Myotonic Disorders
Stephanie J. Valberg
Myotonic muscle disorders represent a heterogeneous group of diseases that share the feature of delayed relaxation of muscle after mechanical stimulation or voluntary contraction.
Abnormal muscle membrane excitability appears to be the shared abnormality among myotonic disorders. The nondystrophic myotonias in large animals include myotonia congenita in horses and goats and equine hyperkalemic periodic paralysis.28 Sarcolemmal ion channel dysfunction causes these nondystrophic myotonias. Dystrophic myotonia, a progressive disease that may also be associated with abnormalities in other body systems, has been reported in horses.29,30 In addition, it has been noted that some horses with ear tick infestations develop percussion myotonia and painful muscle cramps.31Myotonia
CLINICAL SIGNS. Myotonia congenita in humans, horses, and goats is usually detected in the first year of life.39-42 Affected animals commonly have conspicuously well-developed musculature and display mild to moderate pelvic limb stiffness. Gait abnormalities are usually most pronounced when exercise begins and frequently diminish as exercise continues. Bilateral bulging (dimpling) of the thigh and rump muscles is often obvious and gives the impression that the animal is well developed (Fig. 42.3). Stimulation of affected muscles, especially percussion, exacerbates the muscle dimpling below a large area of tight contraction (Fig. 42.4). Affected muscles may remain contracted for up to a minute or more with subsequent slow relaxation.30,42 Myotonia congenita does not usually show progression of clinical signs beyond 6 to 12 months of age in horses.30
In goats, myotonia congenita appears to be an autosomal dominant mutation in the skeletal muscle chloride channel (CLCN1) that has incomplete penetrance.24,41,43 Affected goats are commonly referred to as “fainting goats.” Signs are usually recognizable by 6 weeks of age and vary from stiffness after rest to marked general rigidity after visual, tactile, or auditory stimulation.
Clinical signs remain throughout the animal's life but are not progressive.44 An autosomal recessive c.1775A>C mutation was identified in a New Forest pony with congenital myotonia. The missense mutation results in a substitution of aspartic acid for alanine in codon 592 of the C-terminal cytoplasmic domain of the equine CLCN1 protein.45Myotonia dystrophica appears to be a separate form of myotonia in horses.29,30,46 Severe clinical signs of myotonia that progress to marked muscle atrophy and possibly involve a variety of organ systems have been observed in Quarter Horse, Appaloosa, and Italian-bred foals. Retinal dysplasia, lenticular opacities, and gonadal hypoplasia have been reported in one such Quarter Horse foal.29 This condition resembles myotonia dystrophica in humans, which is caused by genetic mutations involving either the DMPK gene or the ZNF9 gene.47,48 In both cases, a short segment of deoxyribonucleic acid (DNA) is abnormally repeated many times, forming an unstable region in the gene, which alters messenger ribonucleic acid (mRNA) processing. The genetic basis of myotonic dystrophy in horses is not yet known.
■ Diagnosis A tentative diagnosis frequently can be made on the basis of age, clinical signs (stiff gait, particularly at the onset of exercise), muscle bulging, and prolonged contractions following muscle stimulation.
Definitive diagnosis of myotonia is usually based on electromyographic examination. Affected muscle manifests pathognomonic, crescendo-decrescendo, high-frequency repetitive bursts with a characteristic “dive bomber” sound.29,46,49 This sound is produced by the repetitive firing (after contractions) of affected muscle fibers. After a contraction diminishes, the excitability of muscle fibers is decreased and the action potentials recorded by the EMG reflect the diminution of electrical activity.50
Examination of muscle biopsies from foals with myotonia congenita may be normal or may demonstrate extremely variable muscle fiber dimensions up to twice those of normal age- matched controls.42 Type I fiber hypertrophy or hypotrophy
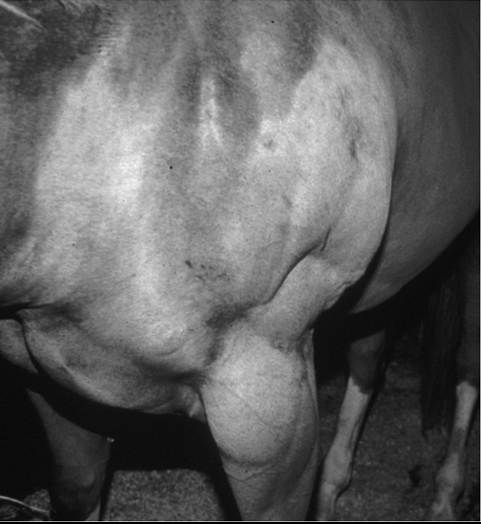
FIG.
42.4 Myotonic dimpling of the triceps in a horse with hyperkalemic periodic paralysis.
FIG. 42.3 Normal muscle mass in an Appaloosa foal (A) and spontaneous myotonic dimpling of semimembranosus muscles in a foal with myotonic dystrophy (B).
may be seen. The major changes noted with myotonic dystrophy are ringed fibers, alterations in the shape and position of myonuclei, sarcoplasmic masses, and an increase in endomysial and perimysial connective tissue.29,30,46,51 Fiber type grouping and atrophy of both type I and type II muscle fibers may be present.
■ Treatment Considering that the pathophysiologic basis of myotonia in horses has not been clearly identified, recommendations for specific, effective therapy are almost impossible. In affected humans and dogs, some relief of signs has been provided by drugs such as quinine, procainamide, and phenytoin. However, responses vary among patients. Phenytoin has been reported to be efficacious in two Quarter Horses with hyperkalemic periodic paralysis and myotonic dystrophy.49
■ Prognosis Prognosis appears to be variable and dependent on the severity of clinical signs. Mildly affected animals with congenital myotonia may undergo some amelioration of clinical signs with increasing age over a period of months to years. The reason(s) for this regression of signs is unknown. Other, more severely affected horses, particularly those with dystrophic myotonia, may have progression of signs, including atrophy and fibrosis or pseudohypertrophy to the point at which the animal is no longer able to move without great pain and difficulty (Fig. 42.5). Euthanasia of such animals is often warranted. Although conclusive evidence regarding the genetic basis of dystrophic myotonia in horses is still not available, owners of affected horses should be cautioned as to the possibility of this disease being heritable.
Hyperkalemic Periodic Paralysis
Sharon Jane Spier
Equine hyperkalemic periodic paralysis (HYPP) is caused by an inherited defect in the skeletal muscle sodium channel.28,52-55 This myopathy manifests as abnormal skeletal muscle membrane excitability leading to episodes of myotonia, or sustained muscle contraction, and paralysis. In humans, numerous muscle membrane channel defects (so-called channelopathies) have been characterized, and the molecular basis for disease is well described.40 Other reported disorders with suspected membrane defects in horses include myotonic dystrophy and congenital

FIG. 42.5 Marked progressive atrophy of the epaxial and gluteal muscles of a horse with myotonic dystrophy.
myotonia.29,42 Hyperkalemic periodic paralysis was the first equine disease attributed to a specific genetic mutation and detectable through DNA technology.54
Hyperkalemic periodic paralysis is an autosomal dominant trait affecting Quarter Horses, American Paint Horses, Appa- loosas, and Quarter Horse crossbred animals worldwide. A “syndrome” in related horses was first recognized in the 1980s by breeders and veterinarians and first reported to be similar to HYPP in humans by Cox at the American Association of Equine Practitioners convention in 19 8 5.55 In December 2002, this genetic disease was publicly linked to a popular Quarter Horse sire named Impressive. This prolific sire, born in 1969, has more than 500,000 offspring registered with the American Quarter Horse Association (AQHA; AQHA registrar, personal communication, 2012), and these offspring dominate the halter horse industry. Current estimates indicate that 1.5% of Quarter Horses and 4.5% of Paints are affected.56 Notably, however, 58% of halter horses have the HYPP mutation.55 Unfortunately, the gene frequency has not decreased in the past 20 years since genetic testing has been available to breeders, and controversy continues among horse breeders whose stock carry this gene (statistics from UCD Veterinary Genetics Laboratory HYPP Testing, 2006).
Affected horses appear to have been preferentially selected as breeding stock due to their pronounced muscle development, and there is evidence of selection of HYPP-affected horses as superior halter horses by show judges.57 In 1996 AQHA officially recognized HYPP as a genetic defect or undesirable trait. To increase public awareness of this genetic defect, mandatory testing for HYPP with results designated on the Registration Certificate began for foals descending from Impressive born after January 1, 1998. In response to requests from the membership, the AQHA Stud Book and Registration Committee ruled that foals born in 2007 and later testing homozygous affected for HYPP (H/H) are not eligible for registration. Breeders opposed to restrictions argue that the disease can be controlled through diet and medication and that these horses are highly successful in the show ring.58■ Clinical Signs Clinical signs among horses carrying the same mutation range from asymptomatic to daily muscle fasciculations and weakness. In the majority of horses, intermittent clinical signs begin by 2 to 3 years of age with no apparent abnormalities between episodes.28,53 Ingestion of diets high in potassium (>1.1%), such as those containing alfalfa hay, molasses, electrolyte supplements, and kelp-based supplements, or sudden dietary changes commonly trigger episodes.59 Fasting, anesthesia or heavy sedation, trailer rides, and stress may also precipitate clinical signs; however, the onset of signs is often unpredictable, without a definable cause. Other possible precipitating factors that have been noted in humans and horses are exposure to cold, fasting, pregnancy, and concurrent disease and rest following exercise. Exercise per se does not appear to stimulate clinical signs, and serum CK shows no change or only modest increases during episodic fasciculations and weakness.
In most cases, clinical episodes begin with a brief period of myotonia, with some horses showing prolapse of the third eyelid.
Sweating and muscular fasciculations are observed commonly in the flanks, neck, and shoulders. The muscle fasciculations become more generalized as additional muscle groups are involved. Stimulation and attempts to move may exacerbate muscular tremors. Some horses may develop severe muscle cramping. Muscular weakness during episodes is a common characteristic of HYPP. Horses remain standing during mild attacks. In more severe attacks, clinical signs may progress to apparent weakness with swaying, staggering, dog sitting, or recumbency within a few minutes. Heart and respiratory rates may be elevated, and horses may show manifestations of stress (anxious appearance) yet remain relatively bright and alert during episodes. Affected horses usually respond to noise and painful stimuli during clinical manifestations of the disorder. Episodes last for variable periods, usually from 15 to 60 minutes. Several horses have died during acute episodes. Respiratory distress occurs in some animals as a result of paralysis of upper respiratory muscles, and a tracheostomy may be necessary. In addition, young horses that are homozygous for the HYPP trait have been observed to manifest a respiratory stridor and periodically may develop obstruction of the upper respiratory tract. Horses homozygous for HYPP may present for dysphagia or respiratory distress, and endoscopic findings include pharyngeal collapse and edema, laryngopalatal dislocation, and laryngeal paralysis.60 After the episode subsides, horses regain their feet and appear normal with no apparent or minimal gait abnormalities. Although HYPP horses appear normal between attacks, electromyographic examination of affected horses reveals abnormal fibrillation potentials, complex repetitive discharges with occasional myotonic potentials, and trains of doublets between episodes.28,61■ Etiology HYPP results from a point mutation that causes a phenylalanine/leucine substitution in a key part of the voltage-dependent skeletal muscle sodium channel alpha subunit.54 In horses with HYPP, the resting membrane potential is closer to firing than in normal horses.62 Sodium channels are normally briefly activated during the initial phase of the muscle action potential. The HYPP mutation results in a failure of a subpopulation of sodium channels to inactivate when serum potassium concentrations are increased. As a result, an excessive inward flux of sodium and outward flux of potassium ensues, resulting in persistent depolarization of muscle cells and temporary weakness (Fig. 42.6).
■ Diagnosis Descent from the stallion Impressive on the sire or dam's side in a horse with episodic muscle tremors, weakness, or collapse is strongly suggestive of HYPP. Quarter Horse foals born after 1998 that are offspring of an affected parent have a statement recommending DNA testing for HYPP on the Certificate of Registration. In most cases, hyperkalemia (6 to 9 mEq/L), hemoconcentration, and mild hyponatremia occur during clinical manifestations of the disease with normal acid-base balance.28 Serum potassium concentration returns to normal following the abatement of clinical signs. Some affected horses may have normal serum potassium concentrations during minor episodes of muscle fasciculations.53 Differentials
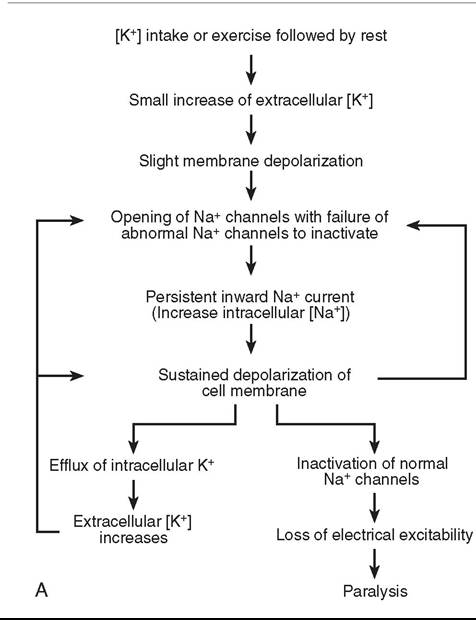

FIG. 42.6 A, Explanation for paralytic attacks in horses with hyperkalemic periodic paralysis (HYPP). B, A horse suffering from an episode of HYPP.
for hyperkalemia include delay before sample centrifugation, hemolysis, acidosis, renal failure, severe rhabdomyolysis, and high-intensity exercise.
Because veterinarians may not be present during acute episodes, the definitive test for identifying HYPP is the demonstration of the base-pair sequence substitution in the abnormal segment of the DNA encoding for the alpha subunit of the sodium channel.54 Submission of mane or tail hair should be made to a licensed laboratory.
■ Treatment Mild exercise can sometimes abort an episode in mild cases or if horses are just beginning to exhibit clinical signs. Feeding grain or corn syrup to stimulate insulin-mediated movement of potassium across cell membranes may also be helpful. Other treatment options, which may abort an episode, include intramuscular (IM) administration of epinephrine (3 mL of 0.006 mg/kg/500 kg) and administration of acetazolamide (3 mg/kg orally [PO], every 8 to 12 hours). Many horses experience spontaneous recovery from episodes of paralysis and appear normal by the time a veterinarian arrives.
■ TABLE 42.1
Examples of Feed Containing High, Medium, or Low Concentrations of Potassium (K+)a
| High-Potassium Feed | K+ (%) | g K+/lb Feed |
| Electrolyte supplements | 30 | 136 |
| Molasses | 6 | 27 |
| Kelp supplements | >4 | >18 |
| Alfalfa hay (90% DM) | 1.4-2.4 | 6.4-10.9 |
| Canary grass hay | 2.6 | 2.6 |
| Orchard grass hay | 2.4-2.6 | 10.9-11.8 |
| Soybean meal | 2 | 9.1 |
| Medium-Potassium Feed | K+ (%) | g K+/lb Feed |
| Fescue hay | 1.7-2.1 | 7.7-9.5 |
| Rice bran | 1.8 | 8.1 |
| Timothy hay | 1.4-2.1 | 6.4-9.5 |
| Coastal Bermuda hay | 1.2-1.9 | 5.5-8.2 |
| Kentucky bluegrass hay | 1.4 | 6.4 |
| Oat hay | 1.4 | 6.4 |
| Low-Potassium Feed | K+ (%) | g K+/lb Feed |
| Pure fats and oils | 0 | 0 |
| Beet pulp | 0.2-0.3 | 0.9-1.4 |
| Corn, oats, or barley | 0.3-0.5 | 1.4-2.3 |
| Pasture grass (23% DM) | 0.3-0.8 | 1.4-3.6 |
| Wheat | 0.4 | 1.8 |
| Wheat bran | 1.2 | 5.45 |
| Soybean hulls | 1.2 | 5.45 |
aTo decrease the frequency of episodes, avoid high-potassium feed; select feed that contains medium to low K+. Feeding a balanced ration containing less than 1.5% K+ and meals less than 33 g K+ decreases fluctuations of blood K+, lowering the frequency of HYPP symptoms.12,15,16
DM, Dry matter.
In severe cases, administration of calcium gluconate (0.2 to 0.4 mL/kg of a 23% solution diluted in 1 L of 5% dextrose) will often provide immediate improvement. An increase in extracellular calcium concentration raises the muscle membrane threshold potential, which decreases membrane hyperexcitability. To reduce the serum potassium, intravenous (IV) dextrose (6 mL/kg of a 5% solution) alone or combined with sodium bicarbonate (1 to 2 mEq/kg) can be used to enhance intracellular movement of potassium. With severe respiratory obstruction, a tracheostomy may be necessary.
■ Control Decreasing dietary potassium and increasing renal losses of potassium are the primary steps taken to prevent HYPP episodes. Foodstuffs to avoid include high-potassium feeds such as alfalfa hay, orchard grass hay, brome hay, soybean meal, sugar molasses, and beet molasses. Optimally, later cuts of Timothy or Bermuda grass hay and grains such as oats, corn, wheat and barley, and beet pulp should be fed in small meals several times a day (Table 42.1). Regular exercise and/or frequent access to a large paddock or yard are also beneficial. Pasture works well for horses with HYPP because the high water content of pasture grass makes it unlikely that horses will consume large amounts of potassium in a short period of time. Ideally, horses with recurrent episodes of HYPP should be fed a balanced diet containing between 0.6% and 1.1% to 1.5% total potassium concentration and meals containing less than 33 g of potassium.59,63,64 Horses will adapt to diets higher in potassium over a period of 2 weeks and will experience fewer fluctuations in potassium in blood with subsequent decreased frequency of clinical signs.63 Because there is a wide variation in potassium concentration of forages depending on maturity and soils, it is advisable to have feeds analyzed for potassium concentrations and other nutrient requirements.64 Table 42.1 contains examples of feeds containing varying concentrations of potassium. Supplement with vitamin E, selenium, salt, and balanced minerals where indicated to meet nutritional requirements. Commercially available complete feeds with a guaranteed potassium content may be more convenient for some HYPP horses, especially for owners with few horses.
For horses with recurrent episodes of muscle fasciculations even with dietary alterations, acetazolamide (2 to 3 mg/kg PO, every 8 to 12 hours) or hydrochlorothiazide (0.5 to 1 mg/kg PO, every 12 hours) may be helpful. These agents exert their effects through different mechanisms; however, both cause increased renal potassium excretion. In addition, acetazolamide stabilizes blood glucose and potassium by stimulating insulin secretion. Breed registries and other associations may have restrictions on the use of these drugs during competitions, as diuretics may mask prohibited substances.
■ Prognosis In most cases HYPP is a manageable disorder, although recurrent bouts may occur and severe episodes can be fatal. Owners of affected horses should be strongly discouraged from breeding these animals for the long-term health of the Quarter Horse and other breeds. Because this is a dominant trait, breeding an affected horse to a normal horse results in a 50% chance of producing a foal with HYPP. All affected horses share the same mutation, regardless of whether owners have witnessed symptoms in their horses.65 Affected horses are not suitable for young or inexperienced riders. Owners of affected horses should advise veterinarians of HYPP status before anesthesia or procedures requiring heavy sedation because these circumstances could precipitate an episode of paralysis.
HYPP-Like Syndrome
Other cases of generalized muscle fasciculations arise in horses after forced exercise or transportation, or in some cases for unknown reasons that last for an hour or less. Horses present with fasciculations in the flanks, lateral neck, and shoulders that can gradually became more generalized. In some cases horses can progress to apparent weakness characterized by swaying, staggering, buckling at the knees, and a basewide stance. An elevated serum potassium at the time of attack has been documented in a Criollo horse.66 The cause of this type of HYPP-like episode has yet to be determined.
Hypokalemic Myopathy in Dairy Cattle
■ Etiology Hypokalemic myopathy in dairy cattle occurs when serum potassium concentrations are below 2.5 mmol/L, producing severe signs of muscle weakness.67-69 Ketosis, anorexia, and enhanced potassium excretion due to the administration of one or more doses of isoflupredone acetate to ketotic cows are common causes of hypokalemia. Isoflupredone acetate has both glucocorticoid and mineralocorticoid activity, resulting in a decrease in mean plasma potassium concentration by 25% two days after one injection (20 mg) and by 46% in cows 3 days after two injections.
■ Clinical Signs and Diagnosis Clinical signs of hypokalemic myopathy include severe weakness, recumbency, abnormal position of the head and neck, rumen hypomotility or atony, abnormal feces, anorexia, and tachycardia. Cardiac dysrhythmia is also common. Diagnosis is based on clinical signs combined with serum potassium of less than 2.5 mmol/L. Other common clinical chemistry abnormalities include ketosis, metabolic alkalosis, and elevated serum CK and AST activities. Muscle biopsies reveal a vacuolar myopathy.
■ Treatment Restoration of whole body potassium balance can be difficult, and serum potassium concentrations do not necessarily reflect muscle potassium concentrations. Recommended supplementation includes potassium chloride given orally (0.1 to 0.4 g/kg body weight), not to exceed 230 g potassium chloride orally per 24 hours. Reserve IV potassium (20 to 40 mEq potassium per liter IV solution, up to 80 mEq/L) for recumbent ruminants with severe hypokalemia and rumen atony. Do not to exceed a maximum infusion rate of 0.5 mEq/kg/h. Early treatment should also be directed at resolving the primary cause of ketosis and anorexia, as well as providing supportive care. Survival has been reported at between 22% and 79%.
Muscle Cramping
Stephanie J. Valberg • Gary P. Carlson
Muscle cramps are a painful condition that arises from hyperactivity of motor units caused by repetitive firing of the peripheral and/or central nervous system. The origin of the cramp in most cases is believed to be the intramuscular portion of the motor nerve terminals.22,70 Most muscle cramps are also accompanied by fasciculations in the same muscle. Muscle cramps can be induced by forceful contraction of a shortened muscle, by changes in the electrolyte composition of extracellular fluid, and by ear tick infestations in horses.22,31 In contrast, muscle contractures are painful muscle spasms that represent a state of muscle contracture unaccompanied by depolarization of the muscle membrane.70 Muscle contractures occur with malignant hyperthermia and some forms of exertional myopathies and are invariably accompanied by markedly increased serum CK activity.
Dietary Electrolytes
Muscle stiffness, weakness, and occasional elevations in serum CK can occur when diets are deficient in sodium or potassium. These chronic deficiencies are rarely reflected in serum electrolyte concentration but may be detected by performing renal fractional excretions of electrolytes.3 Sodium deficiency is particularly common in horses because forage and grain diets are low in sodium and chloride and high in potassium. Supplementation of the equine diet with salt is a necessity. Salt blocks may not be adequate in this regard, and loose salt (1 to 2 oz) added directly in the grain is often the best mechanism of supplementing horses with salt. Some horses may require higher dietary salt supplementation to maintain an adequate sodium balance. Balancing dietary electrolytes has been reported to decrease muscle cramping and serum CK activity in those horses with dietary deficiencies.3
Exhaustion in Endurance Horses
Muscle cramping in endurance horses occurs commonly during prolonged exercise in hot weather, particularly when the humidity is high.71,72 Under such circumstances rectal temperatures reach as high as 41° C, and horses may lose up to 15 L/h of fluids in the form of sweat that is rich in sodium, potassium, and chloride.73,74
■ Clinical Signs Affected horses demonstrate stiffness and cramping in the muscles of locomotion. Pain is a characteristic of the disorder, and affected muscle groups often undergo periodic spasms. In addition, exhausted horses are often dull, depressed, and clinically dehydrated with elevated heart and respiratory rates and persistently elevated body temperature. Common electrolyte abnormalities include a hypochloremic metabolic alkalosis with hypokalemia, hypomagnesemia, and low serum ionized calcium concentrations.71,72,75 Synchronous diaphragmatic flutter may be seen in association with cramping.71 Although many of the signs of muscular dysfunction are similar to those of exertional rhabdomyolysis, affected horses do not generally develop myoglobinuria.71
■ Etiology Factors contributing to cramping are dehydration, electrolyte abnormalities, and disturbances in thermoregulatory and local circulatory function. Whether this disorder is similar to heat cramps seen in human athletes is not known.
■ Diagnosis A variety of electrolyte abnormalities occur in affected animals.71,75 Mild cases are distinguished by the presence of muscle cramps that subside with rest or light exercise in heat-stressed horses. In more severe cases clinical signs of dehydration and shock are often present. Horses with muscle cramping will not have marked elevations in serum CK or AST, nor will they exhibit myoglobinuria. Exhausted horses, however, may progress to develop rhabdomyolysis with marked electrolyte derangements. These horses require immediate treatment.
■ Treatment Under most circumstances the mild form of muscle cramping is self-limiting, and the signs abate with rest or light exercise. However, if evidence of other metabolic derangements exists, treatment for these disorders (e.g., plasma volume expansion with oral or intravenous isotonic polyionic fluids, cooling using water and fans) is frequently beneficial to the horse.76 Because most horses with this condition are alka- lotic, administration of solutions containing sodium bicarbonate is contraindicated. Dietary analysis should be performed to determine the extent of salt and electrolyte supplementation in affected horses. Daily direct addition of 2 oz of sodium chloride and 1 oz of potassium chloride to the feed is recommended for horses with recurrent cramping in addition to electrolyte supplementation before and after endurance rides.
Synchronous Diaphragmatic Flutter
Synchronous diaphragmatic flutter (SDF), also known as “thumps,” usually occurs in horses suffering from derangements in fluid and electrolyte balance. Inciting causes include endurance exercise, hypocalcemia, hypoparathyroidism, digestive disturbances, and possibly the administration of medications. A characteristic clinical manifestation of the disease occurs when the diaphragm contracts in synchrony with atrial depolarization.77’79
■ Clinical Signs The classic sign of SDF is a contraction or twitch in the flank region (unilateral or bilateral) as the diaphragm contracts synchronously with the heart. In severe cases this twitch may produce an audible thumping sound. The metabolic derangements leading to SDF may also be clinically apparent in some cases. These may include signs of dehydration and volume depletion. Endurance horses suffering from SDF in association with the exhausted horse syndrome may demonstrate dehydration, inappropriate sweating responses, persistently elevated body temperature, depression, anorexia, and aperistalsis.71,72 In some horses SDF may be a chronic, recurring problem.77
■ Etiology A variety of stimuli may result in SDF. These include prolonged exercise, particularly during hot weather; hypocalcemia resulting from lactation, transit, or stress; digestive tract dysfunction; furosemide therapy; trauma; and primary hypoparathyroidism.77,79 The most consistent metabolic derangement reported in horses with SDF is low serum ionized calcium concentrations usually associated with hypochloremic metabolic alkalosis.77,78 Metabolic alkalosis may alter the ratio of free to bound calcium (increasing calcium binding to protein and decreasing ionized calcium), which possibly induces SDF.
SDF occurs in association with atrial depolarization in horses. It has been postulated that fluid, electrolyte, and acid-base derangements may disrupt the normal membrane potential of the phrenic nerve, which passes directly over the atrium, resulting in nerve discharges in response to atrial depolarization.77,78,80
■ Treatment In most cases SDF is a transient event, usually abating when the underlying cause resolves, either spontaneously or in response to treatment.77 Most horses undergo rapid remission of signs when given calcium solutions intravenously, as described in the Hypocalcemia in Horses section later. Although hypomagnesemia is often present with SDF, horses do not respond to magnesium supplementation unless calcium is administered concurrently. Response to therapy is also reflected by improved mental status, return of appetite, and gut motility.77
■ Control Electrolyte supplementation and some dietary manipulations may help to reduce the incidence of SDF in some endurance horses suffering recurrent bouts. Providing chloride, potassium, and sodium during prolonged exercise may help to reduce fluid losses and the metabolic alkalosis that commonly accompanies this form of exercise and frequently occurs in association with SDF. Metabolic alkalosis decreases the amount of free calcium available. Supplementation of calcium and magnesium during endurance rides has been suggested as helpful in horses prone to SDF.
Alternative approaches involve reduction of dietary calcium in horses prone to SDF for a few days before an endurance ride. It is postulated that this reduction in dietary calcium stimulates the endocrine homeostatic mechanisms and increases osteoclastic activity. In the short term the horse depends less on dietary calcium and is able to mobilize substantial amounts of calcium in response to the demands imposed by the exercise; calcium losses in sweat are overcome by the release of calcium from endogenous storage pools (bone).77 Further, horses routinely fed alfalfa hay, which has a relatively high calcium concentration, may be more prone to the development of SDF. Limitation of this foodstuff may be indicated in chronically affected horses.
Hypocalcemia in Horses
Hypocalcemia is a relatively rare disorder in horses that has also been referred to as lactation tetany, transport tetany, idiopathic hypocalcemia, and eclampsia.
■ Clinical Signs Clinical signs are variable and include increased muscle tone; a stiff, stilted gait; rear limb ataxia; muscle fasciculations (especially temporal, masseter, and triceps muscles); trismus; dysphagia; salivation; anxiety; profuse sweating; tachycardia; elevated body temperature; cardiac dysrhythmias; SDF; convulsions; coma; and death.81,82 Clinical signs may be remarkably similar to some of those seen with tetanus. This disorder may be progressive (in lactating mares in particular) over a 24- to 48-hour period, and some animals die. Clinical signs are related to the magnitude of the serum calcium concentration. Increased excitability is usually the only sign when values are below normal but above 8 mg/dL. Values of 5 to 8 mg/dL usually produce tetanic spasms and incoordination. Concentrations below 5 mg/dL usually result in recumbency and stupor.
■ Etiology Loss of calcium in milk, especially in mares that produce large amounts of milk, seems to predispose to this disorder.81,82 Other factors, such as heavily lactating mares grazing lush pastures, hard work or prolonged transport, and ingestion of blister beetles (cantharidin toxicosis), may precipitate attacks. Primary hypoparathyroidism has also been diagnosed in a 3-month-old hypocalcemic warmblood foal with weakness and muscle trembling.83
■ Diagnosis Clinical signs are often highly suggestive of hypocalcemia in affected horses. Historic aspects such as lactation, previous prolonged exercise, or transport may also direct the clinician to the suspected diagnosis.81 Definitive diagnosis depends on laboratory demonstration of hypocalcemia, with total calcium concentrations as low as 4 to 6 mg/dL in some cases. In addition, metabolic alkalosis, hypomagnesemia or hypermagnesemia, and hyperphosphatemia or hypophosphatemia have all been found in association with hypocalcemia in horses.81 These alterations may need correction before a return to normal function is seen in some affected animals.
■ Treatment Although many mild cases recover without specific treatment, in others this disorder may be life threatening. Therefore therapy should be encouraged in most cases. Treatment involves the IV administration of calcium solutions such as 20% calcium borogluconate or those recommended for the treatment of parturient paresis in cattle.81 Administration of these solutions at the rate of 250 to 500 mL/500 kg diluted 1:4 with saline or dextrose often results in full recovery, although in some cases it may take several days.81 Relapses do occur. These preparations should be administered slowly in conjunction with close monitoring of the cardiovascular response. Dilution in saline or dextrose before infusion decreases the chance of cardiotoxicity. Normally there is a positive ionotropic effect in response to calcium administration.84 However, alterations in rate or rhythm provide evidence to suspend the infusion. If no response to an initial infusion occurs, a second dose may be given 15 to 30 minutes later. Most cases respond to this form of therapy, although in some cases in which signs persist, repeated treatments may be necessary.
Ear Tick-Associated Muscle Cramping
Intermittent painful muscle cramps have been described in a small number of horses with severe Otobius megnini infestations.31 Muscle cramping is not associated with exercise. These horses show intermittent signs of severe muscle cramping of pectoral, triceps, abdominal, or semitendinosus and semimembranosus muscles lasting from minutes to a few hours, with severe pain that often resembles colic. Horses may fall over when stimulated. Between muscle cramps, horses appear to be normal. Percussion of triceps, pectoral, or semitendinosus muscles results in a typical myotonic cramp. Horses have elevated serum CK activities ranging from 4000 to 170,000 IU/L. Numerous ear ticks (O. megnini) can be identified in the external ear canal of affected horses. Without treatment for ear ticks, the spasms continue; however, local treatment of the ear ticks using pyrethrins and piperonyl butoxide results in recovery within 12 to 36 hours. Acepromazine may be helpful to relieve painful cramping.