parenteral NUTRITIONAL SUPPORT
Nutrition can be provided intravenously to meet part or all of a patient’s nutritional needs (Figure 12-37, A and B).Either all of the nutritional needs may be met (so-called total parenteral nutrition [TPN]), or some of the nutritional needs may be met (so-called partial parenteral nutrition [PPN]).
Actually, even with TPN, nutritional requirements are not completely met; however, most of the major nutrient requirements may be met. Components used in formulating parenteral nutrition include a protein source in the form of amino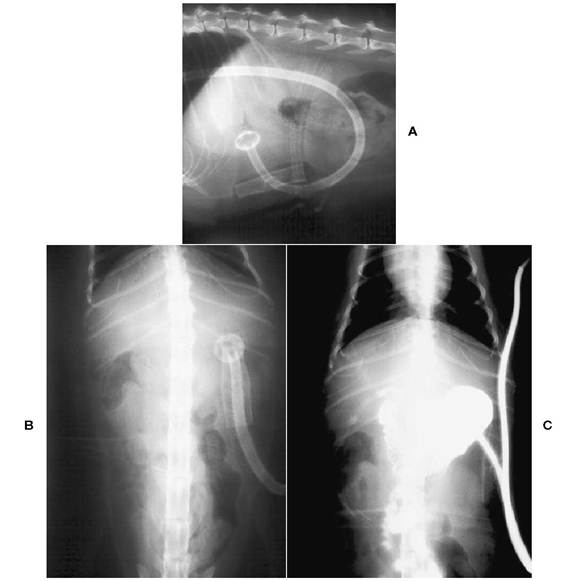
Figure 12-36 A, Survey lateral abdominal radiograph of an adult cat with a mushroom-tipped percutaneous endoscopic gastrostomy feeding tube. B, Survey ventrodorsal abdominal radiograph of the adult cat in A. C, Ventrodorsal abdominal radiograph of an adult cat with a mushroom-tipped percutaneous endoscopic gastrostomy feeding tube. Diluted iodinated contrast medium has been injected into the tube, which is positioned on the left abdominal wall. Contrast fills the stomach and has entered the small intestine.
acids, a carbohydrate source in the form of dextrose, a lipid source in the form of long-chain fatty acids, electrolytes, minerals, trace elements, and vitamins (Figure 12-38). Amino acids are commonly supplied as an 8.5% solution with or without electrolytes (4.25% to 10% solutions are available), dextrose is commonly supplied as a 50% solution, and lipids are commonly supplied as a 20% emulsion (10% solutions are also available). If electrolytes are not contained in the amino acid solution, an electrolyte solution designed for use with parenteral nutrition can be used (TPN electrolytes providing 16.1 mg sodium chloride per milliliter, 16.5 mg calcium chloride per milliliter, 74.6 mg potassium chloride per milliliter, 25.4 mg magnesium chloride hexahydrate per milliliter, and 121 mg sodium acetate per milliliter) and potassium phosphate (224 mg of monobasic potassium phosphate per milliliter and 236 mg dibasic potassium phosphate per milliliter) may be added as a source of phosphate.
Vitamins and trace elements are also available for use. We routinely use a B-vitamin complex in the parenteral solution (1 ml/L of TPN). Vitamin K cannot be given intravenously and is administered subcutaneously at 0.25 mg/lb once a week.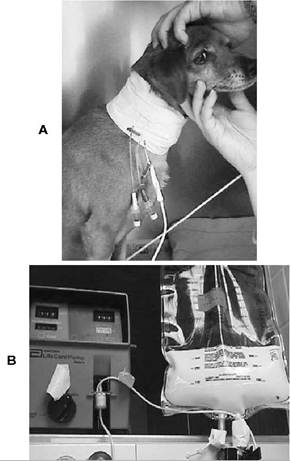
Figure 12-37 A, Total parenteral nutrition (TPN) being administered to an adult male Dachshund with an insulinoma.A triple lumen jugular catheter has been inserted, and the TPN is the white solution flowing through the bottom infusion line. B, TPN admixture bag for the dog described in A. TPN is administered using an infusion pump.
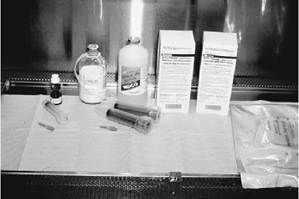
Figure 12-38 TPN components (clockwise from left):TPN multivitamin (brown bottle),lipid (white solution in glass bottle), 50% dextrose (plastic bottle), amino acids (two boxes), all-in-one admixture bag, and syringes and needles.
Total Parenteral Nutrition
Nutritional requirements are calculated in the same way as described for enteral nutrition. We calculate energy requirements, protein requirements, and then water requirements.The lipid and dextrose (nonprotein calories) provide energy. Usually the lipid component provides 40% to 60% of the nonprotein calories, and the dextrose component provides the remainder of the calculated caloric requirements. A 20% lipid emulsion provides 2 kcal/ml, and a 50% dextrose solution provides 1.7 kcal/ml. Protein requirements are then calculated as described previously. For maintenance, 4 g/100 kcal of energy intake for dogs and 6 g/100 kcal of energy intake for cats is required; more or less can be provided depending on protein status and disease state.An 8.5% amino acid solution provides 0.085 g of protein per milli- liter.We add 20 ml of TPN electrolyte solution per liter of TPN solution and 5 ml of potassium phosphate per liter of TPN solution. The amino acid solution is also available as a balanced electrolyte solution; however, it is more expensive than amino acid solutions without added electrolytes.
B vitamins may be added at 1 ml per liter of solution. If additional electrolytes are required, for example, KCl, they may be added. If additional fluids are required, for example, lactated Ringer’s solution (LRS), they may either be added to the TPN solution or they may be administered through a separate intravenous catheter. Magnesium may be added to parenteral solutions; however, magnesium chloride is the salt of choice to add and not magnesium sulfate because the sulfate form is not compatible with parenteral solutions.The resultant osmolality of TPN is usually 800 to 1200 mOsm/kg; therefore TPN solution must be administered through a centrally placed catheter to avoid thrombophlebitis. The 8.5% amino acid solution is approximately 800 mOsm/kg; therefore 4.25% amino acid solution is close to isotonicity. The 50% dextrose solution is approximately 2000 mOsm/kg (Table 12-5); therefore 5% dextrose is approximately isotonic. The lipid emulsion does not exert tonicity; therefore it is not included in the calculation of osmolality.
Partial Parenteral Nutrition
With partial parenteral nutrition, all of the calculated nutritional requirements are not met. This may occur if less than the calculated amount of formula is administered, if components of the
parenteral nutrition are not administered, or if components are diluted to allow administration through a peripheral vein. If the clinician is administering parenteral nutrition through a peripheral vein (such as a cephalic or saphenous vein), the solution must be isotonic. It is difficult to meet protein needs with 4.25% amino acid solution, and difficult to meet caloric needs using 5% or 10% dextrose. Often PPN is administered to dogs infected with parvovirus to provide some calories or protein. In most instances we use TPN.
| TABLE 12-5 | Parenteral Glucose Solutions | |
| Glucose Concentration (%) | Caloric Content (kcal/L) | Osmolarity (mOsm/L) |
| 5 | 170 | 253 |
| 7.7 | 262 | 388 |
| 10 | 340 | 505 |
| 20 | 680 | 1010 |
| 30 | 1020 | 1515 |
| 40 | 1360 | 2020 |
| 50 | 1700 | 2525 |
| 60 | 2040 | 3030 |
| 70 | 2380 | 3535 |
| 100 | 3400 | 5050 |
Formulation and Administration When compounding parenteral nutrition solution, it is critical that aseptic technique be adhered to (Box 12-5).
The dextrose and lipid are excellent media for bacteria, and there are no bacteriostatic or bactericidal properties to parenteral solutions. If pharmacists prepare parenteral nutrition solutions, they will use a laminar flow hood to minimize the risk of bacterial contamination. We compound parenteral nutrition solutions in an operating room suite after gowning and gloving in (Figure 12-39). Tops to bottles are prepared aseptically as if it were a surgical site. Although infrequent, sepsis and bacteremia can occur with TPN administration (in humans on long-term TPN administration, the incidence is 3% to 5%).We place single-, double-, or triple-lumen catheters in the jugular vein for administration of TPN. If a single-lumen catheter is inserted, it should only be used for TPN administration. If a double- or triple-lumen catheter is used, one port is dedicated for TPN solution administration and the other port(s) may be used for administering other fluids, administering medication, or collecting blood samples. The jugular catheter must be placed as aseptically as possible. It is possible to administer TPN through a single-lumen jugular catheter that is inserted into a cephalic vein, which terminates in the subclavian vein or cranial vena
BOX 12-5
Prevention, Diagnosis, and Therapy Protocols for Sepsis Associated With Parenteral Nutrition
Prevention Protocol
Prepare and handle parenteral solutions aseptically.
Use aseptic technique to place intravenous catheters.
Ensure strict aseptic management of dressing and infusion apparatus.
Change bandage covering intravenous catheter at least every other day.
Maintain a closed system.
Do not inject medications or blood products, measure central venous pressure, or draw blood through the catheter.
Use a specialized team or individual to manage therapy.
Appropriately treat concurrent infections.
Diagnosis and Treatment Protocols
Suspect sepsis if the patient develops a fever.
Monitor closely for any indication of source and/or progression toward septic shock/endotoxemia.
Monitor blood parameters for predictive changes of sepsis.
If no source of fever can be found within 24 hours after detection, culture the blood, parenteral nutrition solution, and catheter. Pending culture results, use Gram stain to examine the solution and catheter, if it is removed.
Catheter may be removed and replaced over a guide wire pending culture results if continued feeding or vascular access is desired.
If the bacteriologic culture of the catheter is positive, remove the replacement catheter.
Begin empiric antibiotic therapy until culture results return.
Allow 24 to 48 hours for bacteremia to resolve before a new catheter is placed.
Specific antibiotic therapy is initiated according to culture and sensitivity results.
Continue specific, symptomatic, and supportive treatment appropriate for the patient’s clinical status.

FIGURE 1 2-39 Veterinary nurses aseptically preparing TPN solution.
cava, or a catheter inserted into the femoral vein, which terminates in the caudal vena cava. Aseptic catheter management is imperative.As few people should handle the catheter or the TPN solution as possible. Tubing connections should be scrubbed before connecting, and the connections should be taped together to prevent them from accidentally separating. If the lines become disconnected, then all tubing should be discarded. Some recommend discarding the TPN solution as well in this instance.
Once the TPN is formulated and compounded, the daily amount is calculated and is administered as a constant-rate infusion. The volume of TPN solution that must be administered over the 24-hour period determines the rate. Usually the administered volume meets or slightly exceeds the daily fluid requirement; therefore additional fluids are not needed. However, if a patient is losing more fluid than maintenance (e.g., ascites, polyuric diseases, or peritonitis), then additional fluids must be administered.
To begin TPN, one half of the calculated rate (milliliters per hour) is administered for the first 8 to 12 hours; supplemental fluids will need to be administered to meet daily fluid requirements. At the end of this period the clinician should measure levels of blood glucose, blood urea nitrogen (BUN), packed cell volume (PCV), and total solids and examine the plasma or serum for lipemia or hemolysis. If the findings are normal, the rate of TPN is increased to full and the supplemental fluids are decreased or discontinued. After an additional 8 to 12 hours (which is usually in the morning), a complete blood count, serum biochemical analysis, and urinalysis should be performed (Box 12-6).The TPN solution can be adjusted as needed based on these results. Laboratory evaluation should be performed as needed depending on the underlying disease; however, renal function, electrolyte concentrations, and acid-base status should be evaluated every 3 to 4 days.Blood work should be repeated anytime an unexpected turn for the worse occurs. A bottle of TPN solution may be used for 3 days and occasionally 4 days. If used for more than 3 or 4 days, the risk of bacterial contamination increases and the lipid emulsion begins to break down. Breaking down of the emulsion results in a “brown scum” that adheres to the glass bottle; this process is called caramelization.Once the patient begins eating or is well enough to begin eating, TPN may be discontinued. This is accomplished by decreasing the rate to one half of the calculated maintenance rate for 8 to 12 hours. TPN can be discontinued after this point is reached. If TPN is discontinued too quickly, hypoglycemia may occur.
Complications of Parenteral Nutrition
Complications associated with parenteral nutrition may be classified as mechanical or metabolic (Table 12-6). Mechanical complications include accidental removal of the venous catheter, accidental disconnection of lines, kinking of the
BOX 12-6
Protocol for Monitoring Patients Receiving Parenteral Nutrition
1. Vital signs, including temperature, pulse, and respiration (TPR), mucous membrane color, and capillary refill time every 6 to 12 hours
2. Body weight every 24 hours
3. Blood glucose level every 6 to 12 hours initially, then at least every 24 to 72 hours
4. Serum electrolyte concentrations every 24 hours for the first 2 to 3 days, then at least one to two times a week
5. Serum urea nitrogen concentration 12 hours after beginning parenteral nutrition, then at least one to two times a week
6. Packed cell volume, total solids, platelet count, and plasma color and turbidity every 24 hours for 2 to 3 days, then at least once a week
7. Complete blood cell count and serum biochemical profile at least one to two times a week, more often if indicated catheter or lines, occlusion of the lines or catheter, or using a bottle of parenteral solution for too long. There are several metabolic complications that can occur and have been described; however, the most common ones are hypoglycemia, hyperglycemia, hyperlipidemia, metabolic acidosis, and potassium imbalances. Fortunately, these are not usually severe. As mentioned before, trace element and/or mineral deficiency may occur. In one study of dogs and cats receiving TPN for 1 to 14 days, clinical signs of mineral or trace element deficiencies were not apparent. In that study 46% of cases experienced mechanical problems (e.g., break in infusion line or catheter dysfunction), 16% developed clinical sepsis, and metabolic complications (e.g., glucose, lipid, protein, electrolyte, or acidbase imbalances) occurred in approximately 50% of the cases but did not result in clinical problems. Mechanical and septic complications can be minimized by practicing aseptic technique when
| TABLE 12-6 | Complications, Predisposing Factors, Prevention, and Therapy Related to Parenteral Nutrition | |||
| Complication | Predisposing Factors | Prevention | Therapy | |
| Hyperglycemia | Diabetes mellitus, stress, glucocorticoids, rapid glucose infusion | Consider enteral nutrition, insulin therapy with diabetes mellitus; monitor blood and urine glucose | Decrease infusion rate; change to a lower dextrose/higher lipid infusion, insulin | |
| Hypoglycemia | Abruptly stopping dextrose solution | Taper feedings; monitor blood glucose levels | Intravenous or oral carbohydrate | |
| Hypokalemia | Insulin therapy, diuretic therapy, vomiting, diarrhea, rapid dextrose infusion, chronic renal disease in cats, metabolic alkalosis | Monitor serum K+ | Supplement K+; correct or control underlying cause | |
| Hyperkalemia | Metabolic acidosis, renal failure | Monitor serum K+ | Sodium bicarbonate if acidotic; decrease K+ content of solution; increase dextrose infusion; glucose and insulin administration; administer diuretics that promote K+ excretion | |
| Hypophosphatemia Diabetes mellitus, insulin therapy | Monitor serum phosphorus | Supplemental phosphorus; stop insulin if possible; stop feedings | ||
| Hypomagnesemia Diuretic therapy, malabsorption | Monitor serum Mg2+ | Supplemental Mg2+ | ||
| Hypocalcemia | Hypoalbuminemia, hypomagnesemia, hyperphosphatemia | Monitor serum Ca2+ | Supplemental Mg2+ if low; monitor ionized Ca2+; supplemental Ca2+; increase serum protein | |
| Low Na+/low carbohydrate diet, cardiac disease, hypoalbuminemia | Avoid high carbohydrate/ high Na+ diets | Correct Na+ intake; increase serum protein; treat underlying cardiac disease | ||
| Abnormal liver function test results | Stress, infection, excessive intake of carbohydrate, anorexia (cats) | Monitor liver enzymes | Decrease intake of dextrose/increase lipid; decrease feedings | |
| Metabolic acidosis Diarrhea, renal failure, excessive amino acid intake | Monitor serum total CO2 or blood gas values; avoid excessive amino acid infusion | Increase acetate and decrease Cl- in solution; decrease amino acid intake; sodium bicarbonate therapy | ||
| TABLE 12-6 | Complications, Predisposing Factors, Prevention, and Therapy Related to Parenteral Nutrition—cont’d | |||
| Complication | Predisposing Factors | Prevention | Therapy | |
| Metabolic alkalosis Vomiting | Monitor CO2 or blood gas values; control vomiting | Increase Cl- and decrease acetate in solution | ||
| Hypovolemia | Gastrointestinal or renal losses, fluid loss in body cavities | Monitor hydration status; quantitate fluid loss | Increase intake of fluid | |
| Hyponatremia | Gastrointestinal loss, fluid overload, diuretics | Monitor serum Na+; discontinue diuretics; monitor hydration | Supplemental Na+ | |
| Hyperlipidemia | Diabetes mellitus, glucocorticoids, rapid or excessive lipid infusion | Monitor plasma turbidity | Decrease rate or amount of lipid infused, treat underlying metabolic cause(s) of lipid intolerance | |
placing the intravenous access line and by careful handling of the infusion system. Monitoring serum biochemical parameters and adjusting the TPN rate or formulation as needed may minimize metabolic complications.
References
Abood SK, Buffington CA: Improved nasogastric intubation technique for nutritional support in dogs, J Am Vet Med Assoc 199:577,1991.
Abood SK, Buffington CA: Use of nasogastric tubes: indications, technique, and complications. In Kirk RW, Bonagura JD, eds: Current veterinary therapy XI, Philadelphia, 1992,WB Saunders.
Abood SK et al.: Nutritional support of hospitalized patients. In Slatter D, ed: Textbook of small animal surgery, ed 2, Philadelphia, 1993,WB Saunders.
Armstrong PJ: Enteral feeding of critically ill pets: the choices and techniques, Vet Med 87:900,1992.
Armstrong PJ, Lippert AC: Selected aspects of enteral and parenteral nutritional support, Semin Vet Med Surg (Small Anim) 3:216,1988.
Bartges JW: Nutritional support. In Lipowitz AJ et al., eds: Complications in small animal surgery, Baltimore, 1996,Williams & Wilkins.
Brady LJ et al.: Influence of prolonged fasting in the dog on glucose turnover and blood metabolites, J Nutr 107:1053, 1977.
Bright RM: Percutaneous tube gastrostomy with and without endoscopy. Proceedings of the fourth annual forum of the American College of Veterinary Internal Medicine, 1986.
Bright RM, Burrows CF: Percutaneous endoscopic tube gastrostomy in dogs, Am J Vet Res 49:629,1988. Carnevale JM et al.: Nutritional assessment: guidelines to selecting patients for nutritional support, Comp Cont Educ Pract Vet 13:255, 1991.
Cerra FB: How nutrition intervention changes what getting sick means, J Parenter Enteral Nutr 14:164S, 1990.
Crowe DT: Nutritional support for the seriously ill or injured patient: an overview, J Vet Emerg Crit Care 1:1, 1985.
Crowe DT: Clinical use of an indwelling nasogastric tube for enteral nutrition and fluid therapy in the dog and cat, J Am Anim Hosp Assoc 22:675, 1986.
Crowe DT, Downs MO: Pharyngostomy complications in dogs and cats and recommended technical modifications: experimental and clinical investigations, J Am Anim Hosp Assoc 22:493, 1986.
Fulton RBJ, Dennis JS: Blind percutaneous placement of a gastrostomy tube for nutritional support in dogs and cats, J Am Vet Med Assoc 201:697, 1992.
Haskins SC: A simple fluid therapy planning guide, Semin Vet Med Surg (Small Anim) 3:227,1988.
Howe PE et al.: Fasting studies.VI. Distribution of nitrogen during a fast of 117 days, J Biol Chem 11:103, 1912.
Lippert AC: Parenteral nutrition. In: DiBartola SP, ed: Fluid therapy in small animal practice, Philadelphia, 1992, WB Saunders.
Lippert AC, Fulton RBJ, Parr AM: A retrospective study of the use of total parenteral nutrition in dogs and cats, J Vet Intern Med 7:52, 1993.
Lippert AC et al.: Total parenteral nutrition in clinically normal cats, J Am Vet Med Assoc 194:669, 1989.
McCrackin MA et al.: Endoscopic placement of a percutaneous gastroduodenostomy feeding tube in dogs, JAm Vet Med Assoc 203:792, 1993.
Rawlings CA: Percutaneous placement of a midcervical esophagostomy tube: new technique and representative cases, J Am Anim Hosp Assoc 29:526, 1993. Remillard RL, Martin RA: Nutritional support in the surgical patient, Semin Vet Med Surg (Small Anim) 5:197,1990.
Remillard RL,Thatcher CD: Parenteral nutritional support in the small animal patient, Vet Clinic North Am SmallAnim Pract 19:1287,1989.
Sanderson SS, Bartges JW Osborne CA: Management of anorexia. In Kirk RW Bonagura JD, eds: Current veterinary therapy XffLPhiladelphia, 1999,WB Saunders. Tennant B,Willoughby K:The use of enteral nutrition in small animal medicine, Comp Cont Educ Pract Vet 15:1054,1993.
Thatcher CD, Hand MS, Remillard RL: Small animal clinical nutrition: an iterative process. In Hand MS et al., eds: Small animal clinical nutrition, ed 4,Topeka, Kan, 2000, Mark Morris Institute.