Heel and Foot Pain
Sarah N. Sampson
■ Introduction Lameness associated with the foot is the most common cause of lameness in any type of horse. Predominantly this is lameness affecting the front feet, but there are also a number of horses with hind foot lameness that blocks to the heel and foot.
In this section, heel and foot pain is used due to our inability to specifically localize foot pain to the navicular region with any diagnostic block other than a navicular bursa (NBSA) block. Historically, lameness that blocks to a palmar or plantar digital nerve (PDN) block (aka “heel block”) was called navicular disease. However, this term was changed to navicular syndrome once it was realized that the navicular bone is only one of many structures affected in horses that blocked to a PDN block. These navicular syndrome horses are now referred to as “heel pain” or “foot pain” horses, because we realize that a PDN block is not just blocking the navicular region. In 1996, when we started evaluating the feet of live horses with MRI, it became evident that the PDN block was actually resulting in anesthesia of many structures in the foot other than those in the navicular region. It is important to realize that in this section on heel and foot pain, all of the structures listed below can be anesthetized with a PDN block due to proximal diffusion of the block and the variable range of anesthesia achieved with this block. Depending on diffusion, it is also possible in some instances to block structures in the fetlock region.1. Distal aspect of first phalanx
2. Middle phalanx
3. Distal phalanx
4. Collateral cartilages
5. Navicular bone (distal sesamoid bone)
6. Oblique and straight distal sesamoidean ligaments
7. Proximal and distal digital annular ligaments
8. Deep digital flexor tendon
9. Superficial digital flexor tendon branches
10.
Collateral sesamoidean ligament (aka navicular suspensory ligament)11. Distal sesamoidean impar ligament
12. Collateral ligaments (proximal and distal interphalangeal joints)
13. Proximal interphalangeal joint
14. Distal interphalangeal joint
15. Navicular bursa
16. Digital flexor tendon sheath
17. Laminar tissue
■ Pathophysiology The ability to use MRI on live horses has enabled us to obtain a definitive diagnosis in horses with heel and foot pain. Due to the number of different clinical presentations as well as the number of structures that may or may not be affected, the etiology of pathologic change in the heel and foot can vary widely. For example, if a horse has unilateral deep digital flexor tendon (DDFT) pathology in the heel and no other structures are affected, this is likely a traumatic injury. Conversely, if a horse has bilateral DDFT pathology with concurrent navicular bone (NB) pathology and distal sesamoidean impar ligament (DSIL) and collateral sesamoidean ligament (CSL) desmopathy, this is more likely to be a degenerative process with a possible genetic predisposition (Quarter Horses, warmbloods, and Thoroughbreds are overrepresented and Arabians are underrepresented in horses presenting with heel and foot pain).
The exact etiology of NB pathology remains unclear, but a biomechanical theory has the most experimental support at this time and suggests that the degenerative changes in the NB result from abnormal forces exerted on the bone and its supporting ligaments (the DSIL and CSL). The podotrochlear apparatus (NB, CSL, DSIL, NBSA) and the DDFT and distal digital annular ligament (DDAL) are intimately related in the heel region from a biomechanical perspective, and these structures are often affected concurrently. Compression of the distal half of the NB by the DDFT is an important aspect of this theory. The greatest forces to the NB are applied during the propulsion phase of the stride, during extension of the distal interphalangeal joint (DIJ) just prior to toe off.
The DDFT, CSL, and DSIL act to stabilize the DIJ as they are put under tension during the propulsion phase. The biomechanical force applied to the NB depends on hoof conformation and is increased in horses with low heels and decreased in horses with more substantial heels. There are also cases in which unilateral NB pathology can be due to a traumatic event, although this is much less common. There are also a number of very young Quarter Horses (complaints and/or complaints of intermittent forelimb lameness. Often these horses will have had one or more episodes of acute, obvious lameness that then improves quickly, and they are able to continue in performance for a limited period. Sometimes these horses are thought to have a foot abscess, but no drainage is seen and the horse improves temporarily. Horses with heel and foot pain may become more lame toward the end of the trimming and shoeing cycle and/ or may be “tenderfooted” right after trimming and shoeing. Owners may also complain of stumbling, stiffness in the front end, pointing one front foot, and/or a shortened, choppy stride. A common history is that the horse was out of work and confined to a stall for some other reason and then was observed to be lame on one or both forelimbs on resumption of work.Acute injuries in the heel and foot can present with a history of acute lameness during an event or when brought out of the stall or pasture. They may have improved partially with rest or not improved at all. However, with any riding or exercise, the lameness typically worsens again. As noted previously, owners may think the horse has a foot abscess and manage it accordingly until it becomes evident that the horse is not improving or the lameness continues to recur. With bilaterally lame horses, owners often think shoulder lameness exists because the horses move very stiffly. Also, horses with severe pathology can present similarly to a laminitic horse with slightly elevated pulses and a “walking on eggshells” look.
It is important to perform a complete radiographic evaluation that includes a navicular skyline view, particularly if the horses are not sensitive over the toe to hoof testers.■ Diagnosis
CLINICAL EVALUATION. Clinical evaluation of any horse presenting for lameness begins with a thorough physical examination. The physical exam will often be normal in these horses, but some horses may have slightly increased digital pulses on the affected limbs and some horses may have palpable DIJ effusion on the affected limbs. Horses with DDFT and/ or DDAL pathology in the pastern region may have thickening palpable in the palmar or plantar pastern. Abnormalities in hoof conformation are noted in many horses, but there is no correlation between the types of pathology seen within the foot and types of hoof abnormalities involving the internal structures of the foot. Horses with perfect feet can have the same pathology as horses with poorly conformed feet.
Hoof tester evaluation can be done either before or after the motion exam. Heel and foot pain horses may be negative to hoof testers, or they may have sensitivity in any area of the foot, although most commonly over the mid-frog region and heels. Hoof tester evaluation is a standard part of the lameness exam, but it does not correlate well with the type of pathology present in the foot and it is very important to remember that a negative hoof tester exam does not rule out foot pain. The hardness of the hooves, the thickness of the sole, and whether the horse is stoic can all influence whether the horse will respond to hoof tester pressure applied to the foot. Based on a group of bilateral forelimb lame horses that blocked to a PDN block, no correlation between hoof tester evaluation and MRI findings in the foot was found.1
LAMENESS EVALUATION. The lameness evaluation should be performed on smooth, hard ground. More severely affected horses can be lame at a walk (mildly lame to severely lame, depending on the pathology present).
However, most horses with heel and foot pain will be sound at a walk and have mild to moderate lameness at a trot in a straight line. Horses that have a very symmetric, bilateral lameness may not look lame at a trot in a straight line but will be “choppy” or short strided.Circling these horses with the lame limb on the inside of the circle will commonly exacerbate the lameness when compared to movement in a straight line. Circling these horses with the lame limb on the outside of the circle may reveal lameness in the limb that is now on the inside of the circle. For example, a horse that is right front lame in a straight line may have an exacerbated right front lameness when circling to the right but then show a left front lameness when circling to the left. If a horse is unilaterally lame, it may show the same unilateral lameness in all directions.
Flexion tests performed on horses with heel and foot pain will often be positive to lower limb flexion. Occasionally the limb contralateral to the one being flexed will show increased lameness after flexion.
DIAGNOSTIC ANESTHESIA. Localizing pain to the heel, foot, or pastern is commonly done with a palmar digital nerve block (1.5 to 2.0 mL/nerve). However, determining which structures are the source of pain can be challenging. It seems that the more we learn about diagnostic anesthesia, the more clouded the picture becomes. We used to believe that a PDN block localized the lameness to the heel or sole region, but this is not the case. Structures associated with the coffin joint, hoof wall, and pastern can also be desensitized with this block, depending on the amount of anesthetic diffusion that occurs.
The location of the lameness in the foot or pastern can be further defined using a DIJ (coffin joint) block, NBSA block, and/or digital flexor tendon sheath (DFTS) block in the lameness workup. When using these blocks, it is important to realize that a DIJ block can anesthetize the navicular region and a DFTS block can anesthetize some DDFT lesions within the proximal aspect of the foot.
The NBSA block is the most specific block for navicular area pain, but it is also the most time consuming, so it is often not performed in a typical lameness evaluation. A positive response to NBSA block most likely reflects pathology in the navicular bursa, navicular bone, or supporting ligamentous or tendinous structures. Once the lameness has been localized to the pastern or foot region, diagnostic imaging is performed to attempt to identify the definitive cause of lameness.■ Diagnostic Imaging
RADIOGRAPHY. A minimum of three high-detail radiographic views should be used to evaluate the foot (lateromedial, 60-degree dorsoproximal-palmaro/plantarodistal oblique, and palmaro/plantaroproximal-palmaro/plantarodistal oblique [navicular skyline]), with additional views including a horizontal dorsopalmar view and a dorsomedial and dorsolateral 45-degree oblique view of the navicular bone and distal phalanx palmar processes. Examples of abnormal radiographic changes in the navicular bone include variation in size and shape of the synovial invaginations, cystic changes within the medullary cavity, enthesophyte formation at the wings, flexor cortical erosion, loss of corticomedullary distinction, sagittal fracture, distal border remodeling, and proximal and distal border fragments. Horses that block to a PDN block may have pathology in other bones in the pastern or foot. Examples of pathology seen in the distal phalanx include fracture, pressure necrosis from a keratoma, osteolysis, bone cyst, osteochondral fragment, and osteoarthritis associated with the DIJ. Pathologic changes can also be seen in the proximal and middle phalanges that can potentially block to a PDN block and can include bone cyst, osteoarthritis of the proximal interphalangeal (PIP) joint, and osteochondral fragments. Ossification of the collateral cartilages of the distal phalanx is common and can be associated with lameness, particularly if there is a fracture at the base of the ossified collateral cartilage. Mineralization of the soft tissue structures within the foot or pastern may also be identified and is most commonly seen associated with the DDFT just proximal to the navicular bone.
Previous studies have shown that variations in synovial invagination size and shape correlate poorly with lameness, rarely progress over time, and are inconclusive for the diagnosis
of navicular bone degeneration. Radiographic abnormalities more strongly associated with lameness and relevant navicular bone degeneration include flexor cortical erosion (Fig. 38.23) and loss of the corticomedullary junction (e.g., medullary sclerosis) (Fig. 38.24). Navicular bone distal border fragments are more common, and the flexor cortex is thicker in horses with navicular pathology.2 Although radiographic evaluation
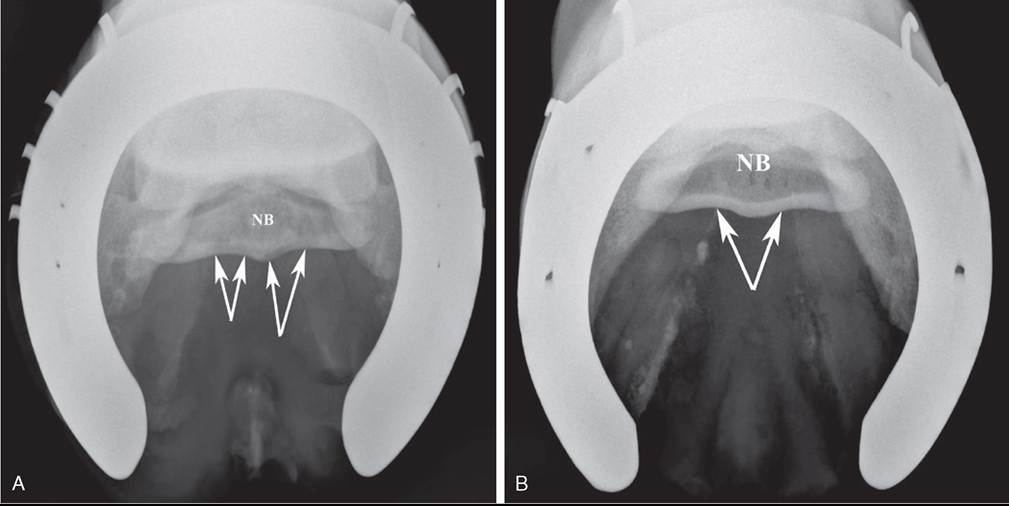
FIG. 38.23 Navicular skyline radiographic projections highlighting the flexor cortex and medullary cavity of the navicular bone (NB). A, Arrows point to two flexor cortical erosions on the flexor cortex of the NB, which is indicative of severe NB degeneration. B, Arrows point to a normal flexor cortex of the NB.
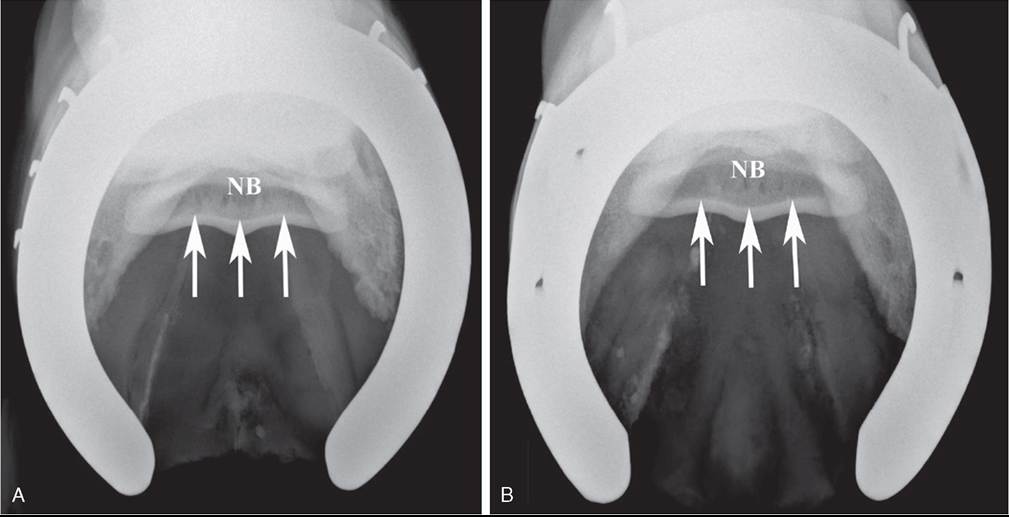
FIG. 38.24 Navicular skyline radiographic projections highlighting the flexor cortex and medullary cavity of the navicular bone (NB). A, Arrows point to the corticomedullary junction where there is loss of distinction between the flexor cortex and the medullary cavity. This is indicative of NB degeneration. B, Arrows point to a very distinct corticomedullary junction in a normal horse.
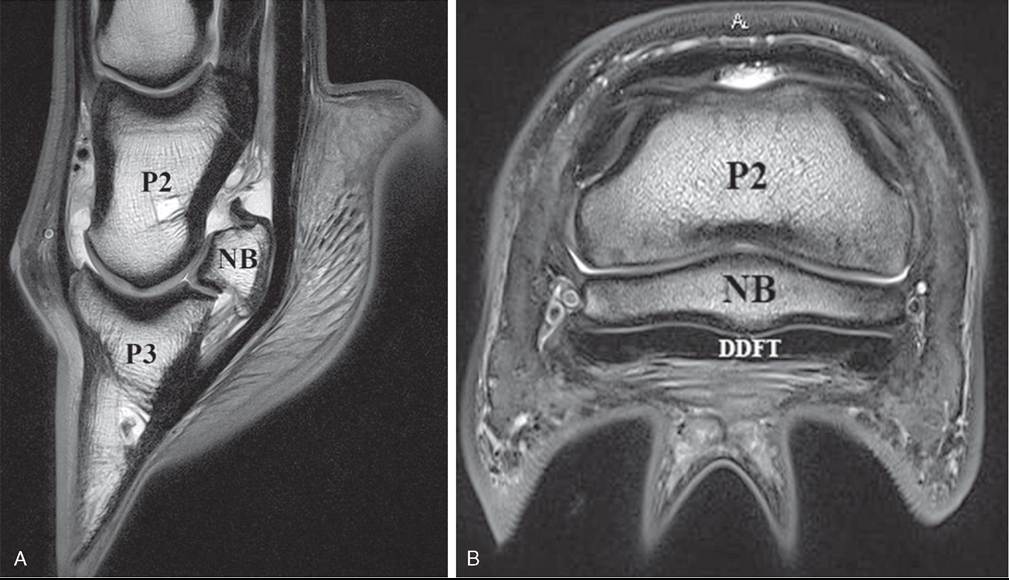
FIG. 38.25 Magnetic resonance images of the foot of a horse. A, Sagittal midline image of the foot. B, Transverse image of the foot at the level of the navicular bone (NB). DDFT, Deep digital flexor tendon; P2, middle phalanx; P3, distal phalanx.
is important in the diagnostic workup of a horse showing heel and foot pain, it is not always very sensitive in defining the actual pathologic condition of the NB. Radiographs often underestimate the extent of pathology seen on necropsy in horses with navicular lesions, and many horses with lameness localized to the foot have normal radiographs even though they have multiple bone and soft tissue lesions on MRI.1
ULTRASONOGRAPHY. Ultrasonography can be used to assess the structures of the pastern circumferentially, which includes the DDFT, superficial digital flexor tendon (SDFT), distal sesamoidean ligaments, proximal digital annular ligament, proximal aspect of the DDAL, proximal aspect of the DIJ collateral ligaments, collateral ligaments of the PIP joint, and periphery of the first and second phalanges.
Within the foot, ultrasonography can variably identify effusion of the NBSA, the CSL, and the proximal margin of the NB when imaged through the heel bulbs. This is very dependent on the heel conformation of the horse and access to a microconvex probe that can fit in between the heel bulbs of the horse. If the frog is pared down and the foot is soaked in water for 24 hours, a thin window on midline that is imaged through the frog can be assessed using ultrasound. If the frog is excessively hard or has a deep sulcus, poor contact between the frog and transducer may prevent propagation of the ultrasound beam.3 Unfortunately, the images obtained through the frog are difficult to interpret, and ultrasonographic findings do not correlate well with pathologic findings on MRI. The structures partially visible in this transcuneal ultrasound window include the axial aspect of the navicular bone flexor surface, distal portion of DDFT, DSIL, and palmar aspect of the distal phalanx.3
MAGNETIC RESONANCE IMAGING. Magnetic resonance imaging is the gold standard in orthopedic imaging evaluation. This modality can assess both the bone and soft tissue structures of the distal limb (Fig. 38.25). It uses hydrogen protons in the body that align with the external magnetic field to assess tissue at a molecular level. Perturbation of the hydrogen atoms within the body using a radiofrequency pulse results in a grayscale image of the anatomic area imaged. Pathologic change that is not visible with ultrasonography or radiography can be identified with MRI. In regard to the foot of the horse, MRI provides a look at the internal structures of the foot that is not possible with other imaging modalities. It is used for horses with heel and foot pain when a diagnosis cannot be made with radiographs or ultrasound or when nuclear scintigraphy localizes pathology to the foot. However, many owners also request MRI in order to more fully evaluate the foot or pastern (1) to determine if there are more than one issues, (2) to further define the severity of a previously diagnosed lesion, or (3) as a component of a prepurchase evaluation. For a definitive diagnosis in a horse with heel and foot pain that has an unremarkable radiograph and ultrasound evaluation, an MRI is the next diagnostic step.
Horses can be imaged in either high- or low-field-strength magnets. The higher the field strength (T; Tesla), the better the image resolution and the faster the image acquisition. All high-field magnets (≥1 T) require general anesthesia so that the horse's limbs can be placed in the bore of the magnet. Low- field magnets (≤0.3 T) can be either “standing” magnets, where the horse is sedated but standing during imaging, or magnets that require the horse to be anesthetized for the images to be acquired. The low-field, standing magnets produce the lowest- quality and lowest-resolution images due to the inherent movement of a standing horse. Motion correction software is used to decrease the image degradation, but it is not enough to make the image as clear as those obtained from a horse that is anesthetized for image acquisition. High-field-strength magnets have better-quality and better-resolution images, which is directly related to the field strength of the machine. High- field magnets are also much more costly to purchase, but the cost to the client to image a horse is often similar between high- and low-field magnets.
NUCLEAR SCINTIGRAPHY. Nuclear scintigraphy in the horse involves intravenous injection with a radiopharmaceutical that is labelled to phosphorous and concentrates in areas of high bone turnover. This radiopharmaceutical emits gamma rays that are captured by a gamma camera during the procedure. In regard to the foot, if the navicular bone is undergoing active bone remodeling, the radiopharmaceutical will be concentrated in the navicular bone, and this will be evident on the images obtained. Increased radiopharmaceutical uptake in the foot is a good predictor of pathology, but a negative scintigraphic result does not exclude the presence of significant pathology.4,5 Nuclear scintigraphy has been shown to have a high specificity but low sensitivity for detection of lesions of the NB, DDFT, and collateral ligaments of the DIJ when compared to MRI.4,5 Nuclear scintigraphy can help determine the significance of pathology found with MRI, particularly if more than one structure is affected and the clinical relevance of a specific lesion is questioned.
COMPUTED TOMOGRAPHY. Computed tomography units used for horses typically involve general anesthesia, but a small number of units that can image the standing horse are being used now.
CT is used much less commonly than MRI for evaluation of the foot of the horse. It is excellent for detecting and evaluating bone pathology in the cortex or trabecula (fractures, sclerosis, peripheral remodeling), but it provides inadequate soft tissue detail when compared to MRI. It is based on density of tissue, similar to radiographs, and can show excellent peripheral bone detail, particularly for bone fragmentation, that is better than MRI, but MRI shows better internal detail of bone overall. Although less expensive than MRI, CT is less versatile and is most commonly used to assess fracture configuration or peripheral lesions of bone. CT is also used to guide some orthopedic injections and some complicated surgical procedures.
■ Treatment There are numerous treatment options for horses with heel and foot pain. However, unfortunately many treatment options are only palliative, not curative. Horses with pain localized to the foot but without a definitive diagnosis will be treated based on the veterinarian’s clinical evaluation and best guess as to the cause of the lameness. This decision will also take into consideration the use of the horse, the financial constraints of the owner, and any other concerns or constraints based on the individual horse-owner pair. When a definitive diagnosis is available, treatment is tailored to the structures affected, with the hope that by treating the specific cause of lameness, the prognosis for return to performance will be increased.
■ Medical Management
REST AND REHABILITATION. Injuries to the pastern or foot region that will most likely involve a rest and rehabilitation program include, but are not limited to, fracture, acute tendon injury, acute ligament injury, bone bruise (“edema”), and acute laminar inflammation. Depending on the structure affected and the severity of the lesion, the rest period could last from 3 to 12 months, and this is why a specific diagnosis is so important. Typically these types of lesions do not resolve with “pasture” rest, and stall or small paddock confinement is needed at the beginning of the rest and rehabilitation program. Conversely, standing a horse in a stall for 6 months is also not a reasonable rehabilitation program. When horses are rehabilitated after an injury, they should be in a controlled environment that limits their free exercise (typically a stall initially, then a small paddock, and then a larger paddock). During this confinement, it is important that the force the horses put on their limbs slowly increases in a controlled manner. A gradual increase in workload is done using hand walking, jogging in hand, and in some horses, using specific types of rehabilitation equipment based on the particular injury.
A recent study looking at 118 cases of primary DDFT injury in the pastern or foot region found that prognosis for return to use depended on injury severity, presence of concurrent injury to other structures in the foot, type of activity, and owner compliance with specific treatment recommendations.6 Specifically, horses treated with intrasynovial corticosteroid injections and 6 months of rest and rehabilitation returned to use for a significantly longer duration than did horses treated without a rest period.6 Also, Western performance horses returned to use for a significantly longer duration than English performance horses.6
FARRIERY. Therapeutic trimming and shoeing to reduce biomechanical forces on the heel region is a very important part of treatment for horses with foot and heel pain. Most often, horses will improve somewhat after corrective shoeing if they are not already shod appropriately, but they still require additional treatment to get them back in performance. The goals are to (1) restore hoof balance, (2) improve existing problems such as underrun heels, (3) reduce biomechanical forces on the heel region, and (4) protect injured areas of the foot. Although there is no standard shoeing technique for horses with heel pain, observing abnormalities in the hoof and lower limb and following basic principles can often accomplish these four goals. Proper trimming alone may restore correct hoof balance such that special shoes or pads are unnecessary. Even with proper trimming, however, many horses still require special shoes or pads to achieve the desired breakover and heel support, as well as offer protection to the bottom of the foot. The veterinarian, farrier, and owner must work together and consider the horse’s hoof shape and hoof wall quality, environment, conformation, use, and severity of disease.
The configuration of the hoof capsule reflects the stresses applied to the foot during the previous year. Hoofbalance refers to both mediolateral and dorsopalmar balance. Dorsopalmar balance refers to proper hoof-pastern alignment. Ideally, when viewed from the side, a line drawn through the central aspect of the first phalanx should bisect the hoof capsule, and the toe angle and heel angle should be parallel to this line. A broken back hoof-pastern axis is common in horses with long toe-low heel conformation and results in increased stress on the phalangeal joint capsules, navicular suspensory apparatus, and distal DDFT and increased pressure between the NB and DDFT.
Breakover (breakover point) of the foot is the terminal part of locomotion when the heel loses contact with the ground surface, followed by the toe. Breakover point on the bottom of the foot can be determined by finding the last point of contact of the foot or shoe with the ground near the front of the foot. A low heel angle and/or a long toe is associated with prolongation of breakover time. A high heel angle reduces breakover, causing a reduction in the forces exerted on the palmar and plantar structures of the foot and limb (e.g., navicular suspensory apparatus, DDFT).
Corrective trimming is often more important but can be more difficult than corrective shoeing. The toe is shortened as much as possible, and the heels are trimmed back to the widest aspect of the frog. Proper heel trimming (back to the widest aspect of the frog) increases the functional weight-bearing surface of the foot. The ground surface of the properly trimmed foot has a more rounded appearance. Palmar and plantar hoof support is essential for horses with heel pain. Full-fitting shoes provide more support by increasing the weight-bearing surface. Using a wedged shoe or pad to elevate the heels by 2 to 3 degrees after the foot is properly trimmed has been shown to decrease tension in the DDFT, reducing pressure applied to the heel region. However, each horse is an individual, and the shoeing should be tailored to each horse and adjusted, if needed, at each shoeing cycle.
NONSTEROIDAL ANTIINFLAMMATORY DRUGS (NSAIDS). Phenylbutazone is the most common NSAID used to decrease the pain associated with lameness in the foot region. It reduces pain by inhibiting the enzyme cyclooxygenase and the subsequent cascade of prostaglandins. The recommended dosage depends on individual horse needs and severity of disease. An initial dosage of 4.4 mg/kg daily as needed for lameness can be used. Often this is used in the first 1 to 2 weeks following joint injections or shoeing changes. Many horses will require additional treatment during competition if medication rules allow and the lameness is not fully resolved with other medical treatments. Horses that are retired due to lameness that is performance limiting can be treated with low to moderate dose (2.2 to 4.4 mg/kg) phenylbutazone as needed to help with chronic pain.
IsoxsUPRINE HYDROCHLORIDE. Isoxsuprine hydrochloride is a drug that causes vascular smooth muscle relaxation and may increase blood flow to the foot. Its absorption after oral (PO) administration in the horse is erratic, and its usefulness is questioned. The recommended dose of isoxsuprine is 0.6 mg/ kg PO twice daily for 3 weeks; if no response is seen, the dose is increased to 1.2 mg/kg PO twice daily for 3 weeks, then once daily for 3 weeks, then every other day for an additional 3 weeks. No adverse drug reactions have been reported. At this time, isoxsuprine is not commonly used in the treatment of heel and foot pain due to the lack of evidence of efficacy.
INTRAARTICULAR MEDICATIONS. There are three synovial structures associated with the foot that can be accessed and used as a route for intraarticular medication: distal interpha- langeal joint, navicular busa, and digital flexor tendon sheath (Fig. 38.26).
The distal interphalangeal joint can be medicated when there is pathology associated with the joint itself or its associated collateral ligaments. However, the DIJ also covers the dorsal surface of the CSL and DSIL, as well as the proximal, dorsal, and distal aspects of the NB where the synovial invaginations of the NB are actually contiguous with the DIJ.7 Furthermore, triamcinolone acetonide that is injected into the DIJ in normal horses has been shown to diffuse into the NBSA in all instances.8 Due to the broad coverage by the DIJ, this is often the first synovial structure medicated in horses when they are diagnosed with foot pain but do not have a definitive diagnosis. Since the DIJ is a high-motion joint, most veterinarians are injecting triamcinolone acetonide and hyaluronic acid into this synovial structure when treating horses with heel and foot pain.
The navicular bursa is medicated when (1) DIJ injections fail to improve the horse for a reasonable period of time, (2) there is pathology associated with the flexor cortex of the NB, (3) there is navicular bursitis, or (4) dorsal DDFT pathology is known or suspected. Navicular bursa injection should be done with radiographic guidance, and therefore this is a slightly more involved procedure than DIJ injection, it takes longer to perform, and it is typically more expensive. The navicular bursa contains fibrocartilage on the back of the NB, but no hyaline cartilage is present, thus practitioners will use either triamcinolone acetonide or methylprednisolone acetate in combination with hyaluronic acid when injecting the navicular bursa.
The digital flexor tendon sheath is medicated when pathology within it or in association with the sheath is known or suspected. Examples of pathology within the pastern or foot that may respond to DFTS injection include DDFT pathology within
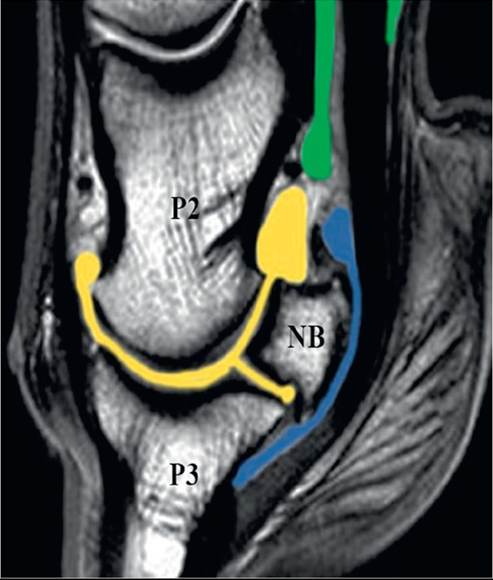
FIG. 38.26 Sagittal midline magnetic resonance image highlighting the boundaries of the distal interphalangeal joint (yellow), navicular bursa (blue), and digital flexor tendon sheath (green). Dorsal is to the left. NB, Navicular bone; P2, middle phalanx; P3, distal phalanx.
the sheath, SDFT branch tendinopathy, DDAL desmopathy,9 and oblique and straight distal sesamoidean desmopathy.10 Practitioners will most commonly use either triamcinolone acetonide or methylprednisolone acetate in combination with hyaluronic acid when injecting the DFTS.
A recent study evaluated 101 horses with clinical signs of heel pain that underwent MRI evaluation and had the NBSA medicated based on MRI findings associated with that region.11 Seventy-six of 101 (75%) horses returned to their intended use for a mean of 9.6 months. Horses that had been lame for less than 6 months had a significantly better chance of returning to intended use than horses that had been lame more than 6 months.11 Horses with primary DDFT pathology that had NBSA injections and were put through a 6-month rest and rehabilitation program responded for the longest period. If the DDFT pathology extended into the area of the DFTS, this synovial structure was also medicated. Horses with scar tissue and adhesions between the DDFT and CSL or horses with adhesions between the NB and DDFT were treated with pressurization of the NBSA with 30 to 50 mg of hyaluronic acid in an attempt to break down adhesions, but these horses were less likely to have a positive response to therapy.11 Horses with multiple structures affected in the heel region were also less likely to respond well to treatment.11
HYALURONAN. Hyaluronan (HA) is a normal component of synovial fluid and functions as a boundary lubricant within the joint. It also appears to have some antiinflammatory properties, but the exact mechanism is unknown. Exogenous HA inhibits chemotaxis and phagocytosis of granulocytes, reduces the stimulation of lymphocytes, and has been shown to decrease prostaglandin E2 synthesis by cultured equine synoviocytes if given intraarticularly but not systemically.12 The antiinflammatory properties of HA appear to be dose dependent, and HA with a molecular weight greater than 500,000 Daltons may be more effective. The effect of systemic HA on pathology within the pastern or foot region is unknown. The recommended dose is 40 mg intravenously once weekly for 3 weeks, then once monthly for maintenance, but there is not substantial research in the literature at this time regarding HA administration systemically.
POLYSULFATED GLYCOSAMINOGLYCANS. Polysulfated glycosaminoglycans (PSGAGs) are referred to as Chondroprotective agents and have antiinflammatory properties. They decrease IL-1 and prostaglandin E2 and directly inhibit MMPs, proteinases, lysosomal enzymes, collagenase, and stromelysins. If given intraarticularly, they potentiate infection; therefore they must be given with an intraarticular antibiotic. PSGAGs given as 500 mg intramuscularly every 4 days for 7 treatments have been shown to provide positive effects (decreased joint circumference, greater carpal flexion) in a controlled study of equine carpitis.13
BISPHOSPHONATES. Biphosphonates are a class of drug that inhibits osteoclasts and are used in human medicine to treat osteoporosis. Bisphosphonates have not yet been shown to have the same inhibitory effects on osteoclasts at the doses used in horses.14 The two bisphosphonate medications used commonly in horses are tiludronate (intravenous) and clodronate (intramuscular). One study has shown improvement in lameness using a 1 mg/kg dose of tiludronate when assessing horses with lameness that blocked to a PDN block and in which the horses had radiographic evidence of navicular bone degeneration.15 At this time, the improvement in lameness seen with bisphosphonates is thought to be due to an antiinflammatory effect and not a bone remodeling effect.
EXTRACORPOREAL SHOCKWAVE TREATMENT. Investigated as a treatment for navicular bone degeneration in horses, extracorporeal shock wave treatment (ESWT) directs a pressure wave to a specific area of the body to increase osteogenic activity in bones and induce neovascularization. A single ESWT applied to the frog and heel bulb region does not influence lameness in horses with navicular bone disease.16 ESWT over three treatments had no effect on pre- and postscintigraphic or radiographic images of the heel region.17 In a study looking at collateral desmopathy of the DIJ, there was no effect of ESWT on outcome.18 At this time, the benefit of EWST on pathology in the foot needs further investigation.
■ Surgical Treatment
PALMAR/PLANTAR DIGITAL NEURECTOMY. Palmar/plantar digital (PD) neurectomy is a surgical procedure that removes a section of the medial and lateral PDN between the fetlock and heel bulbs. This typically abolishes sensation in the heel and sole region of the foot. This procedure is an option for horses that block to a PDN block and are nonresponsive to medical management, with no other viable treatment options available. In a recent report in which MRI was used to guide treatment, 92% of horses responded favorably to PD neurectomy, with 80% able to return to their previous level of work for a median time of 20 months (range: 12 to 72 months).19 Postoperative complications, including residual lameness, painful neuromas, or early recurrence of lameness, occurred in 36% of these horses.19 Horses with DDFT pathology within the foot or pastern region are not good candidates for this procedure because they experience residual lameness or early recurrence of lameness after PD neurectomy.19 Horses with other foot lesions or only dorsal border lesions of the DDFT had a better response to surgery.19 In another study, 88% of horses were sound for at least 1 year after PD neurectomy.20 Magnetic resonance imaging is used frequently to determine if DDFT

FIG. 38.27 Transverse magnetic resonance image of a horse with a portion of the deep digital flexor tendon torn and protruding (arrow) into the navicular bursa. Dorsal is to the top.
pathology is present, and if so, these horses are not considered good candidates for a PD neurectomy.
NAVICULAR BURSOSCOPY. Navicular bursoscopy is being used more often as a treatment option now that we are able to use MRI on horses and determine optimal candidates for this procedure. Optimal candidates include horses that have a primary navicular bursitis with a mild to moderate amount of fibrinous or fibrous tissue within the proximal NBSA, as well as horses that have lesions located along the dorsal border of the DDFT at the level of the proximal NBSA (Fig. 38.27). This surgical procedure allows direct visualization of pathology within the proximal NBSA, along the dorsal border of the DDFT, and along the NB flexor cortex. This procedure also enables removal of scar tissue from within the NBSA and debridement of DDFT fibrils extruding from the dorsal border due to a tendon tear. In a recent study of 92 horses undergoing navicular bursoscopy, 61% returned to work and were sound, and 42% returned to their previous level of performance.21 Horses in this study that had extensive tearing and combination injuries of the DDFT and navicular bone identified with MRI had poor outcomes.21
COLLATERAL SESAMOIDEAN DESMOTOMY. This procedure involves transection of the branches of the CSL, which is the ligament that suspends the NB from the middle phalanx. When this procedure was first developed, these branches were transected at the lateral aspect of the middle phalanx through skin incisions.22-24 In the first study, 13 of 16 (81%) horses were able to work without lameness after the procedure.22 In the second study, 76% of horses were sound at 6 months, and 42% of horses were sound at 36 months.23 In the third study, 12 of 17 (70%) horses were sound at 6 months following surgery.24
More recently, a procedure was developed to transect the CSL branches from within the palmar pouch of the DIJ using arthroscopic guidance.25 This technique provides the ability to verify full transection of the ligament by visualization of transection and increased movement of the NB away from the middle phalanx. Collateral sesamoidean desmotomy is performed when pathology associated with the suspensory apparatus (DSIL, NB, CSL) of the foot has been diagnosed but no flexor cortical erosion is present. In addition, other causes of lameness that would preclude the horse from responding positively to CSL desmotomy (e.g., DDFT pathology, navicular bursitis) need to be ruled out. Due to the specific diagnosis needed, MRI is highly recommended to determine whether this procedure would be a viable treatment option. Unfortunately, at this time there are no published reports of response to treatment using MRI as a screening tool. The hope is that by using MRI to define optimal candidates for this treatment, the prognosis for return to performance may be improved.
■ Summary No single treatment option is suitable for all horses with heel and foot pain. Each horse must be evaluated individually so that the structures affected, severity of disease or injury, use of horse, level of performance, and financial constraints are determined and used to guide treatment. Many treatment options are available to help these horses return to performance, but treatment can be much more successful in horses in which a definitive diagnosis has been obtained so that treatment is tailored to the individual horse. Magnetic resonance imaging is the best diagnostic tool we have to identify pathology within the foot of horse, and it should be used if at all possible to determine the cause of the lameness.