Pancreatitis
Introduction and definitions
Pancreatitis describes pancreatic inflammation. It is the most common exocrine pancreatic disease in both dogs and cats. In an older study from Europe, histopathological evidence of pancreatitis was found in 1.0% of 9,342 canine pancreata and 0.6% of 6,504 feline pancreata.9 However, recently, it has been suggested that the true prevalence of pancreatitis is by far greater.
In one study, more than 21% of 73 dogs undergoing necropsy at the Animal Medical Center in New York City had macroscopic lesions suggesting pancreatitis.10 Pancreata from all 208 dogs were sectioned every 2 cm and a total of 64% had histological lesions of acute and /or chronic pancreatitis (Figure 8.3).11 In another study, 25.6% of 200 unselected dogs submitted to necropsy through a group of first-opinion practices in the UK showed evidence of chronic pancreatitis and 2.0% showed evidence of acute pancreatitis.12 These data suggest that pancreatitis is far more common in dogs than previously suspected. However, the data also suggest that infiltration of the pancreas with inflammatory cells is not necessarily clinically significant and more research is needed to characterize clinically significant disease better.Similar data have recently been reported for cats.13 In a study of 115 cats submitted for necropsy at the University of California in Davis that had three biopsies collected (one from the left limb, one from the right limb, and one from the body of the pancreas), 67.0% showed lesions suggestive of acute and / or chronic pancreatitis (Figure 8.4).13 This would suggest that, similarly to dogs, feline pancreatitis is far more common than previously expected, but also that more work is needed to clearly characterize clinically significant disease.
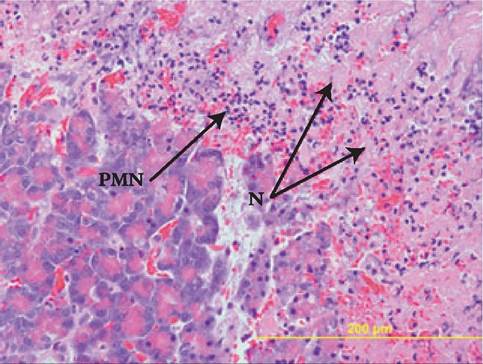
Figure 8.5:
Acute pancreatitis.
This image shows a section of pancreas from a dog with acute pancreatitis. Note the marked necrosis (N) of the acinar cells and the infiltration of the pancreatic tissue with neutrophils (PMN). (H&E, 40?; image courtesy of Dr. Shelley Newman, University of Tennessee, USA.)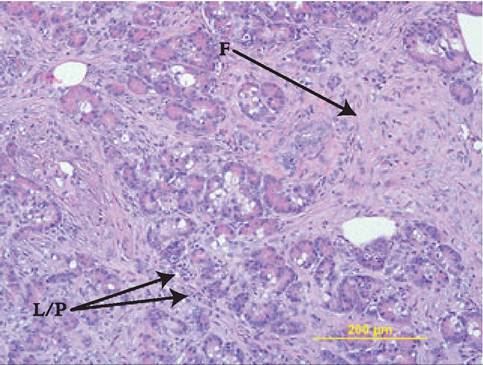
Figure 8.6:
Chronic pancreatitis. This image shows a section of pancreas from a dog with chronic pancreatitis. Notably, there is pancreatic acinar atrophy, evidenced by the lack of pancreatic acinar cells and abundant infiltrative fibrosis (F). Scattered infiltrates of lymphocytes and plasma cells (L/P) are also seen. (H&E, 20?; image courtesy of Dr. Shelley Newman, University of Tennessee, USA.)
As is the case with other organs, pancreatic inflammation can be classified based on different parameters. In human medicine, several international conferences have been held to arrive at an internationally agreed upon multi-disciplinary classification system for pancreatitis.14 This system was last updated in Atlanta in 1993.14 Because a similar classification system is not available for veterinary medicine, the author generally adheres to this human classification system. However, it should be pointed out that this classification system sometimes stands in contrast to the definitions used by other authors. In general, pancreatitis is divided into acute and chronic pancreatitis.14,15 This classification is exclusively based on the histopathological findings, with acute pancreatitis (Figure 8.5) not being associated with permanent histological changes, while chronic pancreatitis is associated with permanent changes, most importantly, pancreatic atrophy and pancreatic fibrosis (Figure 8.6).15
Both acute and chronic pancreatitis can be associated with local and systemic complications. Local complications include pancreatic necrosis, pancreatic pseudocyst, and pancreatic abscess.
Systemic complications include electrolyte imbalances, acid-base imbalances, DIC, acute renal failure, lung failure, myocarditis, neurological signs (also known as pancreatic encephalopathy), and multi-organ failure. The severity and prognosis of pancreatitis are dependent on the presence of these local and systemic complications.Etiology
The etiology and pathogenesis of pancreatitis is not clearly understood, but there are many risk factors that have been implicated in causing pancreatitis. Miniature Schnauzers have long been recognized as being at an increased risk for pancreatitis, but only recently has a mutation been identified that may be responsible for this increased risk.7 Three mutations of the SPINK gene (i.e., the gene encoding the pancreatic secretory trypsin inhibitor, PSTI), have been identified.7 It is interesting to note that mutations of the SPINK gene, though not the same as the ones that have been identified in the Miniature Schnauzer, are also associated with hereditary pancreatitis in humans.6 There are some other breeds that have also been suggested to be at an increased risk for pancreatitis, including Boxers, Cavalier King Charles Spaniels, Cocker Spaniels, Collies, and Yorkshire Terriers.12,16
Dietary indiscretion, mainly of fatty foods, has anecdotally been blamed for many cases of canine pancreatitis; however, only recently, has a study shown that dietary indiscretion in dogs is in fact associated with a statistically increased risk for pancreatitis in dogs (Foley K, personal communication, 2007). Hyperlipidemia, and more specifically, hypertriglyceridemia, is also considered a risk factor for pancreatitis. In humans, it has been suggested that the risk for pancreatitis is dramatically increased when serum triglyceride concentrations exceed 1,000 mg/dL.17 In a recent study, an increased serum triglyceride concentration above 900 mg/dL was shown to carry an increased risk for pancreatitis in the dog.18
Hypotension and pancreatic hypoperfusion have also been identified as risk factors for pancreatitis and in fact, it has now been speculated that the increased incidence of pancreatitis in human patients undergoing surgery may in fact be caused by pancreatic hypoperfusion, rather than pancreatic trauma.19 Thus, proper fluid support during anesthetic procedures is crucial in maintaining exocrine pancreatic health.
Notwithstanding this, pancreatic trauma (surgical or other) can lead to pancreatitis.19-21 As a consequence, extreme care should be taken when handling the pancreas during a surgical procedure.20Certain infections have also been implicated in causing pancreatitis; however, such infections are extremely rare in dogs. Anecdotal reports of isolated cases of fungal infiltration of the pancreas leading to pancreatitis are available (Newman SJ, personal communication, 2007). In addition, there are only two reports of a bacterial infection of the pancreas in dogs.22,23 In the first report, a pancreatic abscess was diagnosed in six dogs. Klebsiella pneumoniae was cultured in one of these dogs from the area of the pancreas during surgery and Pseudomonas aeruginosa was cultured in a second dog.22 The bacterial cultures were negative in the remaining four dogs.22 In the second report, only two of nine dogs with a pancreatic abscess had a positive bacterial culture.23 Bacterial infections of the pancreas are also extremely rare in cats and have only been associated with a pancreatic abscess in a single cat.24 However, Toxoplasma gondii can infect the feline pancreas. In one study, 38 of 45 cats (84.4%) with toxoplasmosis showed organisms in the pan- creas;25 though, the organisms were limited to the pancreas only in one cat.25 The hepatic fluke, Amphimerus pseudofelineus, can also infest the pancreas of cats and lead to pancreatitis.26 Other infections, including FIP, feline parvovirus, FIV, and FeLV, have all been implicated in causing pancreatitis, but the evidence is limited. In dogs, infection with Babesia canis has been shown to cause pancreatitis.27
Drugs can also cause pancreatitis. In humans, approximately 54 drugs and drug classes have been implicated in causing pancreatitis.19,28 However, demonstration of a cause and effect relationship is difficult and proof of such a relationship has only been demonstrated for a very limited number of agents.29 In dogs, several agents have been implicated, including calcium, L-asparaginase, potassium bromide, phenobarbital, and antimonial drugs for the treatment of Leishmania.8,30 In cats, calcium and organophosphates have been implicated as causing pancreatitis.31 In humans, in comparison, many more drugs have been implicated, including azathioprine, vinca alkaloids, diuretics, and several NSAIDs and antibacterial agents.19,28 However, steroid administration is currently not considered a risk factor for pancreatitis and the treatment of patients with pancreatitis with steroids is not considered to be contraindicated.
Finally, several endocrine disorders, including hyper- adrenocorticism, diabetes mellitus, and hypothyroidism have been identified as risk factors for pancreatitis in dogs.16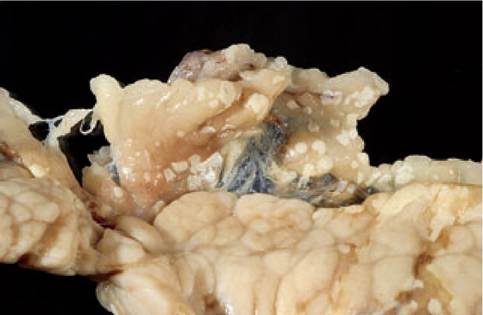
Figure 8.7:
Peripancreatic fat necrosis. This picture shows a canine pancreas with many white raised nodules consistent with peripancreatic fat necrosis. Triglycerides in the tissue surrounding the pancreas are hydrolyzed to fatty acids that then form calcium soaps (saponification). (Image courtesy of Dr. Shelley Newman, University of Tennessee, USA.)
Pathogenesis
Pancreatitis is a complex disease and the pathogenesis is not completely understood. As indicated above, there are many risk factors for pancreatitis. These risk factors ultimately lead to premature activation of the zymogens within the acinar cells, which in turn leads to local damage. Exactly how the enzyme cascade is activated is poorly understood. However, one of the first indicators of ensuing pancreatitis is a decreased secretion of pancreatic enzymes and co-localization of zymogen granules and lysosomes.32 Co-localization of these cellular compartments leads to a decrease in the pH in the newly formed giant vacuoles compared to the zymogen granules, which favors autoactivation of trypsinogen to trypsin. It is also possible that lysosomal enzymes directly activate trypsinogen. Trypsin, if not immediately scavenged, in turn activates more trypsinogen molecules and other zymogens.5 The prematurely activated digestive enzymes then lead to local damage. Phospholipase destroys the phospholipid bilayer of the acinar cells, leading to pancreatic necrosis. Lipase hydrolyzes pancreatic and peripancreatic triglycerides to fatty acids, which fall out as calcium soaps and form yellowish nodules in the peripancre- atic region (Figure 8.7). Kinins are vasoactive polypeptides that can lead to vasodilation and pancreatic hypoperfusion.
Elastase can digest the elastin of the capillaries and lead to bleeding. The local damage then leads to the release of cytokines and recruitment of inflammatory cells. This inflammatory reaction not only leads to further local damage, but also leads to systemic complications, such as hypotension, acid-base abnormalities, DIC, renal failure, lung failure, or multi-organfailure.33 There is some debate of whether some of these systemic complications could also be due to circulating pancreatic enzymes, but most evidence suggests that these systemic complications are mainly due to the inflammatory reaction instead. One exception may be systemic lipodystrophy, which is characterized by disseminated fat necrosis.34 There is little doubt that a lipase is involved in this process and it has traditionally been assumed that pancreatic lipase is the causative factor. However, this has not been verified experimentally.
Clinical presentation
In one study of 70 dogs with fatal pancreatitis (i.e., dogs that either died of their disease or were euthanized because of the severity of their disease), the most common clinical signs reported were anorexia (91%), vomiting (90%), weakness (79%), abdominal pain (58%), dehydration (46%), diarrhea (33%), and fever (21%).35 In comparison, a recent compilation of 159 feline pancreatitis cases reported anorexia (87%), lethargy (81%), dehydration (54%), weight loss (47%), hypothermia (46%), vomiting (46%), icterus (37%), fever (25%), abdominal pain (19%), and diarrhea (12%) as the most common clinical signs.36 According to these reports, abdominal pain, one of the key clinical signs of pancreatitis in humans, is reported much less frequently in dogs and cats than in humans. While one could stipulate that dogs and cats with pancreatitis are less commonly affected by abdominal pain than are humans, the author believes that it is far more likely that abdominal pain is not accurately identified in small animals. As a consequence, the author strongly believes that abdominal pain should be suspected in all small animal patients diagnosed with pancreatitis. Some patients may not show any obvious evidence of abdominal pain, but others may show classical signs of severe abdominal pain. One such example in dogs is the so-called prayer position (Figure 1.7). Generally, cats appear to have far fewer specific clinical signs than dogs. This may be due to the fact that cats more commonly have mild chronic pancreatitis rather than the more severe forms.
As stated above, diarrhea has been reported to be a fairly common clinical sign in dogs with pancreatitis and has also been observed in some cats with pancreatitis.35,36 Thus, pancreatitis should be considered as a differential diagnosis in dogs and cats with diarrhea.
Diagnosis
Routine clinical pathology
Routine clinical pathology testing, including CBC, serum chemistry profile, and urinalysis often show mild or nonspecific changes.31,35 More severe changes can be observed in patients with severe forms of pancreatitis that are affected by systemic complications. Thus findings on routine blood work are not useful for the primary diagnosis of pancreatitis, but should be used as an indicator of the overall health status of the patient.
In a study of 70 dogs with severe pancreatitis, thrombocytopenia was the most common finding on CBC and was reported in 59% of the cases.35 A neutrophilia with a left shift (55%) and anemia (29%) were also frequently observed. Neutropenia was only rarely observed (3%).35 In 40 cats with severe pancreatitis, findings on CBC included anemia (26%), hemoconcentration (13%), leukocytosis (30%), and leukopenia (15%).31
A routine serum chemistry profile may show mild elevations of hepatic enzymes.31,35 Electrolyte abnormalities are commonly seen in severe cases and are due to dehydration and severe vomiting. Azotemia can be seen and may be due to dehydration or may be an indicator of acute renal failure secondary to pancreatitis.31,35 Hypoalbuminemia may also be seen. Hypocalcemia can be seen in severe cases and may be due to hypoalbuminemia or may also be due to the formation of calcium soaps with fatty acids in areas of fat necrosis.
Urinalysis often reveals an elevated urine specific gravity, secondary to dehydration. However, in severe cases, acute renal failure may ensue and the urine specific gravity may drop and casts may be seen in the sediment.
Diagnostic imaging
Abdominal radiographs may show a loss of detail in the cranial abdomen.31,35,37 In some cases, there may also be a suggestion of a mass in the cranial abdomen. Transposition of abdominal organs can also be seen in some cases and may include a transposition of the duodenum dorsally and laterally, the stomach to the left, and the transverse colon caudally.31,35,37 However, these findings are rather subjective and a conclusive diagnosis of pancreatitis is not possible on the basis of abdominal radiographs alone.
Thoracic radiographs in patients with pancreatitis are usually normal; however, pleural effusion maybe seen in a small number of severe cases.35
In contrast to abdominal radiography, abdominal ultrasonography is highly specific for pancreatitis if stringent criteria are applied (Figure 1.40).38 Over the last 20 years, abdominal ultrasonography has greatly advanced and is still advancing, leading to an improved resolution of diagnostic images. This progress has made repeated revisions of ultrasonographic diagnostic criteria necessary. When pancreatic ultrasonography in dogs was first introduced more than 20 years ago, the pancreas could not be routinely identified during abdominal ultrasonography and identification of the pancreas was seen as an
important indicator for the presence of pancreatitis. With better equipment and more expertise, the pancreas could soon be routinely identified in every dog and cat. However, an enlarged pancreas and/or fluid accumulation around the pancreas were considered highly suggestive of pancreatitis. Further advances led to the recognition that an enlarged pancreas and fluid accumulation around the pancreas alone are not sufficient to make a diagnosis of pancreatitis as pancreatic edema can also be observed with portal hypertension or hypoalbu- minemia.39 While not diagnostic for pancreatitis, various degrees of peripancreatic fluid accumulation are often seen in patients with pancreatitis.35,40 The pancreas may appear hypo- echoic when pancreatic necrosis is present.35,41 In acute cases, a hypoechoic pancreas is often surrounded by a hyperechoic area that is due to peripancreatic fat necrosis.35,40 Chronic pancreatitis may be associated with a hyperechoic pancreas indicating the presence of pancreatic fibrosis (Figure 8.8), but this finding is not commonly observed.42 However, it is important to note that with recent advances in image quality and resolution, echogenicity changes due to pancreatitis must be differentiated from echogenicity changes that are due to pancreatic hyperplastic nodules, which occur extremely frequently in both dogs and cats and is a change associated with age rather than pancreatitis.43,44 The need for stringent criteria for abdominal ultrasound has been underscored by a recent study, in which two of three cats that were suspected of having pancreatitis, but that did not have any evidence of pancreatitis during exploratory laparotomy or histopathological evaluation of a pancreatic biopsy, were falsely diagnosed with pancreatitis by abdominal ultrasonography.41 Other, less commonly reported findings in patients with pancreatitis are an enlarged pancreatic papilla and a dilated pancreatic duct. The sensitivity of abdominal ultrasound reported in 70 dogs with severe pancreatitis was 68%.35 This is higher than the sensitivity reported for cats with pancreatitis, which ranges between 11-35%.40,45,46 This difference is likely due to the larger size of the organ in the dog.
Contrast-enhanced abdominal CT is the diagnostic tool of choice for human patients suspected of having pancreatitis.47 This technology is not only highly sensitive for the diagnosis of human pancreatitis, but is also a sensitive tool for the detection of pancreatic necrosis and thus a useful prognostic tool. However, two recent studies showed that contrast-enhanced abdominal CT was inferior to abdominal ultrasonography in cats with suspected pancreatitis.41,46 A similar study in dogs also failed to show any diagnostic usefulness of this diagnostic tool in dogs suspected of having pancreatitis, though successful use of this technology has been reported in isolated cases.48,49
Pancreatitis markers (see also 1.4.4)
Serum amylase and lipase activities are of no clinical value for the diagnosis of pancreatitis in the cat and are of limited clini-
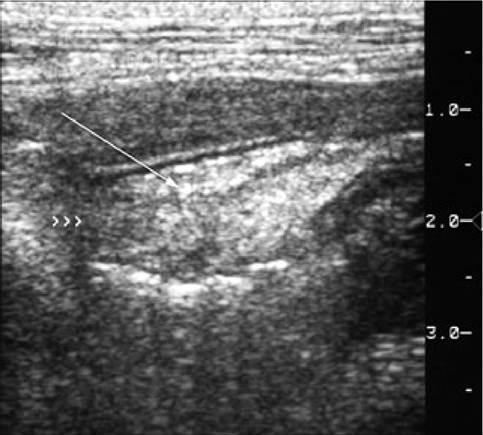
Figure 8.8:
Pancreatic fibrosis. This ultrasonographic image was taken in a cat. The pancreas is markedly hyperechoic (arrow) suggesting pancreatic fibrosis. However, pancreatic fibrosis often is not severe enough to be identified during ultrasound examination. (Image courtesy of Dr. Mark Saunders, Lynks Group, Shelburne, VT, USA.)
cal utility in the dog. The specificity of either of these parameters is only approximately 50%, even when stringent criteria are applied.50 Thus, serum amylase and lipase activities should only be used for the diagnosis of canine pancreatitis until more definitive diagnostic tests can be performed.
Trypsin-like immunoreactivity (TLI) is specific for exocrine pancreatic function. However, the sensitivity of serum TLI concentration for pancreatitis in dogs and cats is only approximately 30-60%, making it a suboptimal diagnostic test for pancreatitis in both species.41,45,46,51 However, serum TLI concentration remains the diagnostic test of choice for the diagnosis of EPI.
Recently, assays for the measurement of pancreatic lipase immunoreactivity in dogs and cats (cPLI and fPLI, respectively) have been developed and validated.52,53 Many different cell types in the body synthesize and secrete lipases. In contrast to catalytic assays for the measurement of lipase activity, the use of immunoassays does allow for the specific measurement of lipase originating from the exocrine pancreas.54
Serum PLI concentration is specific for exocrine pancreatic function. In one study, serum cPLI concentration was measured in a group of dogs with EPI and the median serum cPLI

Figure 8.9:
SNAP cPL. This figure illustrates the assay interpretation of the new SNAP cPL test. (a) A test spot that is lighter in color than the control spot indicates a serum Spec cPL concentration within the control range and suggests that pancreatitis is unlikely. (b) A test spot that is darker in color than the control spot suggests that serum Spec cPL is above the control range and pancreatitis may be present.
trol spot suggests that serum Spec cPL is above the control range and that pancreatitis may be present (Figure 8.9b). An abnormal result should always be followed up by the measurement of Spec cPL in the laboratory to confirm the diagnosis and to arrive at a base-line value that can be used to assess the progression of disease.
Pancreatic biopsy
Traditionally, a pancreatic biopsy has been viewed as the most definitive diagnostic tool for pancreatitis. Pancreatic biopsies can be collected during abdominal exploratory or by laparoscopy. The presence of pancreatitis is easily diagnosed by the gross appearance of the pancreas in many cases; however, the absence of pancreatitis can be difficult to prove. In a recent study, histopathological findings in dogs with pancreatitis were evaluated. The pancreata were sectioned every 2 cm.11 In half of all the dogs with pancreatitis and in two-thirds of dogs with chronic pancreatitis, evidence of pancreatic inflammation was found in less than 25% of all the sections.11 Thus, even if multiple biopsies are collected, pancreatic inflammation, especially in cases of chronic pancreatitis, may easily be missed. These findings also suggest that laparoscopy is inferior for the collection of a pancreatic biopsy as it is much more difficult to evaluate the entire organ during laparoscopy than during exploratory laparotomy. It should also be noted that while a pancreatic biopsy in itself is not associated with many complications, many patients with pancreatitis are poor anesthetic risks.
Therapy
Treatment of the cause
concentration was significantly decreased compared to healthy dogs and was not detectable in most of the dogs.55 Serum PLI concentration is also very sensitive for pancreatitis in both dogs and cats.10,41,51 The sensitivity ranges depending on the study population examined, but is higher than any other diagnostic test currently available. Serum PLI assays are speciesspecific and separate assays for dogs (Spec cPLtm) and cats (fPLI) are available. Currently, the fPLI assay is only available through the Gastrointestinal Laboratory at Texas A&M University (www.cvm.tamu.edu/gilab). In addition, an in-clinic test (SNAP cPL) for the measurement of PLI in dogs has recently been introduced. The assay is semi-quantitative and is evaluated by comparing the color of the test spot with the control spot. A test spot that is lighter in color than the control spot indicates a serum Spec cPL concentration within the control range and suggests that pancreatitis is very unlikely (Figure 8.9a). A test spot that is darker in color than the conAs with many other diseases, treatment of the underlying cause of pancreatitis should be the primary goal. However, many if not most cases of canine and feline pancreatitis remain idiopathic.16,31 In a few cases, the cause of the pancreatitis may be obvious (e.g., pancreatitis in a patient after removal of a pancreatic insulinoma). Nevertheless, when the cause of the pancreatitis is not obvious, the patient should be very carefully evaluated for any possible risk factors, such as hypertriglyceridemia, hypercalcemia, history of concurrent conditions, history of dietary indiscretion, anesthetic history, and drug his- tory.16 When a potential risk factor has been identified, it should be addressed appropriately. For example, if the patient has a history of being treated with potassium bromide and is considered to be in need of antiepileptic therapy, an alternative antiepileptic medication (e.g., Zonisamide or levetiracetam) should be chosen.
Identification and management of complications
As mentioned previously, pancreatitis can be associated with a variety of local and systemic complications. It is crucial to carefully monitor the patient for the development of any such local or systemic complications. While some complications, such as dehydration and electrolyte abnormalities may be easily corrected, others, when established, are extremely difficult, if not impossible, to counteract. In human patients, it has been suggested that the presence of organ failure of any major organ as a complication of pancreatitis for a period of more than 24 hours has a dramatic impact on the prognosis. While this may also be the case for veterinary patients, most likely the mere development of any such organ failure should be expected to have a severe negative impact on the overall prognosis. Therefore, patients should be carefully monitored and if any evidence of an impending development of organ failure is identified, aggressive measures should be taken to prevent such complications. For example, dehydration should be treated with aggressive fluid therapy to prevent acute renal failure.
Nutritional considerations
Until recently, it was common practice to hold dogs and cats with acute pancreatitis NPO (nothing per os), in order to “rest” the pancreas. However, there is little evidence that such resting of the pancreas has any beneficial effect and there is mounting evidence that nutritional support is crucial in pancreatitis patients. In human pancreatitis patients, early nutritional support has been shown to have a beneficial effect on outcome and enteral feeding is preferable over parenteral nu- trition.56-58 As a consequence, the author recommends feeding patients with pancreatitis orally if they do not vomit. If the patient does vomit, an antiemetic should be used and the patient should only be held NPO if vomiting cannot be controlled. If the patient has to be held NPO, alternative modes of alimentation, such as a jejunostomy tube, partial parenteral nutrition, or total parenteral nutrition must be considered.59 Feeding through a jejunostomy tube is preferable from a GI physiology point of view, but requires anesthesia for placement, which may have a negative impact on the overall outcome. Approximately 12 hours after the patient stops vomiting, the patient should be offered a small amount of fresh water. If this does not lead to vomiting, the patient should be offered a small amount of low-fat food, which should be repeated every few hours if the patient does not vomit.
If the patient does not vomit but refuses to eat, an esophagos- tomy or gastrostomy tube can be used for feeding. However, placement of both of these feeding devices requires general anesthesia and a nasogastric tube may be a better choice in these patients. In humans with acute pancreatitis, nasogastric tubes are commonly used with great success.
Regardless of the route of alimentation, a diet should be chosen that is low in fat. This is especially important in canine patients, where an ultra low-fat diet should be selected.
Analgesia
Abdominal pain or discomfort is one of the key clinical signs in human beings with pancreatitis and has been reported in more than 90% of all human pancreatitis patients.19 While the reported incidence of abdominal pain in dogs and cats is much lower than this (up to 58% in dogs and up to 25% in cats), the author believes that this difference is not due to an actual difference in the incidence of abdominal pain, but rather due to the inability to correctly identify abdominal discomfort in small animal patients.31,35 Therefore, the author suggests that every dog and cat with pancreatitis should be suspected of having abdominal pain and should be managed accordingly.60 Only if analgesic therapy does not appear to have any clinical impact should the analgesic therapy be discontinued.
There are a variety of analgesic options for dogs and cats. Patients that are being treated in a hospital can be treated with meperidine (5-10 mg/kg IM or SC as needed in dogs and 2-5 mg/kg IM or SC as needed in cats), butorphanol (0.20.4 mg/kg IV, IM, or SC q 2-4 h), fentanyl (initial dose 410 μg∕kg IV, then 4-10 μg∕kg∕h as a constant rate infusion), morphine (0.5-2.0 mg/kg IM or SC q 3-4 h in dogs; 0.050.2 mg/kg IM or SC q 3-6 h in cats), lidocaine (2 mg/kg diluted into 50 ml of warm 0.9% NaCl IP q 6-8 h), and a variety of other analgesic drugs.
The selection of analgesic drugs for outpatients is much more limited. Butorphanol (0.55 mg/kg PO in dogs and 0.4 mg/kg PO in cats q 6-12 h) or tramadol (1-4 mg/kg PO q 8-12 hr) can be used orally, while patients with more severe pain can be treated transdermally by use of a fentanyl patch (1/2 to a whole of a 2.5 mg patch [i.e., do not cut patch, but expose half of the membrane] for cats and small dogs [i.e., 30 kg BW); such patches are effective for 3-5 days.
Antiemetic therapy
Antiemetic therapy is very important in the treatment of pancreatitis for two reasons, the importance of providing nutritional support by the enteral route and because vomiting in itself is debilitating to the patient. A variety of antiemetic drugs are available. Dopamine inhibitors, such as metoclopramide, probably are the most commonly used antiemetic agents in small animal practice; however, these agents may not be a good choice in patients with pancreatitis as dopamine is crucial for
the regulation of splanchnic perfusion. While the effects of dopamine on pancreatic perfusion have not been evaluated, it seems prudent to use alternative antiemetic agents.
Another class of antiemetics are the HT3-antagonists, such as ondansetron (0.11-0.176 mg/kg IV q 12-24 h in dogs and 0.22 mg/kg IV q 12-24 h in cats) and dolasetron (0.3-0.6 mg/ kg IV, SC, or PO q 12-24 h in both dogs and cats). These agents are very effective, but can also be expensive. The advantage of dolasetron is that the intravenous formulation can be used orally, making it a lot more affordable than ondansetron tablets.
Recently, a new antiemetic, maropitant (1 mg/kg SC q 24 h or 2 mg/kg PO q 24 h in dogs; no known dosage for cats), has been licensed for dogs in Europe and the USA. This antiemetic is a NK1-antagonist and is highly effective in inhibiting vomition mediated by both peripheral and central pathways. In Europe, maropitant has been available for about a year and first experiences have shown that it has a high efficacy.61 Unfortunately, almost no data are available about the off-label use of maropitant in cats.
Protease inhibitors
Based on the pathophysiological evidence that shows that pancreatitis is ultimately caused by the premature activation of digestive pancreatic enzymes, there have been efforts to treat pancreatitis by inhibiting proteases. Aprotinin was one of the first drugs that was evaluated and in the early studies, the progression of experimental canine pancreatitis could be prevented when dogs were treated with aprotinin.62 In addition, an initial study with another protease inhibitor, gabexate mesylate, in dogs with experimental pancreatitis has shown some promising results.63 However, studies in human patients with spontaneous pancreatitis have not shown any beneficial effect of any of the protease inhibitors investigated.64,65 This may have been due to the fact that the dose used in the human patients was much lower than the one used in the dogs with experimental disease. However, it is more likely that the administration of a protease inhibitor in patients with established pancreatitis is simply too late in order to have any beneficial effect. It is possible, on the other hand, that the pretreatment of patients that are in danger of developing pancreatitis may be more useful and patients undergoing endoscopic retrograde cholangiopancreatography (ERCP) may benefit from being treated prior to the procedure.65 However, the routine use of protease inhibitors in veterinary patients is not indicated at this point in time.
Plasma
Plasma contains a variety of substances, including coagulation factors, proteinase inhibitors (i.e., α1-PI, α2-macroglubulin), and albumin, which may all have a beneficial effect in patients with pancreatitis.66 However, clinical studies in human pancreatitis patients failed to show any beneficial effect of using plasma.67,68 Despite these findings in human patients, most veterinary clinicians, including the author, believe that plasma has a beneficial effect in dogs with severe forms of pancreatitis. In cats, the benefit of plasma, which is largely unavailable, or any other blood product, is less clear. Also, the appropriate dose of plasma in dogs with severe pancreatitis is unknown. Factors, such as overall severity, systemic complications, and especially serum albumin and antithrombin-III (AT-III) concentrations in the patient should be taken into consideration. However, the goal of plasma therapy in pancreatitis patients is not to normalize the serum albumin or AT-III concentrations.
Antibiotics
Many veterinarians routinely treat dogs and cats with acute or chronic pancreatitis with antibiotics; however, there is little scientific evidence for such practice. For example, the use of antibiotics in humans with acute pancreatitis is still questionable, even though approximately a third of all human pancreatitis patients that die of their disease process die of infectious complications.69 Although early studies in the 1970s showed no benefit of routine antibiotic use in human pancreatitis patients, studies in the 1990s did show a beneficial effect.70-72 Several meta-analysis studies have recently been presented on this topic, but their results are contradictory.73-75 In addition, two recent consensus reports concerning the treatment of severe acute pancreatitis in humans did not recommend the routine use of antibiotics.56,76 To complicate matters further, dogs and cats with severe pancreatitis are believed to only rarely have infectious complications. In fact, to date, only four dogs and one cat have been reported that had such infectious com- plications.22-24 All five of these patients were diagnosed with an infected abscess.22-24
In conclusion, the author currently believes that routine therapy of canine and feline pancreatitis patients with antibiotics should be avoided. Instead, antibiotics should only be given if an infectious complication is identified or highly suspected as in patients with a urinary tract infection or aspiration pneumonia.
Anti-inflammatory agents
Non-steroidal anti-inflammatory drugs (NSAIDs) should not be administered to patients with pancreatitis as many of them have been shown to potentially cause pancreatitis. They are all known to cause GI side effects, and they do not appear to have any beneficial effect on pancreatic inflammation.28
Glucocorticoids were once believed to cause pancreatitis in both humans and veterinary species.16,77 However, the scientific basis for this hypothesis is weak and in fact, in humans, glucocorticoids are generally no longer believed to be a risk factor for pancreatitis.28 It must be borne in mind, however, that patients who receive glucocorticoids generally have diseases that in themselves are considered risk factors for pan- creatitis.28
About 20 years ago, a new disease entity was described in humans: autoimmune pancreatitis.78 Since the initial description of the disease, its characterization has been changed and autoimmune pancreatitis is now believed to be an important cause of chronic pancreatitis in humans.78,79 Autoimmune pancreatitis is characterized by a lymphoplasmacytic infiltration and fibrosis of the pancreas that appears to be mostly distributed in the area around the pancreatic duct system.78,79 It is interesting to note that most dogs and cats with chronic pancreatitis also have a lymphoplasmacytic inflammation of the pancreas. In addition, many dogs and especially cats with chronic pancreatitis have concurrent inflammatory conditions of other abdominal organs, such as IBD and/or hepatitis/ cholangiohepatitis.80 While not all canine and feline patients with pancreatitis may benefit from glucocorticoid therapy, anecdotal reports have shown that some patients do respond quite favorably. Also, a recent case report has documented the favorable response of a cat with lymphoplasmacytic pancreatitis to prednisolone therapy.81
The author recommends evaluating patients with chronic pancreatitis for any potential risk factor or concurrent disease and only treating those patients with glucocorticoids that do not have any identifiable risk factors and /or concurrent conditions that pose a contraindication to the use of corticosteroids (e.g., suppurative cholangiohepatitis). The author measures the PLI concentration (Spec cPL in dogs and fPLI in cats) before treatment is started and rechecks the PLI concentration after 10-14 days of therapy. Treatment should only be continued if the patient has either clinically improved, the serum PLI concentration has decreased, or both.
Dopamine
Dopamine is crucial for splanchnic and pancreatic perfusion and hypotension and pancreatic hypoperfusion can lead to pancreatitis. One study in cats with experimental pancreatitis has shown that the progression of pancreatitis can be halted if patients are treated with dopamine within 12 hours after the induction of pancreatitis.82 This is obviously not feasible in spontaneous pancreatitis patients. However, treatment of patients at risk for pancreatic hypoperfusion (i.e., patients with pancreatitis that have to undergo general anesthesia) may benefit from dopamine therapy. A low dose (i.e., 2-5 μg∕kg∕min as a constant rate infusion) should be given, as this dose does not cause peripheral vasoconstriction and so does not negatively affect splanchnic perfusion.
Antioxidants
There is some evidence suggesting that reactive oxygen species (ROS) play a role in the pathogenesis of pancreatitis.83 Such ROS can lead to tissue damage and also stimulate an inflammatory response. Thus, it has been hypothesized that antioxidants should have a beneficial effect in patients with pancreatitis. Several studies in humans with acute pancreatitis have suggested a beneficial effect.84-86 However, other, controlled, studies were not able to confirm these effects.87 A single study in dogs with acute pancreatitis suggested that selenious acid decreased the mortality rate of dogs with acute pancreatitis by 50%.84 However, the findings of this study are suspect as only historical controls were used, with the control dogs being enrolled in a time period before the period in which the treated dogs were enrolled.84 In addition, the enrollment occurred over several years and it is, therefore, likely that the dogs enrolled later in the study (i.e., the dogs in the treatment group) would have had less severe disease as the diagnostic modalities for pancreatitis had improved during this period.84 In conclusion, at this point in time, there is little evidence to suggest that the use of antioxidants in canine and /or feline patients with acute severe pancreatitis would be of benefit.
Recently, it has been speculated that antioxidants may be more efficacious in patients with mild chronic pancreatitis.88 In a pilot study of five dogs with subclinical pancreatitis, antioxidant administration led to a decrease in median serum cPLI, cTLI, and CRP concentrations, suggesting that further studies would be warranted (Steiner JM, unpublished data, 2007).
Modulation of inflammatory mediators
Over the last decade it has become clear that pancreatitis is a two-stage disease process with the first stage being caused by premature activation of pancreatic digestive enzymes and the second stage being due to an inflammatory response by the body. In fact, it has been suggested that most systemic complications of pancreatitis are due to the inflammatory response rather than the prematurely activated enzymes. Once the inflammatory reaction has been initiated, proteinase inhibition appears to have little effect on the disease.64 Therefore, modulation of inflammatory mediators may be a promising method of treatment.
One group of modulators of inflammatory mediators investigated initially were the platelet-activating factor antagonists (PAFANTs) and one of the first compounds in this group investigated was lexipafant. Lexipafant was used in several studies on experimental pancreatitis and also in some small clinical trials in humans with pancreatitis, and all showed a beneficial effect.89,90 In comparison, a large international multi-center trial with more than 1000 humans with acute pancreatitis failed to show a beneficial effect.91 However, the results of this study have not yet been published, probably because of commercial constraints and the very disappointing results of the study. Other modulators of inflammatory cytokines are currently being evaluated.
Surgical intervention
A variety of surgical procedures have been suggested for patients with acute and /or chronic pancreatitis, including peritoneal lavage, partial pancreatectomy, and necrosectomy for acute pancreatitis, and partial pancreatectomy and cyst or abscess removal for chronic pancreatitis. There are no studies that have systematically evaluated the effectiveness of pancreatic surgery for either acute or chronic pancreatitis in dogs or cats. The results of such procedures in humans have been rather disappointing and current recommendations for surgical intervention for human pancreatitis patients are rather conser- vative.76,92,93 Currently, the only indications for surgery are an infected necrosis, a pancreatic abscess, or a pancreatic pseudocyst that does not regress.93 There have been isolated reports about surgical intervention in single cases in veterinary patients, but the results are again rather discouraging and it seems prudent to also be conservative when treating dogs and cats with pancreatitis.22,23
Prognosis
The prognosis for dogs and cats with pancreatitis is largely dependant on the presence of local and systemic complications. Patients without pancreatic necrosis and no systemic complications have a good prognosis, while patients with extensive pancreatic necrosis and multi-organ failure have a poor prognosis.94 In dogs and cats, even single organ failure, such as acute renal failure or acute lung failure may not be reversible. In humans with pancreatitis, organ failure in and of itself does not appear to have a major negative effect on outcome, but the presence of any organ failure for more than 24 hours dramatically worsens the prognosis. In comparison, in dogs and cats, the reversal of even single organ failure is not very successful.
In humans, several severity scoring systems (e.g., Ranson’s early prognostic signs, the acute physiology and chronic health evaluation II [APACHE II] score, or the sequential organ failure assessment [SOFA] score) are used to evaluate patients on admission.95,96 This is important because patients may not appear at first to be severely ill clinically, but may develop complications and organ failure shortly after admission. Patients that have a high score on admission must be treated more aggressively to prevent organ failure.97 Several scoring systems and isolated prognostic factors used in humans have been modified for use in the dog or cat, but none have proven reliable in clinical patients thus far.94,98
8.2.1