Osteomyelitis
Canaan Whitfield-Cargile
■ Definition and Etiology Osteomyelitis is an inflammatory disease of bone and its marrow cavity characterized by bone destruction and caused by infection.1 The location of infection along a bone can vary and will depend on the cause of infection.
Possible locations of infection include a local infection of a single region of bone such as the physis or a focal infection along the diaphysis or a more generalized infection involving several structures, including marrow, cortex, periosteum, and surrounding soft tissue.2 If only cortical bone is affected, it is classified as osteitis. Most osteomyelitis cases in large animals are bacterial in origin, although mycotic infections have been reported.3,4 The origin of infection can be hematogenous spread following bacteremia, especially in neonates, or extension of infection from adjacent soft tissue infection or by direct inoculation often associated with a traumatic event.■ Clinical Signs Clinical signs will depend on location of infection, severity of infection, and in some cases the organism involved. Diagnosis is based on clinical findings and ultimately confirmed with diagnostic imaging with culture and histopathologic evaluation of samples from the affected bone. As stated above, there are some differences in osteomyelitis between neonates and adults. In neonates, osteomyelitis is frequently caused by hematogenous spread due to translocation of bacteria from the umbilicus or other sites of infection (e.g., respiratory, gastrointestinal). In the foal, common anatomic locations of established infections have been described and characterized by a classification system.5 The classification system is based on anatomic location of the infection; S-type infections involve only the synovial membrane, E-type infections involve the articular epiphyseal complex, and P-type infections are infections of the long bone physis.
Clinical signs vary based on location of infection, but typically S-type and E-type infections are associated with lameness and synovial effusion. P-type infections also appear lame, although potentially seem less severe that S-type and E-type infections, and instead of synovial effusion have soft tissue swelling in the area of the affected metaphysis. Irrespective of location of infection, pyrexia often accompanies osseous infection of neonates. Although any structure can be involved, the high-motion joints (i.e., femoropatellar, tarsocrural, carpal, and metacarpophalngeal) are most commonly affected.Osteomyelitis in adults is usually associated with trauma resulting in direct inoculation of deeper tissues ultimately leading to bone infection.6 Hematogenous spread, however, does occur, and this is especially true for cases of osteomyelitis involving the axial skeleton.7 Clearly, clinical signs will depend on site of infection. When limbs are affected, the most common clinical sign is lameness, and the degree of lameness will vary depending on location and severity of infection but is frequently mild initially and then progresses to non-weight-bearing lameness. Other clinical signs of osteomyelitis of adults include regional soft tissue swelling, pain on digital palpation, fever, and draining tracts in the case of traumatic osteomyelitis where the wound has failed to heal.2 Time of onset of clinical signs from injury (including postoperative surgical site infection) is highly variable and may be present as early as a few days or be delayed up to 3 to 4 weeks.8 Chronic osteomyelitis becomes more localized as the disease progresses and often results in a firm swelling over the affected area. Persistent drainage from an incision or area of granulation tissue, mild to severe lameness, or a nonhealing wound are also often seen with disease progression in chronic cases. Drainage may be persistent or intermittent and is generally characterized as purulent.
Osteomyelitis, in conjunction with septic arthritis or tenosynovitis, may result in only mild lameness if the wound is open and able to decompress but will result in non-weight-bearing lameness if the wound seals due to accumulation of exudate and/or synovial fluid resulting in stretching of the joint capsule and other structures.■ Diagnosis Prognosis rapidly decreases with duration of unmanaged synovial and osseous infections in all animals but especially in neonates, so prompt diagnosis is critical. In neonates, persistent lameness that is unresponsive to antiinflammatory
treatment often precedes diagnosis, but lameness can be subtle during the early stages of osteomyelitis and easily mistaken for traumatic musculoskeletal injury rather than an infectious process. It is recommended that any lameness in a neonate be thoroughly evaluated for evidence of infection, including a complete physical examination, serial radiographic evaluation of any abnormal findings, and potentially more advanced imaging when in doubt. Additional diagnostics, especially in the case of subtle disease, include CBC, fibrinogen, and potentially other acute-phase proteins, although all of these have not been studied extensively in the context of osteomyelitis of neonates.9 Fibrinogen greater than 900 mg/dL has been shown to be associated with septic physitis and/or osteomyelitis in foals and could help justify more advanced imaging in cases where the diagnosis is difficult. Advanced imaging, including CT and MRI, is increasingly used to diagnose or more accurately characterize the location and severity of osteomyelitis, especially in neonates, as their size greatly enhances the capability of these approaches and the complex nature of osteomyelitis in neonates frequently indicates a more advanced approach.10,11
In adults, osteomyelitis is difficult to diagnose with radiography in the acute stages, as radiographically apparent osseous changes will take time to develop.
In fact, osteolysis does not appear on radiographs until 30% to 50% of bone mineral is lost, which may take up to 10 to 14 days after infection is established.12 In early stages of disease, soft tissue swelling with or without gas opacities adjacent to the area of infection may be the only abnormalities noted.13 In both adults and neonates, ultrasonography can aid in early diagnosis of osteomyelitis by detecting purulent fluid in soft tissues and periosteal involvement and can provide guidance for other confirmatory diagnostic tests, including aspiration of suspect areas for cytology and culture.14 Radiographic signs of chronic osteomyelitis include soft tissue swelling with bone destruction and new bone formation. Infection of bone may result in the formation of an osseous sequestrum, an isolated portion of radiodense cortical bone that has lost local vascular supply (Fig. 38.21). The sequestrum is well defined by an outline of radiopaque productive new bone formation called an involucrum, which forms as a result of attempts to wall off infection.2 An opening to the sequestrum, the cloaca, is usually present and allows drainage of purulent exudate to the skin surface. Sequestra are prevalent following trauma to horses, with more than 30% of wounds to the limbs resulting in sequestra formation.15 The diagnosis of sequestra is usually made radiographically 3 weeks after initial injury and, occasionally, contrast fistulography can be useful in determining the extent of draining tract communication with bone or joints. Advanced imaging modalities provide greater diagnostic capabilities than radiography and may help in the early detection of osteomyelitis.14 CT gives superior imaging of bone, can be reconstructed in three dimensions, and provides excellent information about the cortical bone and medullary involvement.1 CT is also indispensable for evaluating anatomic locations where interpretation of other imaging modalities is complicated by superimposition of complex anatomy (Fig. 38.22).Microbial culture and sensitivity testing should be performed to confirm a diagnosis of osteomyelitis and to guide selection of antimicrobial drugs for treatment. Samples should be collected aseptically and inoculated directly into culture media to improve the chances of obtaining bacterial growth. Swabs taken from an open draining sinus tract may include commensal bacteria that are not responsible for osseous infection. Both aerobic and anaerobic culture testing should be performed on samples when osteomyelitis is suspected. Blood culture may be useful in isolating the infectious organism in the neonate. If there is any suspicion that the osseus infection has spread to synovial structures, appropriate synovial fluid should be collected aseptically and submitted for cytology and culture

FIG. 38.21 Osseous sequestra formation on the dorsolateral aspect of the third metatarsal bone following a laceration to the level of the periosteum 2 weeks previously. Note the new bone formation (involucrum), the isolated portion of cortical bone (sequestrum), and the radiolucent area surrounding the sequestrum (cloaca).
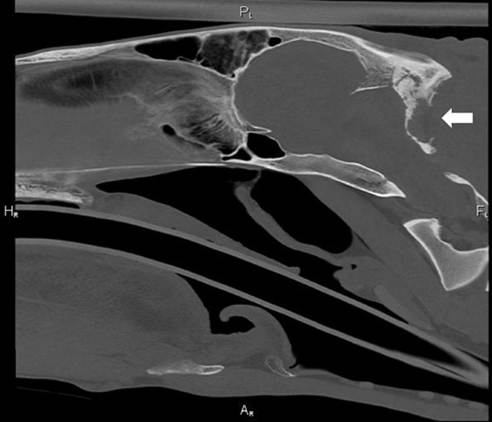
FIG. 38.22 Computed tomography demonstrating osteomyelitis of occipital bone (arrow) following extension of infection from nuchal bursitis.
and sensitivity to confirm involvement. The most commonly isolated gram-negative bacteria from foals include E. coli, Actinobacillus spp., and Salmonella spp. Gram-positive isolates include Streptococcus spp., Staphylococcus spp., and R. equi.l6,17 In the adult horse, members of the Enterobacteriaceae family, Streptococcus spp., and S. aureus are the most commonly isolated microorganisms in cases of osteomyelitis, septic arthritis, and tenosynovitis.8,18
■ Pathophysiology Development of osteomyelitis is related to host factors (i.e., trauma, immune response, etc.) and microbial factors (i.e., virulence, ability to form biofilm, etc.). In the case of sequestra formation, cortical bone becomes exposed, resulting in desiccation of the periosteum, and this may result in a devitalized portion of cortical bone that, if contaminated, can become infected.19 The host response to these bacteria involves invasion of inflammatory cells, including neutrophils that release proteolytic enzymes in an attempt to clear the invading pathogen.
These enzymes are nonspecific, and thus a portion of the surrounding tissue becomes collateral damage (i.e., the cloaca). If the host is unable to eliminate the infection in a timely manner, the exudate accumulates and bacteria colonize adjacent periosteal, cortical, and medullary regions of bone and form a biofilm. A recent study demonstrated that the majority of equine wounds have evidence of biofilm formation, so this should be considered when electing treatment approaches.20,21 Within this biofilm, bacterial microcolonies develop and bacteria become quiescent and are able to evade host immune response and medical therapies while continuing to produce matrix material.22 These defense mechanisms are the principal reason that osteomyelitis persists without aggressive therapy.23 These issues are compounded when foreign material (i.e., metallic implant) or necrotic tissue (i.e., sequestered bone) exists.■ Treatment Early diagnosis and aggressive therapy are critical in preserving normal function to the limb in neonates affected by osteomyelitis and preventing extension of infection in all animals.2 Left untreated, irreversible damage to the growth plate or articular cartilage may cause lifelong debilitating lameness in the affected limb in neonates. As noted above, because bacteria can evade host immune response and medical therapies by residing on necrotic tissue or, more commonly, in a biofilm, medical treatment is often unsuccessful once osteomyelitis is established, and surgical intervention is required. The goals of treatment are to physically remove bacteria, inflammatory debris, and devitalized tissue and to prevent recurrence, as physical removal of all bacteria is rarely possible and therefore recolonization occurs quickly without appropriate continued therapy.24 Long-term medical therapy typically consisting of antibiotics is directed at preventing recurrence, although the length of time to continue and the effectiveness of long-term antibiotics remain questionable in both human and veterinary medicine.25
MEDICAL MANAGEMENT. Medical management, including parenteral antimicrobials and topical wound dressings, may reduce drainage and contain infection to a single area but is rarely successful as a single treatment of osseous sequestra or osteomyelitis. Medical therapy primarily consists of antibiotics, and the selection of antibiotics should ideally be based on culture and sensitivity results. If this information is not available, empirical selection of broad-spectrum antibiotics that will have good delivery to the site of infection is indicated although less than ideal.26 In the neonate, another facet to consider is that osteomyelitis often occurs due to other disease processes, including failure of passive transfer, pneumonia, septicemia, gastroenteritis, colitis, and omphalophlebitis, and thus appropriate diagnosis and management of these comorbidities is a critical component of managing the entire animal when treating osteomyelitis in neonates.
SURGICAL MANAGEMENT. The goal of surgical treatment is to increase efficacy of antimicrobial treatment and host defenses by breaking down the biofilm matrix, removing necrotic debris with infected tissue, promoting vascularization of compromised tissues, and in most cases establishing drainage. For example, in cases of osseous sequestra, sequestrectomy with effective debridement can resolve infection rapidly and decrease the duration of antimicrobial therapy.19 Successful treatment depends on removing necrotic tissue lining the draining tract, opening the cloaca to access and remove the sequestered piece of bone, and aggressive debridement of all infected bone and exudate. Cancellous bone graft or antibiotic-impregnated beads can be used to fill in large defects following sequestrum removal. For other cases of osteomyelitis, the surgical principles are the same and include the goals of debridement of all infection and necrotic tissues, removal of biofilm, and usually establishment of drainage. The surgical technique for accomplishing these goals will vary depending on the details of each case.
LOCAL DELIVERY OF HIGH CONCENTRATIONS OF ANTIMICROBIALS. When possible, local antibiotic delivery is preferred over systemic therapy, as local delivery techniques allow for much higher concentration of antibiotics at the site of infection while avoiding systemic toxicity. Several local delivery techniques are available, including antibiotic-impregnated beads, regional limb perfusion (RLP) techniques, and constant rate infusion systems for synovial structures, to name a few.
ANTIBIOTIC-IMPREGNATED BEADS. Antibiotic-impregnated beads have been used extensively to treat osteomyelitis in horses and other large animal species.27-30 This technique has been shown to be beneficial to the treatment of orthopedic infection in both human and veterinary medicine.31,32 Beads are most commonly made from polymethyl methacrylate (PMMA), which is not biodegradable, or plaster of Paris (POP), which is biodegradable. Although elution characteristics vary based on antibiotic, bead size, bead porosity, and nature of the site of implantation (i.e., highly exudative versus minimal exudate), PMMA elution characteristics are typically described as bimodal with a rapid release in the first 24 hours followed by low-grade, long-term release over weeks to months.33 POP beads, by contrast, typically have rapid high concentration elution characteristics, and POP inherently possesses osteoconductive properties, making it an attractive choice for osteomyelitis, especially in situations where new beads can be easily added (i.e., open wound).34 Antibiotic-impregnated beads can be commercially purchased or easily made. Other antibiotic- impreganated substances (i.e., collagen) exist for treating infections, and these have been occasionally used in large animals although not extensively studied.
REGIONAL LIMB PERFUSION. Regional limb perfusion of antimicrobials is an effective way to deliver a high dose of antimicrobials to an isolated area. For RLP to be effective, it is critical to have adequate venous access, appropriate tourniquet application, and adequate patient restraint. The technique involves a tourniquet placed proximal and distal (or proximal only in cases of distal limb infections) to the site of infection in order to isolate the venous system in the region of the infection from systemic circulation. The tourniquet’s tightness typically occludes the venous system but only partially occludes the arterial system, resulting in a pressurized venous system that allows for antibiotics injected into this system to diffuse into the surrounding tissues and, in some cases, even poorly perfused tissues.26 Vascular access can be obtained by placing a needle or catheter into an accessible vein located between the tourniquets. Alternatively, intraosseous access can be obtained with a cannulated screw or similar device and effective delivery of antibiotic can be obtained with either approach, although there appear to be differences in concentrations achieved when comparing vascular RLP with intraosseous RLP.35,36 The exact volume of perfusate, type of tourniquet, and duration of tourniquet application is still debated.37-42 Although many of these details still need to be optimized, a few points have become more clear: (1) volume of perfusate—it seems clear that higher volumes (60 to 100 mL) result in greater diffusion of antibiotics to the tissues, (2) antibiotic choice—although much work remains here, aminoglycosides are well studied and readily available, and their concentration-dependent action makes this class an excellent choice for RLP, (3) exangunation seems unnecessary, (4) timing of tourniquet application—greater than 20 to 30 minutes is difficult to achieve due to patient factors, and it seems there is minimal difference after 15 minutes, and (5) many other details are debatable and require more work to identify the correct decision.39,43,44 In summary, RLP is an excellent choice for local delivery of antibiotics and should be considered when treating osteomyelitis in large animals.
■ Prognosis The prognosis of osteomyelitis in large animals depends on location of infection, severity of infection, synovial involvement, presence of orthopedic implant, and presence of other comorbidities, especially in neonates. Reports describing survival of adult horses with osteomyelitis vary from 10% to 100% based on many of these factors.6,45 Similarly, reports describing survival and return to function of neonates with osteomyelitis also vary widely.16,46 It is clear that with a prompt diagnosis, consideration of comorbidities, evaluation and management of synovial structures, initiation of appropriate therapy including removal of necrotic and infected tissue, biofilm removal and management, and appropriate use of antimicrobials with an emphasis placed on local delivery techniques, success can be achieved in many cases.