be considered the sole criterion for biliary obstruction. The normal bile duct diameter should not be more than 4 mm in dogs and 3-4 mm in cats.52
Extrahepatic cholestasis can be recognized by a distended gall bladder and bile duct (Figure 1.39 c). The pancreas and duodenal papilla can be sources of obstruction that can be evaluated ultrasonographically (Figure 1.39 d). Pancreatic abscesses, cysts, neoplasia, and choleliths as well as pancreatitis may cause mechanical obstruction of the bile duct (Figure 1.39 e). Bile duct carcinoma, pancreatic carcinoma, or lymphosarcoma in cats are additional causes. Long-standing obstructions may lead to intrahepatic bile duct dilation (Figure 1.39 f ). Ultrasonographically, “too many vessels” can be visualized in the liver that do not show any blood flow when examined with color Doppler. Differential diagnoses for tubular fluid-filled structures in the liver are obstruction, biliary cysts, pseudocysts, biliary cystadenomas, and bile duct carcinoma.
Nuclear scintigraphy and contrast radiography are not commonly performed for the diagnosis of hepatobiliary disease in dogs and cats, but quantitative cholescintigraphy can be used to diagnose extrahepatic biliary obstruction.53 Moreover, nuclear scintigraphy using Tc-99m-mebrofenin shows promise in dogs for the quantification of hepatic function.54 Endoscopic retrograde cholangio-pancreatography (ERCP) uses a combination of endoscopy and fluoroscopy for radiographic contrast imaging of the biliary and pancreatic ducts. Investigators experienced with this method were able to identify an enlarged common bile duct, intraductal filling defects, a deviated course of the common bile duct, and a stenosis of the major duodenal papilla in some affected canine patients. This imaging modality requires specialized equipment and training, but may be promising for the diagnosis of biliary and pancreatic diseases in dogs in the future. 55, 56
1.3.7.4 Interventional procedures of the liver and biliary system
Interventional procedures such as fine-needle aspiration or biopsy of the liver and pancreas can be performed using a 16- to 18-gauge biopsy needle depending on the size of the animal. Both manual and spring-loaded instruments may be used. Recently, the sensitivity and specificity of cytology and histology of tissue samples collected by fine-needle aspiration has come under criticism.57 A coagulation profile should be performed prior to percutaneous true-cut biopsy, but it is not necessary prior to fine-needle aspiration unless there is a clinical suspicion of a coagulopathy. Complications following liver biopsy are extremely rare. Percutaneous ultrasound-guided cholecystocentesis can be performed for cytologic and bacteriologic analysis with a high degree of safety in dogs and cats. A 22-gauge, 1.5-inch (3.81-cm) needle with an attached 12-mL syringe is used via a right-sided transhepatic approach. Alternatively, a right ventral abdominal approach into the fundus of the gallbladder can be used.58
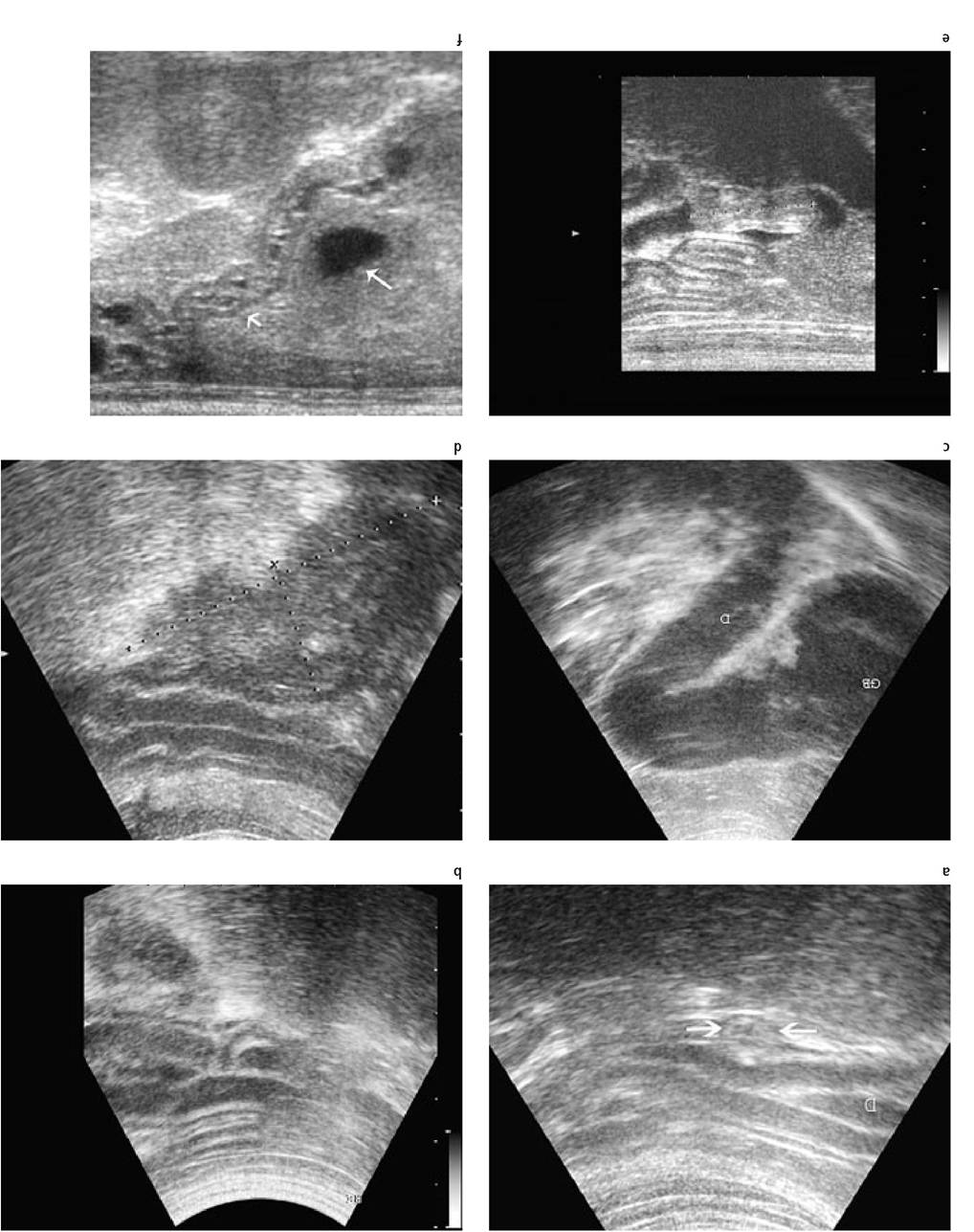
Figure 1.39a-f:
Ultrasonographic assessment of the bile duct.
(a) Normal duodenal papilla in a cat.
(b) Normal common bile duct entering the duodenal papilla in a dog.
(c) Enlarged gall bladder and cystic duct in a dog with extrahepatic bile duct obstruction.
(d) Pancreatitis in a dog that caused obstruction of the bile duct at the duodenal papilla resulting in cholestasis and icterus.
(e) Intraluminal bile concrements obstructing the bile duct in a dog with chronic cholecystitis and choleliths.
(f) Cystic dilation of the intrahepatic bile ducts in a cat with chronic cholestasis due to obstruction of the extrahepatic bile duct.
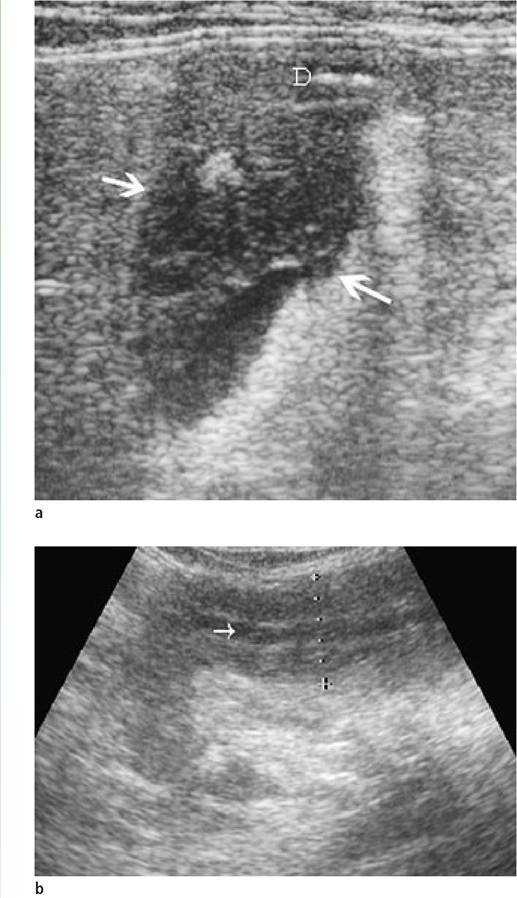
Figure 1.40a, b:
Acute pancreatitis in a cat.
(a) The right pancreatic limb is enlarged (arrows) and very hypoechoic. The surrounding mesenterium is hyperechoic, which is a sign of peripancreatic fat necrosis. D = duodenum.
(b) The left pancreatic limb in the same cat was smaller but hypoechoic. The pancreatic duct (arrow) is mildly dilated.
1.3.8