Local Muscle Strain
Stephanie J. Valberg
Lumbar and Gluteal Muscles
Strain of lumbar and gluteal muscles is common in jumpers, dressage, harness horses, and Thoroughbreds. Deep palpation of epaxial and gluteal muscles results in pain and dorsiflexion of the spine.
Several factors may predispose horses to muscle strains, such as an inadequate warm-up, preexisting lameness, exercise to the point of fatigue, and insufficient training. Lameness can be mild, and horses usually are reluctant to engage their hindquarters during exercise. A specific gluteal syndrome has been described in which the accessory head of the middle gluteal muscle becomes acutely painful to palpa- tion.178 With accessory gluteal head involvement horses become progressively more lame during exercise and will refuse to continue exercise. Horses that show pain but resist dorsiflexion, ventroflexion, and lateral bending on manipulation may have a myopathy secondary to an underlying disorder of the spine or sacroiliac joint.Adductor Muscles
The gracilis muscle can be torn in horses and cause severe pain and, occasionally, recumbency.179,180 A careful physical examination reveals swelling of the medial thigh and pain on palpation. Ultrasonography identifies the extent of disrupted muscle fibers. Adequate rest, NSAIDs, and cold therapy form the basis for acute treatment. Stretches and hand walking once the initial pain has dissipated are beneficial combined with application of heat or ultrasound therapy. Exercise should be resumed gradually, preceded by an appropriate warm-up period in a long and low frame. Adequate conditioning should be ensured before starting strenuous exercise. Saddles should be checked for proper fit.
Semitendinosus and Semimembranosus Muscles
Semitendinosus and semimembranosus muscles are frequently damaged in working Quarter Horses, and in chronic cases this can result in a fibrotic myopathy.181-183 Tearing of the semitendi- nosus and sometimes the semimembranosus, biceps femoris, and gracilis muscles at the point of a tendinous insertion is usually associated with work that requires abrupt turns and sliding stops.
Horses caught in ropes or fences may struggle violently enough to induce sufficient trauma, allowing subsequent development of the myopathy. In one report, 5 of 18 horses developed this condition secondary to intramuscular injections.183Affected muscles in acute cases are painful on deep palpation and may appear warm. Chronically hardened areas within the muscle may represent fibrosis and ossification. The lameness in chronic cases is usually most apparent at the walk and is characterized by an abrupt cessation of the anterior phase of the stride of the affected limb, causing the leg to jerk suddenly to the ground rather than continue its forward motion. Pain is not a feature in chronic fibrotic myopathy, and manipulative tests have little, if any, effect on the degree of dysfunction. The stride has a short anterior phase with a characteristic hoof-slapping gait. The gait reflects a mechanical hindlimb lameness that restricts normal function. Radiographs may indicate ossification of affected muscles.183
■ Diagnosis Serum activities of CK and AST are usually only mildly elevated. In addition to palpation, diagnosis can be confirmed by ultrasonography, thermography, or scintigraphy. Light microscopic evaluation of muscle biopsies is frequently normal in acute cases. Chronically fibrous replacement of muscle fibers is apparent.
■ Treatment Several surgical procedures for correction of fibrotic myopathy have been described.169,183
Exertional Rhabdomyolysis
Stephanie J. Valberg
Exertional rhabdomyolysis (ER) is probably the most common muscle disorder in horses. It is a frequent cause of poor performance in a variety of breeds, including Standardbreds, Thoroughbreds, warmbloods, Arabians, Morgans, Quarter Horses, Appaloosas, and Paints. ER is a complex syndrome that likely has numerous causes. Numerous terms such as tying-up, chronic intermittent rhabdomyolysis, azoturia, Monday morning disease, paralytic myoglobinuria, and exercise- associated myositis have been used for this syndrome.
■ Clinical Signs Classically, horses develop a stiff, stilted gait, with excessive sweating and a high respiratory rate during or after exercise (Fig. 42.17). Most commonly, signs are seen after only 15 to 30 minutes of light exercise. Following exercise, horses may stretch out as if to urinate, become extremely reluctant to move their hindquarters, and in severe cases show signs of colic or become recumbent. Attempts to move more severely affected animals may result in extreme pain, obvious anxiety, and possible exacerbation of the condition. Firm, painful muscles may be palpated over the back and hindlimb muscles. Scintigraphic evaluation of horses with rhabdomyolysis following exercise shows symmetric damage to the gluteal, semitendinosus, and semimembranosus muscles.15 Myoglobinuria is a classic feature of more severely affected horses. Endurance horses often show other signs of exhaustion, including a rapid heart rate, dehydration, hyperthermia, synchronous diaphragmatic flutter, and collapse.71
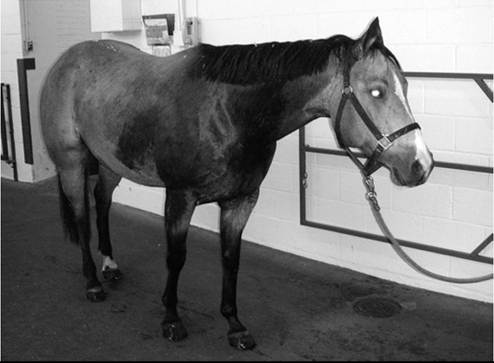
FIG. 42.17 Exertional rhabdomyolysis in a horse showing signs of pain, stiffness, sweating, and elevated respiratory rate.
■ Etiology A number of factors appear to precipitate episodes of ER. Some successful athletic horses may experience one or two isolated episodes of rhabdomyolysis during their lifetime, suggesting that environmental influences play an important role in sporadic cases.184-188 Other horses may have chronic episodes of rhabdomyolysis that compromise their ability to compete. An inherent muscle dysfunction precipitated by certain triggering factors likely contributes to rhabdomyolysis in these horses.7,189,190 Thus ER is a description of a syndrome that has many causes. To identify the cause in individual horses, it may be helpful to initially subdivide cases into those with no intrinsic muscle abnormality (extrinsic or sporadic form) and those with a suspected intrinsic abnormality of muscle function (intrinsic or chronic form).
Causes for sporadic and chronic exercise-induced muscle damage are listed in Box 42.2.Sporadic Exertional Rhabdomyolysis
Most cases of ER can be diagnosed on the basis of the animal's history and clinical signs. Confirmation of rhabdomyolysis requires determination of abnormally elevated serum CK and/ or AST. Serum CK is often in the tens to hundreds of thousands of IU/L and AST in the thousands to tens of thousands. The degree of elevation in enzymes reflects the time lapse between rhabdomyolysis and obtaining a blood sample, as well as the extent of myonecrosis. Myoglobinuria is a common finding in severely affected horses. Horses with sporadic forms of ER develop rhabdomyolysis because of an extrinsic event or recurring extrinsic events that induce muscle damage with exercise. Usually a horse is presumed to have sporadic ER the first time it develops ER.14 If ER recurs once the horse has been rested and gradually returned to exercise, an investigation of an inherent chronic form of ER is usually pursued. Causes of sporadic ER include focal or generalized trauma to muscle, exercise performed beyond any training adaptation or performed to the point of exhaustion, and dietary imbalances that affect muscle function.
■ Signalment, History, and Diagnosis Horses with sporadic ER may be of any age, breed, or sex and involved in a wide variety of athletic disciplines.184 Sporadic ER usually occurs in horses with a history of adequate performance before onset of ER, and a familial history is absent. A diagnosis is made by history, clinical signs, and elevations of serum muscle enzymes. Once external perturbations that affect muscle function are corrected, complete resolution and a successful return to performance are expected. Resolution occurs following a reasonable period of rest, provision of a balanced diet, and a gradual introduction of a training program matched with performance demands. If over time ER recurs despite reasonable management, a diagnosis of chronic ER becomes more likely and further diagnostic testing is appropriate.
■ Causes
OVEREXERTION. A history of an increase in work intensity without a foundation of consistent training for this level of exercise is usually the basis for suspecting a training imbalance as a cause of ER. Signs of muscle stiffness and gait changes range from mild to severe, and severity is reflected by variable elevations of serum CK activity.14 Overexertion is a well- described cause of ER in polo horses, with 81% of cases of ER attributed to overexertion and 30% of cases occurring after a day of rest.188 The incidence of ER is as high as 9% in the United States polo horses, with most of these horses having only one episode of ER early in the polo season.188
Pathologic changes are often not evident in light microscopic evaluation of muscle biopsies from individuals performing unaccustomed exercise, but electron microscopy shows significant disruption of the alignment of muscle contractile proteins within muscle fibers. In more severe cases, overt segmental damage to myofibers may be apparent in muscle biopsy. Repetitive overuse of muscles, such as occurs with overtraining, may result in exercise intolerance and is associated with pathologic changes such as increased muscle fiber size variation and centrally located myonuclei in muscle biopsies.191
EXHAUSTION. Exhaustion occurs most commonly in endurance horses or racehorses exercising in hot, humid weather. Signs of heat exhaustion include weakness, ataxia, rapid breathing, muscle fasciculations, sweating, and in severe cases collapse. The body temperature may be elevated to 105° to 108° F. Muscles are frequently not firm on palpation, although serum CK activity can be markedly elevated and myoglobinuria may be noted.71
DIETARY IMBALANCES. Episodes of ER may be triggered by diets with a high nonstructural carbohydrate (NSC) content and low forage content,192,193 as well as by diets deficient in electrolytes. They may be exacerbated by inadequate selenium and vitamin E.
Electrolyte balance within the body is difficult to determine accurately. One suggested means to practically assess electrolyte balance in horses is to measure urinary fractional excretion of electrolytes.194 Measurement of urinary electrolyte excretion as an indicator of electrolyte balance is complicated because marked variation can occur from diet, exercise, and sampling technique among individuals, as well as within individuals from day to day.4 Furthermore, the high calcium crystal concentration of alkaline equine urine requires acidification to accurately assess calcium and magnesium content.4 The high potassium content interferes with sodium analysis using conventional ion-specific electrodes.7 Thus although popular in the 1990s,3,194,195 urinary fractional excretion is now rarely performed in the United States unless there is a strong suspicion that body depletion has occurred and a laboratory with gas chromatography mass spectrometry analysis of acidified urine can be located. It is important to ensure that horses receive sodium chloride in the diet, with higher concentrations needed in horses that compete in hot, humid weather. Between 30 and 50 g/day combined with 15 to 25 g of “lite” salt containing potassium chloride is recommended for horses exercising in hot, humid conditions and sweating extensively. The entire diet should be adequately balanced with calcium and phosphorus (Ca/P ratio of 2:1 is ideal).Whole blood selenium concentrations measured in ethylenediaminetetraacetic acid (EDTA) or heparin tubes are of value in assessing selenium status in animals housed in areas where soil is deficient in selenium. In cases where selenium has been administered before blood collection, glutathione peroxidase activity can be used to assess potential selenium deficiency.196 Vitamin E concentration should be measured in serum samples kept chilled and protected from light; however, variability in serum levels can be quite large, and repeat sampling is recommended if marginal levels are identified in the first sample tested. Horses with ER are infrequently deficient in selenium and vitamin E, and alone it may not be responsible for ER197; however, anecdotal reports suggest that in some cases supplementation may help to further prevent episodes of ER.
■ Treatment Treatment of ER is directed at relieving anxiety and muscle pain and replacing fluid and electrolyte losses. Tranquilizers such as acepromazine (0.04 to 0.06 mg/ kg IM or IV), xylazine (0.5-1.1 mg/kg IV), or detomidine (0.02 to 0.04 mg/kg IV) combined with butorphanol (0.01 to 0.04 mg/ kg) provide excellent sedation and analgesia. For horses with extreme pain and distress, a constant rate infusion of detomidine, lidocaine, or butorphanol may provide additional pain relief. NSAIDs such as ketoprofen (2.2 mg/kg IV), phenylbutazone (2.2 to 4.4 mg/kg IV or PO), and flunixin meglumine (1.1 mg/ kg IV or PO) are frequently used to relieve pain but should be used with caution on dehydrated animals. Intravenous or intragastric dimethyl sulfoxide (as a be adequate. Horses with moderate to severe dehydration require IV administration of balanced polyionic electrolyte solutions. Hyperkalemia can occur with severe rhabdomyolysis, necessitating the use of isotonic sodium chloride. If hypocalcemia is present, then supplementing IV fluids (100 to 200 mL of 23% calcium borogluconate) is recommended, but serum calcium should not exceed a low normal range. Affected animals are usually alkalotic, making bicarbonate therapy inappropriate. In severely affected animals, regular monitoring of serum creatinine is advised to assess the extent of renal damage.
Following rhabdomyolysis, horses should be stall rested on a hay diet for a few days. Small paddock turnout in a quiet area for a few hours twice a day is then helpful. Horses may be hand walked at this time, but more than 5 to 10 minutes at a time may induce another episode of rhabdomyolysis. For horses with sporadic forms of tying-up, rest with regular access to a paddock should continue until serum muscle enzyme concentrations are normal. For chronic cases of tying-up, this much rest may not be appropriate. Training should be resumed gradually, and a regular exercise schedule that matches the degree of exertion to the horse's underlying state of training should be established. Endurance horses should be supplemented with electrolytes and water during an endurance ride and monitored particularly closely during hot, humid conditions.
■ Management Because the inciting cause is usually temporary in sporadic cases, most horses respond to a few weeks of rest, dietary adjustments, and a gradual increase in training. Regular access to a paddock once stiffness subsides and weekly monitoring of serum CK activity are recommended. Horses are much more susceptible to a second episode of ER in the 2 weeks following an acute episode, and allowing horses the ability to calmly determine their own exercise through turnout often avoids exacerbating rhabdomyolysis. If that is not feasible, hand walking needs to performed with caution and limited to no more than a few minutes initially. While the horse is rested, the diet can be assessed to ensure that the ration is fed in an amount recommended by the manufacturer for the corresponding level of exercise. This will ensure that the proper balance of vitamins and minerals is provided. If excessive calories are provided when fed at the manufacturer's recommended levels, the diet should be switched to a less calorie-dense vitamin/mineral balanced diet. A salt block or 30 to 50 g (1 to 3 tablespoons) of salt per day will provide the necessary additional sodium chloride, with the amount fed depending on the heat, humidity, and intensity of exercise. Once serum CK returns to normal, training can be resumed gradually. A regular exercise schedule, beginning with 20 minutes or less of exercise per day, is gradually increased to eventually match the expected amount of daily exercise to the underlying state of conditioning.
Chronic Exertional Rhabdomyolysis
Horses that have repeated episodes of ER from a young age, from the time of purchase, or after they are put back into training after a long period of rest may have an underlying intrinsic abnormality of muscle function. Many horses with intrinsic muscle defects will have repeated episodes of ER with minimal exercise even when the dietary and training recommendations for sporadic ER are followed. Five specific intrinsic causes of ER have been identified to date (see Box 42.2). Idiopathic ER represents other causes of ER that have yet to be identified. In all of these intrinsic forms of chronic ER, it appears that specific environmental stimuli are necessary to trigger muscle necrosis in genetically susceptible animals. Horses cannot be cured of their susceptibility to this condition, but if the specific form of ER is identified, changes in management can be implemented in order to minimize episodes of rhabdomyolysis.
Polysaccharide Storage Myopathy
Polysaccharide storage myopathy (PSSM) was first recognized as a specific myopathy in Quarter Horse-related breeds in 1992198; however, there are individual cases of abnormal polysaccharide inclusion reported in equine muscle dating back to 197 9.17,199,200 The remarkable feature of the first horses reported to have PSSM was twofold-higher muscle glycogen concentrations than normal horses and abnormal granular amylase-resistant inclusions in histologic sections.198 Similar biopsy findings were reported in Belgian and Percheron draft horses in 1997.201 Since that time, many hundreds of horses of a variety of breeds have been diagnosed with PSSM.
■ Terminology Several acronyms are used for polysaccharide storage myopathy besides PSSM,202 including EPSM or EPSSM (equine polysaccharide storage myopathy).192,203 Considerable controversy existed as to whether these acronyms encompassed one muscle condition.192,193,204 In 2008 a mutation in the glycogen synthase 1 (GYSl) gene was found to be highly associated with the presence of amylase-resistant polysaccharide in skeletal muscle from Quarter Horses with PSSM.205 Genetic testing of hundreds of horses previously diagnosed with PSSM by muscle biopsy revealed that the majority of cases of PSSM characterized by amylase-resistant polysaccharide in skeletal muscle had this genetic mutation.206 However, some cases previously diagnosed with PSSM by muscle biopsy, particularly those with excessive amylase-sensitive glycogen, did not possess the genetic mutation. This suggested that there are at least two forms of PSSM.206,207 For clarity, the form of PSSM caused by a GYSl gene mutation is now called type 1 (PSSMl), whereas the form of PSSM not caused by the GYSl mutation and whose origin is yet unknown is now called type 2 (PSSM2).207 PSSM1 is likely the same disorder described as “azoturia” or “Monday morning disease” in workhorses in the nineteenth and twentieth centuries.208
Type 1 Polysaccharide Storage Myopathy
ETIOLOGY. PSSM1 is caused by a single-base-pair mutation in the GYSl gene resulting in an arginine to histidine substitution at codon 309. Horses with PSSM1 have a gain of function in glycogen synthase enzyme (in basal and stimulated states) because of an autosomal dominant mutation in the GYSl gene encoding glycogen synthase.205 The higher than normal activity in both basal states and when activated by insulin and glucose 6-phosphate appears to have a novel link to the regulation of energy generation in muscle fibers. A deficit in energy metabolism represented by high myofiber inosine monophosphate was demonstrated in individual muscle fibers of horses with PSSM1 after light exercise in association with high serum CK activity.209
■ TABLE 42.3
Number of North American and European Horses Tested and the Percentage of Horses Testing
Positive (Heterozygous and Homozygous) for the GYS1 Mutation in Breeds Sampled Using Random and Nonrandom Sampling
| Random Sampling | Breed | Number Tested | Prevalence (%) |
| North America | Percheron | 149 | 62 |
| (McCue and colleagues, 2010)211 | Belgian | 149 | 39 |
| Clydesdalea | 132 | 0 | |
| Shire | 195 | 0.5 | |
| Quarter Horse | 335 | 6.6 | |
| Paint | 195 | 7.7 | |
| Appaloosa | 152 | 5.9 | |
| Morgan | 214 | 0.9 | |
| Thoroughbred | 96 | 0 | |
| Arabian | 100 | 0 | |
| Norwegian Fjord | 46 | 0 | |
| Icelandic Pony | 45 | 0 | |
| Nonrandom Sampling | Breed | Number Tested | Prevalence (%) |
| Europe | Belgian Trekpaard | 38 | 92 |
| (Baird and colleagues, 2010)210 | Netherlands Trekpaard | 23 | 74 |
| Comtois | 88 | 80 | |
| Breton | 51 | 63 | |
| Swedish Ardenner | 29 | 38 | |
| Rheinisch-Deutsches Kaltblut | 44 | 68 | |
| Sud-Deutsches Kaltblut | 265 | 20 | |
| Hannoverian | 214 | 0 | |
| (Isgren and colleagues, 2010)215 | Standardbred | 36 | 0 |
aBoth randomized and nonrandomized samples.
■ Prevalence PSSM1 is estimated to have emerged approximately 1600 years ago when the great horse was being developed from European draft and light horse breeds to carry knights with heavy armor into battle.205 The highest prevalence of PSSM1 appears to occur in draft horses derived from Continental European breeds (Table 42.3).210 In fact, many Continental European drafts are homozygous for the dominant PSSM1 trait (90% prevalence of PSSM in Trekpaards, with 40% of tested Belgian Trekpaards homozygous). North American Belgians and Percherons also have a high prevalence of PSSM1, with 36% and 54% of horses affected, respectively.211 In contrast, the prevalence of PSSM is low in United Kingdom-derived breeds such as Shires and Clydesdales,211 but PSSM1 is present in other U.K. horse breeds such as Irish Draught, Cob, and Connemara.212 Numerous other breeds, more than 20 in fact, have the GYS1 mutation responsible for PSSM1.
Prevalence estimates of PSSM1 in Quarter Horses range from 6% to 10% of the breed and 6% to 8% for Paints and Appaloosas.56,213 The highest frequency of PSSM1 occurs in halter Quarter Horses (28% affected), and the lowest frequency occurs in racing Quarter Horses.56 The GYS1 mutation has been identified in approximately 72% of Quarter Horses diagnosed with PSSM by muscle biopsy and in 18% of warmbloods of a variety of types diagnosed with PSSM by muscle biopsy.214 The prevalence of PSSM1 is very low to nonexistent in light horse breeds such as Arabians, Standardbreds, and Thoroughbreds (see Table 42.3).215
■ Risk Factors Some horses with PSSM1 are asymptomatic, whereas other horses routinely show stiffness with exercise.216,217 In a family of warmbloods sired by a stallion with the GYS1 mutation, the mutation resulted in a sevenfold-higher risk of developing ER, with 34% of horses with the GYS1 mutation lacking clinical signs of PSSM1.217 The reason for variability in clinical signs of PSSM1 probably lies in the influence of diet, exercise, other environmental factors, and other genes on the expression of the disease.192,218,219 There is no significant temperament, body type, or gender predilection for PSSM1.8 The most common trigger for clinical signs of PSSM1 is less than 20 minutes of exercise at one time.189,217 Clinical signs occur most commonly at a walk and trot, particularly if the horse has been rested for several days before exercise or is unfit. Diets high in NSCs also increase the risk of muscle pain and stiffness in PSSM1 horses.218,220 About 40% of owners feel there is a seasonal incidence to the development of clinical signs, which some have attributed to quality of grass available at the time.189,221 Although exercise is by far the most common trigger for PSSM, Quarter Horse and Paint foals and weanlings may develop rhabdomyolysis in conjunction with a systemic illness.222
■ Diagnosis A high degree of suspicion of a diagnosis of PSSM1 arises from clinical signs and persistent elevations in serum CK and AST activities.8,198,218 If horses have normal serum muscle enzymes at rest, an exercise test consisting of a maximum of 15 minutes lunging at a walk and trot may help to determine if subclinical ER is present.7 Supportive evidence would include a minimum of a threefold elevation in CK activity 4 hours after exercise.
Muscle biopsy provides one means to diagnose PSSM1.18,198,223 The distinctive features of PSSM1 in muscle biopsy samples are numerous subsarcolemmal vacuoles and dense, crystalline periodic acid-Schiff (PAS)-positive, amylase-resistant inclusions (Fig. 42.18, A and B). A diagnosis can be made irrespective of diet and proximity of sampling to recent episodes of rhabdomyolysis. A false-negative diagnosis of PSSM1 by muscle biopsy may occur if biopsy samples are small or if horses are younger than 1 year of age.224
The gold standard for diagnosis of PSSM1 is genetic testing for the GYS1 mutation performed on whole blood or hair root samples. It is important to note that in draft horses of
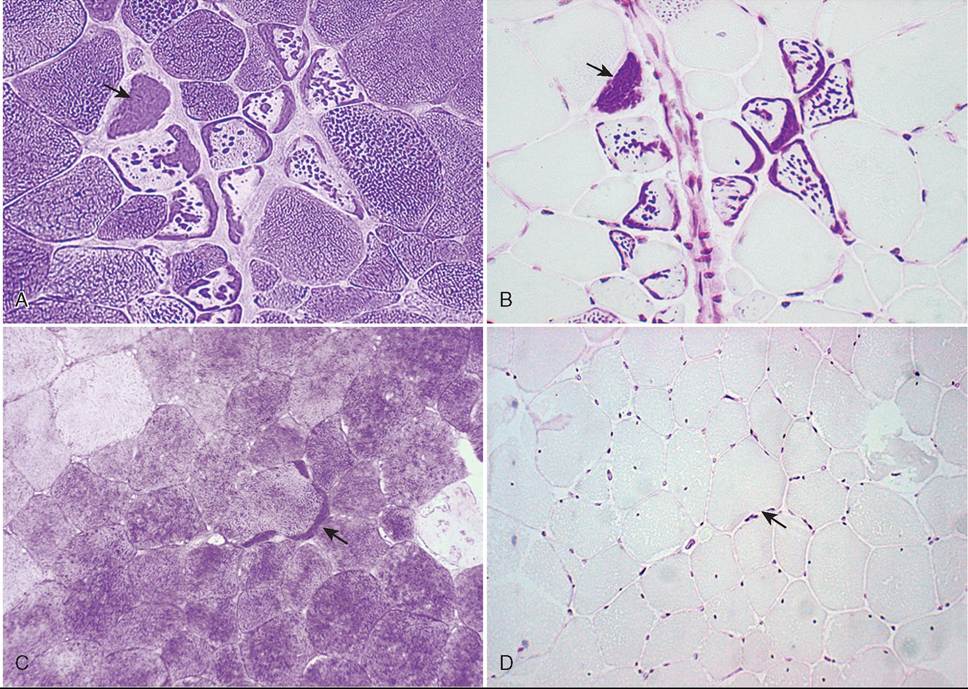
FIG. 42.18 Consecutive sections of a gluteal biopsy from a horse with type 1 polysaccharide storage myopathy (PSSM) stained with (A) periodic acid- Schiff (PAS) stain for glycogen and (B) amylase-PAS stain. Arrows show typical aggregates of intensely staining polysaccharide, which are resistant to amylase digestion. (C) PAS stain and (D) amylase-PAS stain of a gluteal biopsy from a horse with type 2 PSSM. Arrows show an aggregate of polysaccharide under the sarcolemma, which is sensitive to amylase digestion.
Continental European origin, the very high prevalence of PSSM in essence means that there is a high chance that any clinical sign could be falsely associated with the disease PSSM1.210 Thus clinical judgment is required to determine whether the clinical signs of the animal could reasonably be associated with a myopathic process.
■ Clinical Signs
ACUTE. On average, horses show signs of PSSM1 at 5 years of age; however, this can range from 1 to 14 years of age.189 Acute clinical signs occur when horses are calm and include tucking up of the abdomen, fasciculations in the flank, muscle stiffness, sweating, reluctance to move forward, and overt firm muscle contractures (Fig. 42.19).189 The hindquarters are frequently affected, but back, abdomen, and forelimb muscles may also be involved. Signs of pain can last for more than 2 hours, and about 10% of cases become recumbent.189 Less common signs of PSSM in Quarter Horses include gait abnormalities, mild colic, and muscle wasting. During an acute episode of ER, horses with PSSM1 often have markedly elevated serum CK activity of greater than 35,000 U/L, and myoglobinuria may be present. Severe colic-like pain post exercise and myoglobinuric renal failure are less common presenting complaints.8,225
CHRONIC
Light Breeds. Chronic signs of PSSM1 in riding horses include a lack of energy when under saddle, reluctance to
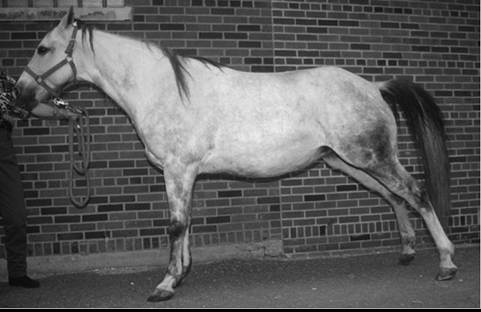
FIG. 42.19 Typical stance of a horse with polysaccharide storage myopathy after 10 minutes of walking and trotting. Note the tucked-up abdomen and camped-out stance that were concurrent with firm muscles, fasciculations in the flank, and elevated serum CK activity.
move forward, stopping and stretching out as if to urinate (see Fig. 42.19), and a sour attitude toward exercise.189 Horses may have a combination of low-grade reluctance to exercise, poor performance, and repeated episodes of ER.217,226 PSSM1 may also present in dressage and showjumpers as chronic back pain, failure to round over fences, and fasciculations or pain on palpation of lumbar muscles.227’228 The range of severity of clinical signs of PSSM1 can be wide, with complete incapacitation in rare cases. Serum CK activities are often elevated in unmanaged horses, even when horses are rested.8 The median CK and AST activities for all PSSM1 Quarter Horses with muscle biopsies submitted to the Equine Neuromuscular Diagnostic Laboratory were 2809 and 1792 U/L, respectively.
A small number of Quarter Horses and Paints have both the GYSl mutation and the genetic mutation for malignant hyperthermia (RYRl).219 This results in particularly severe signs of ER and a limited response to diet and exercise changes. During an episode of ER, excessively high body temperatures may develop, and sudden death can occur in horses with the RYR1 mutation. This combination occurs most often in halter and pleasure horses.
Draft Horse and Draft Crosses. The average age of draft horses diagnosed with PSSM is about 8 years of age. Many draft horses with PSSM are asymptomatic.216 Signs of severe rhabdomyolysis and myoglobinuria may occur in horses that are fed high-grain diets, exercised irregularly with little turnout, or put under general anesthesia.175’189 Rhabdomyolysis can be so severe that it leads to recumbency and death.175 Other signs of PSSM in draft horses include progressive weakness and muscle loss resulting in difficulty rising in horses with normal serum CK activity. Clinical signs appear to be more severe in homozygotes.229 Although the condition shivers was previously attributed to PSSM, a recent study found no causal association between these two conditions.216 The median serum CK and AST activities in draft horses from which biopsies were sent to the Equine Neuromuscular Diagnostic Laboratory were 459 and 537 U/L, respectively.
■ Pathophysiology A high-NSC diet increases the propensity to develop muscle pain with aerobic exercise in PSSM1 horses.192,218 A potential scenario in PSSM1 horses on high-NSC diets could be that nutrient switches do not fully activate enzymes such as pyruvate dehydrogenase during exercise, limiting adequate acetyl-CoA for oxidative metabolism. Although acetyl-CoA could also be supplied by fatty acid oxidation, PSSM horses on high-NSC diets have low plasma nonesterified free fatty acid concentrations, possibly due to suppression of lipolysis by high insulin.218 A further factor reducing fatty acid oxidation in PSSM horses on high-NSC diets could be that high muscle citrate concentrations direct acetyl-CoA away from the citric acid cycle toward malonyl-CoA, the committed step for fatty acid synthesis.230 In addition, accumulation of malonyl-CoA causes inhibition of carnitine palmitoyltransferase, the key enzyme necessary to transport long-chain fatty acids into the mitochondria for β-oxidation.231,232 Thus PSSM horses fed high-NSC diets may be unable to generate sufficient acetyl-CoA from either carbohydrate or fat metabolism to fuel muscle contraction during submaximal exercise. The common occurrence of clinical signs during the first 20 minutes of exercise may be because, at this stage of exercise, muscles rely heavily on glycogen and glucose for energy. Low dietary starch and fat supplementation decrease muscle citrate concentrations and increase plasma free fatty acid concentrations, which may well facilitate muscle fat metabolism in PSSM1 horses.233
TYPE 2 POLYSACCHARIDE STORAGE MYOPATHY. Much less is known about type 2 PSSM because, as it turns out, previous research on PSSM has largely involved horses with type 1 PSSM. Current knowledge of type 2 PSSM is based on retrospective evaluation of cases diagnosed with PSSM by muscle biopsy that are now known to be free of the GYSl mutation and on a few years of prospective clinical cases.223,227
■ Prevalence Approximately 28% of cases of PSSM diagnosed by muscle biopsy in Quarter Horses have PSSM2 because they do not have the GYS1 mutation.206 Type 2 PSSM seems to be common both in high-performance Quarter Horse types such as barrel racing, reining, and cutting horses and in pleasure and halter horses. In the United Kingdom approximately 35% of PSSM cases diagnosed by muscle biopsy have PSSM2.212 Type 2 PSSM also occurs in Paints, Appaloosas, and Morgans. About 80% of cases of PSSM diagnosed by biopsy in warmbloods have PSSM2.206 Breeds affected include Dutch Warmblood (highest prevalence), Swedish Warmblood, Selle Franyais, Hanoverian, Friesian, Westphalian, Canadian Warmblood, Irish Sport Horse, Gelderlander, and Icelandic horses. Many other light breeds have also been diagnosed with PSSM2, including Standardbreds, Thoroughbreds, and Arabians.
■ Pathogenesis The cause or causes of PSSM2 are currently unknown. Muscle glycogen concentrations are not as high as those found in PSSM1, and glycogenolytic enzyme defects have not been identified in the few cases where enzymes were measured.223 To date, the only reported abnormality in muscle ultrastructure is an increase in normal beta glycogen particles.207 It may well be that a group of conditions currently captured under the term type 2 PSSM have separate etiologies but share common findings of glycogen accumulation and poor performance. A heritable predisposition is suspected in Quarter Horses but yet to be proven.
■ Clinical Signs
ACUTE. In Quarter Horses, Thoroughbreds, Standardbreds, and Arabian horses, exertional rhabdomyolysis is the most common clinical sign of PSSM2.223 In warmblood horses, episodes of exertional rhabdomyolysis are more intermittent in nature.223
CHRONIC. Chronic signs of PSSM2 are often most closely related to poor performance rather than recurrent ER and elevations in serum CK activity. An undiagnosed gait abnormality, sore muscles, and drop in energy level and willingness to perform after 5 to 10 minutes of exercise are common complaints in horses with PSSM2.223 Warmbloods with PSSM2 may also have painful, firm back and hindquarter muscles, reluctance to collect and engage the hindquarters, poor rounding over fences, gait abnormalities, and slow onset of atrophy. The mean age of onset of clinical signs in warmbloods is between 8 and 11 years of age, with the median CK and AST activities being 323 and 331 U/L, respectively.
■ Diagnosis PSSM2 must be diagnosed by muscle biopsy where increased or abnormal PAS-positive material that is usually amylase sensitive is apparent (see Fig. 42.18, C and D).207 Determination of what constitutes an abnormal amount of amylase-sensitive glycogen is subjective, the specificity of the diagnosis may be low, and false-positive diagnoses may occur. Consideration should be made for state of training because highly trained horses have increased glycogen storages as a normal response to training. Further, glycogen is commonly found near capillaries in normal horses, and PAS-positive sarcoplasmic masses can be found in 60% of healthy horses, so these should not be diagnostic criteria for PSSM2.234 Formalin- fixed sections show a greater deposition of subsarcolemmal glycogen and precipitation of glycogen in one area of a fiber even in healthy horses, and these should not be considered diagnostic criteria for PSSM2.18 Other histopathologic features that may be present with PSSM2 include centrally located nuclei, subsarcolemmal vacuoles, muscle necrosis, macrophage infiltration of myofibers, regenerative fibers, and fiber atrophy.223 Some laboratories grade polysaccharide accumulation as mild, moderate, and severe, where mild accumulation represents a category that has a higher chance of being a false-positive diagnosis. Mild PSSM cases in particular should receive a full physical examination to ensure that there are no other underlying causes for performance problems.
MANAGEMENT OF TYPE 1 AND TYPE 2 POLYSACCHARIDE STORAGE MYOPATHY. Owners need to be aware that any horse diagnosed with PSSM will always have an underlying predilection for muscle soreness. The best that can be done is to manage horses in the most appropriate fashion to minimize clinical signs. With adherence to both diet and exercise recommendations provided in this chapter, at least 70% of horses show notable improvement in clinical signs and many return to acceptable levels of performance.189,192,227 There is, however, a wide range in the severity of clinical signs shown by horses with PSSM; those horses with severe or recurrent clinical signs will require more stringent adherence to diet and exercise recommendations in order to regain muscle function.
REST. PSSM horses that are confined for days to weeks following an episode of rhabdomyolysis often have persistently elevated serum CK activity.224 In contrast, PSSM horses kept on pasture with little grain supplementation often show few clinical signs of rhabdomyolysis and have normal serum CK activity.224 As a result, a common recommendation for horses with PSSM is to limit stall confinement to less than 48 hours after an episode of rhabdomyolysis and then provide turnout in paddocks of gradually increasing size. Providing horses with as much free exercise as possible on pasture appears to be beneficial in the long term. If pasture is lush, a grazing muzzle may be necessary.226 Following an acute episode, excitable horses may require tranquilization before turnout to avoid excessive galloping. Hand walking horses initially recovering from an episode of PSSM for more than 5 to 10 minutes at a time may trigger another episode of rhabdomyolysis.
EXERCISE. The beneficial response to low-starch, fat- supplemented diets only occurs if it is instituted in conjunction with a regular incremental exercise program.218 Regular daily exercise in PSSM horses over a 3-week period has been shown to produce a dramatic decrease in serum CK responses to exercise, whereas stall confinement often causes elevations in serum CK activity post exercise.218,224 One common adaptation to daily training is an increase in oxidative capacity in skeletal muscle. The activity of these enzymes, however, was equally low in control Quarter Horses. Whether the beneficial effect of daily exercise on PSSM horses is a result of improved oxidative enzyme capacities or enhanced substrate flux or both has not been elucidated.
EXERCISE REGIMENS. Important principles to follow when starting exercise programs in PSSM horses include to (1) provide adequate time for adaptation to a new diet before commencing exercise; (2) recognize that the duration of exercise, not its intensity, is of primary importance; (3) ensure the program is gradually introduced and consistently performed; and (4) minimize any days without some form of exercise. If horses have experienced a moderate to marked episode of rhabdomyolysis recently, 2 weeks of turnout and diet change are often beneficial before recommencing exercise. Exercise should be relaxed, and the horse should achieve a long, low frame without collection. For many horses this is most readily done in a round pen or on a lunge line, but it can be done under saddle if needed. Successive daily addition of 2-minute intervals of walk and trot beginning with only 4 minutes of exercise and working up to 30 minutes after 3 weeks is often recommended.8,14 If horses had minor elevations in 4-hour postexercise CK with the 15-minute exercise test, they may begin at 15 minutes of exercise. Owners often do not recognize that walking the horse for 10 minutes or more initially can trigger muscle soreness in PSSM horses. Advancing the horse too quickly often results in an episode of rhabdomyolysis and repeated frustration for the owner. Work can usually begin under saddle after 3 weeks of ground work and can gradually be increased by adding 2-minute intervals of collection or canter to the initial relaxed warm-up period at a walk and trot. Unless a horse shows an episode of overt rhabdomyolysis during the initial 4 weeks of exercise, reevaluating serum CK activity is not helpful for the first month. This is because it is common to have subclinical elevations in CK activity when exercise is reintroduced, and a return to normal levels often requires 4 to 6 weeks of gradual exercise.8 Keeping horses with PSSM fit seems the best prevention against further episodes of rhabdomyolysis.
DIETS FOR POLYSACCHARIDE STORAGE MYOPATHY. The basis for designing PSSM diets is the belief that lowering the daily starch and sugar intake and increasing dietary fat content will decrease the glucose load, increase the availability of nonesterified fatty acid for muscle metabolism, and lower serum insulin concentrations.218 Quarter Horses naturally have little lipid stored within muscle fibers. The end result would thus be decreased uptake of glucose into muscle cells, less substrate available for—and stimulation of—glycogen synthesis, and normalization of substrate flux. Owners report that this type of diet improves clinical signs of muscle pain, stiffness, and exercise tolerance in draft horses, warmbloods, Quarter Horses, and other breeds.189,192,217,227 Dietary change appears to have less impact on alleviating gait changes such as shivers.227
CALORIC BALANCE. The horse's caloric requirements at an ideal body weight are the most important considerations in designing the diet for PSSM. This is because many horses with PSSM are easy keepers and may be overweight at the time of diagnosis. Adding excessive calories in the form of fat to an obese horse may produce metabolic syndrome and is contraindicated. If necessary, caloric intake should be reduced by using a grazing muzzle during turnout, feeding hay with a low NSC content at 1% to 1.5% of body weight, providing a low-calorie ration balancer, and gradually introducing daily exercise. Rather than provide dietary fat to an overweight horse, fasting for 6 hours before exercise can be used to elevate plasma free fatty acids before exercise and alleviate any restrictions in energy metabolism in muscle.
SELECTION OF FORAGE. Quarter Horses have been shown to develop a significant increase in serum insulin concentrations in response to consuming hay with an NSC of 17%, whereas insulin concentrations are fairly stable when fed hay with 12% or 4% NSC content.220 Because insulin stimulates the already overactive enzyme glycogen synthase in the muscle of PSSM1 horses, selecting hay with 12% or less NSC is advisable. The degree to which the NSC content of hay should be restricted below 12% NSC depends on the caloric requirements of the horse. Feeding a low-NSC hay of 4% provides room to add an adequate amount of fat to the diet of easy keepers without exceeding the daily caloric requirement and inducing excessive weight gain. For example, a 500-kg horse on a routine of light exercise generally requires 18 Mcal/day of digestible energy (DE). Fed at 2% of body weight, a 12% NSC mixed grass hay almost meets the daily caloric requirement by providing 17.4 Mcal/day. Thus with a 12% NSC hay there is only room for 0.6 Mcal of fat per day (72 mL of vegetable oil) in order to achieve 18 Mcal of energy. In contrast, a 4% NSC Blue Grama hay would provide 13.5 Mcal/day, which would allow a reasonable addition of 4.5 Mcal of fat per day (538 mL of vegetable oil).
SELECTION OF FAT SOURCE. High -fat diets increase plasma free fatty acid concentrations and thus the availability of fats for oxidation in skeletal muscle.218 Long-chain fat diets also appear to increase glycogenolytic, glycolytic, and oxidative flux in PSSM1 muscle as shown by higher glucose 6-phospate, lower lactate, and higher pyruvate concentrations in the muscle of PSSM1 horses fed and trained on a commercial high-fat diet (Re-Leve [Kentucky Equine Research, Versailles, Ky.]) compared with sweet feed.220 Thus one means to overcoming limitations in delivery of oxidative substrates in PSSM1 horses is to provide ample long-chain fat in the diet. The major sources of dietary fat for horses are vegetable based, including vegetable oils and rice bran or animal-based fat (tallow [solid rendered fat of cattle and sheep], lard, fish oil). Vegetable oils are highly unsaturated, very digestible (90% to 100%), and very energy dense. Suitable forms include soybean, corn, safflower, canola, flaxseed, linseed, peanut, and coconut. Controlled research studies in exercising PSSM horses have shown a decrease in muscle pain and serum CK in response to the addition of corn oil233 and also a concentrate of soybean oil and rice bran (Re-Leve).218 The amount of oil added in these trials constituted at least 13% of daily DE. Some veterinarians have advocated that as much as 25% of DE be fed in the form of fat to PSSM horses.193 As discussed earlier, the principal consideration here should be whether this provides excessive calories and additional weight gain because feeding 13% DE as fat may well be effective in reducing muscle pain. Limited research has been performed on the form of oil to feed PSSM horses. Whether there is any direct beneficial effect on skeletal muscle of providing energy in the form of omega-3 versus omega-6 fatty acids has yet to be determined. Due to the potential additional oxidant stress of fats, vitamin E (1000 to 5000 U/day) should be fed to horses receiving high-oil diets.
LOW-STARCH, HIGH-FAT CONCENTRATES. Although oils are energy dense and inexpensive, they have the disadvantages of being messy, unpalatable to some horses, prone to rancidity in warm temperatures, and difficult to feed in large amounts. As such, a number of concentrates that contain fats have been developed. The important principle to be met by such feeds is that the starch and sugar components are low enough and the fat supplementation high enough to ensure that in the total diet, the calories supplied by NSC comprise no more than 10% to 15% of the daily DE and the calories supplied by fat comprise about 12% to 15% of daily DE.218 Common fat sources used in such concentrates include, in addition to the oils mentioned earlier, stabilized rice bran or animal fats. Rice bran and its products are palatable to most horses, have a moderate NSC content approximately 25% by weight, contain approximately 20% fat by weight, as well as vitamin E, and are naturally high in phosphorus. The NSC component of rice bran can vary if the manufacturing process is not careful to exclude the white rice grain. Commercial rice bran products occur as powder or an extruded pellet and are considerably more stable in warm temperatures compared with animal fat and vegetable oils. A number of well-balanced, low-starch, high-fat commercial diets are suitable for horses with PSSM.218 Some commercial feeds meet the recommended nutritional needs of PSSM horses in one pelleted ration. These feeds typically contain at least 10% to 15% fat by weight and less than 20% NSC by weight. Some feed companies offer similar nutritional content by blending two or more manufactured feeds or by supplementing with oils or rice bran. At present, the NSC content of equine feed products is not consistently listed on the feed tag, and consultation with the feed manufacturer is necessary to obtain this information. Nutritional support is available through most feed manufacturers in designing an appropriate diet. There is a great deal of variation in individual tolerance to dietary starch; however, horses with more severe clinical signs of PSSM appear to require the greatest restriction in starch intake.
EXPECTATIONS. The beneficial effects of low-starch, high-fat diets require that horses are trained daily to enhance enzymes involved in fat and glucose metabolism. It is important to note that a horse diagnosed with PSSM will always have an underlying predilection for muscle soreness, and the best that can be done is to manage horses to minimize clinical signs. With adherence to both diet and exercise recommendations, 70% to 75% of Quarter Horses and warmbloods show notable improvement in clinical signs, and many return to acceptable levels of performance.189,193,226,227 There is, however, a wide range in the severity of clinical signs shown by horses with PSSM; those horses with severe or recurrent clinical signs will require more stringent adherence to diet and exercise recommendations in order to regain muscle function. PSSM horses that also have the mutation for malignant hyperthermia do not respond as well to diet and exercise recommendations and may continue to develop ER with the possibility of a fatal episode.207
Myofibrillar Myopathy
Myofibrillar myopathy (MFM) is a recently identified disorder in horses presenting with exercise intolerance or intermittent ER that is defined by specific histopathology.235-237 First and foremost, MFM horses have cytoplasmic aggregates of the cytoskeletal protein desmin in scattered muscle fibers. Desmin functions to align sarcomeres at the Z-disc and tether them to the cell membrane. Other ultrastructural derangements evident in electron microscopy include disrupted myofibrillar alignment, ectopic accumulation of cytoskeletal proteins and Z-disc degeneration. In some cases, MFM is also characterized by cytoplasmic aggregates of glycogen similar to PSSM2.235,237 This is likely because pools of glycogen form within disrupted myofibrils. MFM may represent a more extreme subset of PSSM2. Muscle glycogen concentrations in horses with MFM are similar to controls.
Warmblood horses diagnosed with MFM have an insidious onset of exercise intolerance notable by 6 to 8 years of age characterized by lack of stamina, unwillingness to go forward, inability to collect, abnormal canter transitions, and inability to sustain a normal canter.237 Unresolved hindlimb lameness, stiffness, muscle pain, and, rarely, an episode of ER are reported. Serum CK and AST activities are usually within normal limits unless samples are taken in conjunction with ER.237
Arabian endurance horses diagnosed with MFM usually have a history of intermittent elevations in serum CK activity after endurance rides (> 10,000 U/L) or during exercise that follows a week or more of rest.235,236 Horses do not necessarily always show the same degree of pain, sweating, and reluctance to move as is frequently seen in other forms of acute ER. Myoglobinuria can be observed in horses with only mild muscle stiffness. Between episodes, the heart rate, lactate, CK, and AST responses to exercise are normal.236
The best means to manage horses with MFM has yet to be determined. Many horses have been managed in a way similar to horses with PSSM2. There is no information to suggest that limiting NSC or the addition of fat is necessarily of benefit to horses with MFM. The addition of an amino acid supplement (whey based) is currently being tried as a mechanism to enhance turnover and regeneration of myofibrils within muscle cells.237
Recurrent Exertional Rhabdomyolysis
The term recurrent exertional rhabdomyolysis (RER) describes a subset of ER that is believed to be due to an abnormality in the regulation of muscle contraction and relaxation.7,19,21,238 Research into RER has primarily been performed in Thoroughbreds and, to a lesser extent, Standardbreds.21,187,215,239 Scientific studies of RER have used a small number of horses that share common clinical signs of ER and have abnormal muscle contracture tests.19-21 Broader epidemiologic and genetic studies have assumed that the same pathophysiologic basis for ER exists in the majority of Thoroughbreds and Standardbreds with similar clinical signs. Whether this is true or not will require more research. There are reports of some Arabians and warmbloods with ER that may also suffer from RER on the basis of overlapping histories, clinical signs, muscle biopsy findings, and response to management.227
■ Pathogenesis Rhabdomyolysis is triggered suddenly during exercise in RER horses, which results in a sharp rise in serum myoglobin and CK activity.6 Clinically, the triggering event is often associated with excitement in a horse that already has an underlying nervous temperament.187,215,239 Serum cortisol concentrations are higher in RER horses than normal horses before exercise and increase during an episode of ER.240 Serum concentrations of epinephrine and norepinephrine are normal before an episode but increase dramatically in horses with marked elevations in serum CK activity.240
EXERCISE AND EXCITEMENT. In Standardbreds, ER commonly begins after 15 to 30 minutes of jogging at 5 m/s, although clinical signs may not be apparent until after exer- cise.6,215 In Thoroughbreds exercising on the treadmill, ER most commonly develops with intervals of walk, trot, and canter and is less common if horses are allowed to gallop.241,242 At the racetrack, ER occurs commonly when RER horses are held back to a paced gallop.243 During eventing, RER commonly occurs after the excitement of the steeplechase or early in the cross-country phase when horses are held to a predetermined speed. ER rarely occurs when horses are allowed to achieve maximal exercise speeds, such as in racing.187,215,242-244 A day or more of rest before this type of exercise results in higher serum CK activity post exercise.215,242
There is no basis for an association between RER and lactic acidosis.242
INTRACELLULAR CALCIUM REGULATION. Horses with RER are believed to have an intrinsic abnormality in intramuscular calcium regulation that is intermittently manifested during exercise.19,245 Basal muscle intracellular calcium concentrations in RER horses are similar to healthy horses on the basis of assays in muscle cell cultures.245 Higher intracellular calcium concentrations have been measured in horses of unspecified breeds during an episode of ER246; however, this also could be secondary to any insult that impairs energy generation or cell membrane integrity. Contracture testing has been performed in horses using surgically excised bundles of semimembranosus21 or external intercostal muscle.247 Waldron-Mease and col- leagues248 and Beech and colleagues21 found that caffeine contracture thresholds were lower in semimembranosus muscle from Thoroughbreds and Standardbreds susceptible to RER versus breed-matched controls. Lentz and colleagues studied intact external intercostal muscle fibers from six Thoroughbreds with RER and found a lower contracture threshold for triggering agents such as potassium, caffeine, and halothane compared with control horses.19 An abnormality in intracellular calcium regulation was also supported by a muscle cell culture study of RER Thoroughbred horses.245 A lower threshold for induction of myoplasmic calcium release by caffeine was found in myotube cultures from six RER Thoroughbreds compared with controls. Thus all of these studies supported an abnormality in intracellular calcium regulation in most of the Thoroughbred or Standardbred horses studied. However, studies of isolated muscle membranes have not conclusively identified any specific abnormalities in intracellular calcium regulation in RER horses.171 Further, genetic linkage analysis using 96 horses in 4 families of Thoroughbred horses segregating for RER did not find an association linking RER with the calcium regulatory genes RYR1 (ryanodine receptor), SERCA (SR ATPase), or DHPR1 (dihydropyridine receptor).249 Thus in spite of many detailed investigations of a small number of horses, the exact defect in regulating muscle contraction in RER horses has yet to be identified.
■ Prevalence and Risk Factors Assuming that the majority of cases of ER at racetracks are due to RER, the prevalence in Thoroughbred racehorses is remarkably similar around the world, with estimates ranging from 4.9% in the United States239 to 5.4% in Australia184 to 6.7% in the United Kingdom.187,244 The annual incidence of ER in Standardbred racehorses in Sweden is 6.4%.215 Exercise obviously increases the prevalence of RER in horses, and episodes are observed more frequently once horses achieve a level of fitness.215,239
In Standardbreds and Thoroughbreds, mares more commonly have RER than males,187,215,239 but no general correlation has been observed between episodes of rhabdomyolysis and stages of the estrus cycle.250 There is an interaction between age and gender in RER Thoroughbred horses such that the proportion of affected females to males is much higher in young horses compared with older age groups.239 Swedish Standardbreds with RER, which do not begin racing until 3 years of age, did not show the same age association with RER as Thoroughbreds.215 Temperament has a strong effect on the expression of RER in both Standardbreds and Thoroughbreds, with nervous horses, particularly fillies, having a higher incidence of rhabdomyolysis than calm horses.187,215,239 Young fillies are more likely to have a nervous temperament than mares or male horses. Diet also has an impact, with Thoroughbred horses fed more than 2.5 kg of grain per day being more likely to show signs of RER.241,242 One study also found a higher prevalence of rhabdomyolysis among Thoroughbred horses with lameness.243 A few days of rest before exercise increases the degree of elevation on serum CK activity with the next exercise session and in practice predisposes horses to an episode of ER.242
■ Genetics A genetic susceptibility to RER has been suggested for Thoroughbred horses.190,251-253 Standardbred trotters with a history of RER actually have faster racing times from a standstill start than those without a history of RER, suggesting the trait may have beneficial and deleterious effects.215 The variable penetrance of RER, however, and other potential modifying genes have made a genetic basis for RER suspected but difficult to identify.254
■ Diagnosis A presumptive diagnosis of RER is based on clinical signs of muscle pain and the presence of risk factors commonly associated with RER. Muscle histopathology is nonspecific in RER horses; either no abnormalities or evidence of centrally located nuclei in mature fibers and potentially waves of myofiber degeneration or regeneration is found.7 There is a notable absence of abnormal amylase-resistant polysaccharide, although increased subsarcolemmal amylasesensitive glycogen may be present.7 The value of a muscle biopsy as a diagnostic tool in horses with suspected RER is largely confined to particularly recurrent unmanageable cases where a need arises to rule in or out other forms of ER. Serum CK and AST activities serve as the basis for detecting muscle degeneration, and they often show intermittent abnormal elevations that return to normal relatively quickly during the course of training. If CK elevations are mild, there are a number of factors to consider. Timing of the sample with regard to the onset of ER and exercise are important. Reliability is improved by obtaining blood samples at a standardized time after exercise, preferably 4 to 6 hours when CK peaks, and consistently with regard to exercise on the preceding day because serum CK activity is higher on exercise days that are preceded by a day or more of rest.186 In addition, normal values need to be adjusted for the age and sex of horses. Two-year-old fillies generally have greater fluctuations in serum CK activity during race training than 3-year-old fillies or geldings.186
■ Management Prevention of rhabdomyolysis in horses susceptible to RER is complex, and multiple factors need to be changed to decrease episodes. These factors include the environment, the exercise regimen, and diet. In addition, medication may be necessary at times to prevent further episodes of muscle damage.
ENVIRONMENT. Because excitement and nervousness often trigger rhabdomyolysis, stressful situations in the environment that can be modified need to be identified. This may involve a change to a smaller barn with fewer horses and fewer handlers, compatible companions, and a more consistent daily routine. Many stressed RER-susceptible horses respond to a regular routine, including feeding first before other horses and training first before other horses, especially if the horse becomes impatient while waiting. Other horses respond to being housed in a quiet area of the barn next to calm, companionable horses. The use of hot walkers, exercise machines, and swimming pools needs to be evaluated on an individual basis because some horses develop rhabdomyolysis when using this type of equipment. Horses that develop rhabdomyolysis at specific events, such as horse shows, may need to be reconditioned to decrease the stress level associated with such events or tranquil- ized as part of the accommodation process. Providing daily turnout with other horses seems to be beneficial for RER horses and may decrease anxiety and thereby the likelihood of rhabdomyolysis.
EXERCISE. Although a period of rest is recommended for sporadic forms of ER until serum CK normalizes, it is not recommended for horses with RER.14 Daily exercise is important in preventing episodes of rhabdomyolysis, and therefore when serum CK is less than about 3000 U/L, horses are returned to regular daily exercise. Horses with more severe episodes of rhabdomyolysis may require additional time off in a paddock before gradually resuming exercise. Once back in training, some form of daily exercise is recommended. Avoiding fighting to hold racehorses to slower speeds during galloping may decrease rhabdomyolysis in RER-susceptible Thoroughbreds. Interval training and reduction of jog miles to no more than 15 minutes per session will benefit Standardbreds. For horses under saddle, a relaxed warm-up with intermittent periods of long, low stretching may be of benefit, and continued breaks to stretch between episodes of collection are recommended. Event horses may require training that incorporates calm exposure to speeds achieved during the steeplechase or cross-country phase, especially when used in an interval training program.
DIET. A nutritionally balanced diet with appropriate caloric intake and adequate vitamins and minerals are the core elements of managing RER. For RER Thoroughbreds and Standardbreds in training, the challenge is usually supplying enough calories in a highly palatable form to meet their daily energy demands. This is in part because they often require more than 30 Mcal of digestible energy (DE) a day (5 kg sweet feed, 1.5% of body weight in hay) and, due to their nervous temperament, they may be more discriminating in their eating habits. Out of the total daily calories required by RER horses, research suggests that less than 20% DE be supplied by NSCs (starch and sugar) and at least 20% of DE be supplied by fat.242
Selection of Forage. Thoroughbred horses do not appear to show the same significant increase in serum insulin concentrations in response to consuming hay with an NSC of 17% that is seen in Quarter Horses (Borgia L, 2010 PhD thesis, University of Minnesota). This fact combined with the high caloric requirements of racehorses may mean that it is not as important to select hay with very low NSC content in RER Thoroughbreds as it is in PSSM horses. Anecdotally, some trainers find that horses with RER have more frequent episodes on alfalfa hay. The nervous disposition of some RER horses may predispose them to gastric ulcers, and thus frequent provision of hay with a moderate NSC and mixed alfalfa content may be indicated.
Low-Starch, High-Fat Concentrates. When RER Thoroughbreds are fed a moderate caloric intake (24 Mcal/ day) in the form of high-starch concentrates (2.5 kg of corn, oats, wheat middlings, and molasses), they show little elevation in serum CK activity with exercise.241 Most Thoroughbred racehorses, however, are fed at least 5 kg of high-starch concentrate per day at 30 Mcal or more per horse per day, and at this level of feeding postexercise serum CK activity rises significantly.242 The discovery that substitution of fat for starch in a high-calorie ration significantly reduces muscle damage in exercising RER horses was a major advance in nutritional management of RER.242 Practically, however, it was difficult to achieve the desired caloric intake of racehorses because the maximum amount of fat that finicky Thoroughbreds will happily consume is limited often to 600 mL of vegetable oil or 5 lb/day of balanced rice bran. Management of RER horses was significantly improved when a palatable means to provide the amount of fat required by fit, finicky RER Thoroughbreds was developed. A controlled trial using a specialized feed developed for RER (Re-Leve: 13% fat by weight and 9% NSC) determined that NSC should be no greater than 20% of daily DE and that 20% to 25% of daily DE should be provided by fat for optimal management of RER horses fed 30 Mcal or more per day.242 No beneficial effect on serum CK activity occurred when sodium bicarbonate (4.2% of the pellet) was added to a high-starch pellet feed.242 The amount of fat in the diet of an RER horse depends on its caloric requirements. Over and above hay at 1.5% to 2% of body weight and 2.5 kg of grain, any additional calories should be supplied by fat.
The benefit of a fat diet does not appear to be a change in muscle metabolism. Muscle glycogen and lactate concentrations before and after exercise are the same in RER horses fed a low-starch, high-fat diet compared to those fed a high-starch diet.242,255 Rather, low-starch, high-fat diets in RER horses may decrease muscle damage by assuaging anxiety and excitability, which are tightly linked to developing rhabdomyolysis in susceptible horses. Low-starch, high-fat diets fed to fit RER horses produce lower glucose, insulin, and cortisol responses and lead to a calmer demeanor and lower preexercise heart rates.256 Neurohormonal changes may develop in response to high serum glucose, insulin, and cortisol concentrations, resulting in an anxious demeanor. Although a calm demeanor is desired during training, some racehorse trainers feeding low-starch, high-fat feeds prefer to supplement with a titrated amount of grain 3 days before a race to potentially increase liver glycogen and increase a horse's energy during the race.
Expectations. Studies in RER horses show that significant reductions or normalization of postexercise serum CK activity occurs within a week of commencing a low-starch, high-fat diet.242 Days off training in a stall are discouraged because postexercise CK activity is higher following 2 days of rest compared with values taken when performing consecutive days of the same amount of submaximal exercise.
SUPPLEMENTS. Horses require daily dietary supplementation with sodium and chloride in the form of either loose salt (30 to 50 g/day) or a salt block. Additional electrolyte supplementation is indicated in hot, humid conditions. A myriad of supplements that are purported to decrease lactic acid buildup in skeletal muscle of RER horses are sold. These include sodium bicarbonate, B vitamins, branched-chain amino acids, and dimethylglycine. Because lactic acidosis is no longer implicated as a cause for rhabdomyolysis, it is difficult to find a rationale for use of these supplements.
MEDICATIONS. Low doses of tranquilizers such as aceproma- zine before exercise have been used in RER horses prone to excitement.257 A dose of 7 mg IV 20 minutes before exercise is reported to make horses more relaxed and manageable. Reserpine and fluphenazine, which have a longer duration of effect, have also been used for this purpose. Horses given fluphenazine may occasionally exhibit prolonged bizarre behavior. Use of tranquilizers may be necessary only when horses are in their initial phase of training and accommodating to a new environment. Horses obviously cannot compete on these medications, and withdrawal times must be observed.
Dantrium sodium acts to decrease release of calcium from the ryanodine receptor in skeletal muscle and is used to treat malignant hyperthermia. Controlled and field studies have shown that oral dantrolene can significantly decrease signs of rhabdomyolysis in RER horses.168,258,259 One study indicated that horses need to be fasted to achieve measurable blood levels of dantrolene,168 but more recent controlled trials suggest that absorption of dantrium is superior in fed versus fasted horses.258 Administration of 4 mg/kg of dantrium PO 1 hour before exercise to RER-susceptible horses fed high-grain diets resulted in significantly lower serum CK activity 4 hours after exercise compared with placebo.168 A dose of 800 mg of dantrium was given to Thoroughbred horses in the United Kingdom 1 hour before exercise and resulted in significantly lower postexercise CK activity than a placebo.259
Phenytoin has been reported to be effective in preventing rhabdomyolysis in horses with RER.260 Phenytoin acts on a number of ion channels within muscle and nerves, including sodium and calcium channels. Therapeutic levels vary, so oral doses are adjusted by monitoring serum levels to achieve 8 μg∕mL, not to exceed 12 μg∕mL.260 Drowsiness and ataxia are evidence that the dose of phenytoin is too high, and the dose should be decreased by half. Initial dosages are 6 to 8 mg/kg PO twice a day for 3 to 5 days, and if the horse is still experiencing rhabdomyolysis but is not drowsy, the dose can be increased by 1-mg/kg increments every 3 to 4 days. Most horses require a dose of 10 to 12 mg/kg PO twice daily (bid). Phenytoin is a monoaminoxidase activator and can affect dosages of other medications. Unfortunately, long-term treatment with dantrolene or phenytoin is expensive, and these drugs must be withdrawn before competition.
HORMONE THERAPY. Various hormones, ranging from thyroxine to progesterone and testosterone, have been given to horses with RER. Initial studies linking low T3 and T4 concentrations in horses with ER have not been substanti- ated.261-263 Some mares appear to exhibit signs of rhabdomyolysis during estrus, and it may well be of benefit in these horses to suppress estrous behavior using progesterone injections. Testosterone and anabolic steroids have been used at racetracks to prevent signs of RER, but their use is no longer permitted.
ADJUNCT THERAPIES. Massage, myofascial release, mesotherapy, stretching, aqua treadmills, and hot/cold therapy performed by experienced therapists may be of benefit in individual cases.264-266 Their use may promote relaxation and normal muscle tension and build muscle strength.
Malignant Hyperthermia
Malignant hyperthermia (RYR1 mutation) in Quarter Horses and Paints has also been linked to exertional rhabdomyolysis.173,174 It is caused by an autosomal dominant mutation that exists in exon 46 of the skeletal muscle RYR1 gene on ECA 10.
■ Prevalence and Risk Factors Malignant hyperthermia is a rare disorder in Quarter Horses and Paints, affecting less than 1% of the breed. Halter and pleasure horse lines have the highest prevalence. Rhabdomyolysis may be induced by exercise and anesthesia but can be extremely intermittent in nature.173
■ Clinical Signs Horses with the RYR1 mutation may intermittently show signs of ER and high body tempera- tures.173,174 Some horses affected with malignant hyperthermia have died suddenly after an episode of ER. Horses with the RYR1 mutation may also have the GYS1 mutation associated with PSSM1.219 Such horses have more severe episodes of ER, higher serum CK activity after exercise, and a more moderated response to the diet and exercise regimens recommended for PSSM1.219
■ Diagnosis Genetic testing is recommended in Quarter Horses and Paints with difficult-to-manage forms of PSSM or a family history of postanesthetic complications. Muscle biopsy is not particularly useful for diagnosing malignant hyperthermia. Biopsies may contain mild myopathic changes, including increased variation in fiber sizes, centrally located nuclei, fiber necrosis, glycogen depletion, and ringbinden fibers.174
■ Treatment The nature of ER with horses positive for malignant hyperthermia is so intermittent that it is hard to justify premedication with dantrolene before exercise.