Pulmonary Edema
Pamela A. Wilkins
Pulmonary edema rarely occurs as a primary event in the horse and, when present, is usually secondary to some other pathologic process. Extravascular fluid accumulates within the lung after events that alter hydrostatic and colloid osmotic interstitial and vascular forces change the surface area and pore size of the blood-gas barrier or diminish lymphatic drainage.1 Pulmonary edema can be classified as cardiogenic or noncardio- genic.
Pulmonary capillary pressure can be increased by any increase in left atrial or pulmonary artery pressure. In horses, this can occur secondary to acute renal failure, left heart failure, or very high cardiac output conditions, such as extreme exercise. Increases in microvascular permeability may occur with sepsis, disseminated intravascular coagulation, hypoxic acidosis, allergic responses such as transfusion reactions, or primary pulmonary pathology, resulting in the release of mediators of inflammation that increase vascular endothelial or alveolar epithelial permeability. Pulmonary edema associated with airway obstruction has been termed negative pressure pulmonary edema (NPPE) and has been reported in horses.2-7 NPPE occurs secondary to inspiratory efforts against a closed glottis that result in a precipitous fall in intrathoracic pressure. The large decrease in intrathoracic pressure increases the transmural pressure gradient for all intrathoracic vascular structures, favoring movement of water into the extravascular space. Transient pulmonary obstruction may be a root cause of fatal exercise- induced pulmonary hemorrhage (EIPH) in racehorses and other horses performing at maximal exercise; these horses are predisposed because of already large transmural pulmonary vascular pressures and large intrathoracic pressure swings associated with breathing (Wilkins and Del Piero, unpublished data) (Fig. 31.35).Diagnosis is based on clinical examination, history of predisposing causes, and radiographs. Horses have a shallow rapid respiratory pattern and may be dyspneic. Arterial blood gas analysis may reveal hypoxemia and hypercapnia. Fine crackles or wheezes may be audible on auscultation. Patients with volume overload (associated with renal failure or, rarely, too-rapid fluid administration) or primary cardiac problems may have an increased central venous pressure with pronounced venous distention. Fluid (clear or slightly yellow or pink-tinged) may drip from the nostrils and can increase in volume without necessarily becoming frothy. Continuous coughing and production of frothy blood-tinged or bloody fluid production warrants a very grave prognosis. Radiographic findings are nonspecific but include peribronchial and perivascular cuffing, increased prominence of vessels, and a hazy reticular interstitial pattern (Fig. 31.36). Underlying pulmonary disease may obscure signs of edema, and radiographs of sufficiently high quality to show relatively subtle changes may not be obtainable in mature horses. Numerous diffuse comet-tail artifacts are seen with thoracic ultrasound examination (Fig. 31.37). Noncardiogenic pulmonary edema (capillary leak) is a component of the definition for VetALI and VetARDS (see the Acute Respiratory Distress Syndrome and Acute Lung Injury [Acute Bronchointerstitial Pneumonia] section earlier).
■ Treatment Treatment consists of correcting the cause, reversing hypoxemia, decreasing plasma volume and left atrial pressure, and increasing plasma colloid osmotic pressure. Intranasal oxygen and even positive ventilation may be needed in severe cases. Improvement in oxygenation can be monitored by sequential arterial blood gas analysis or by using transcutaneous
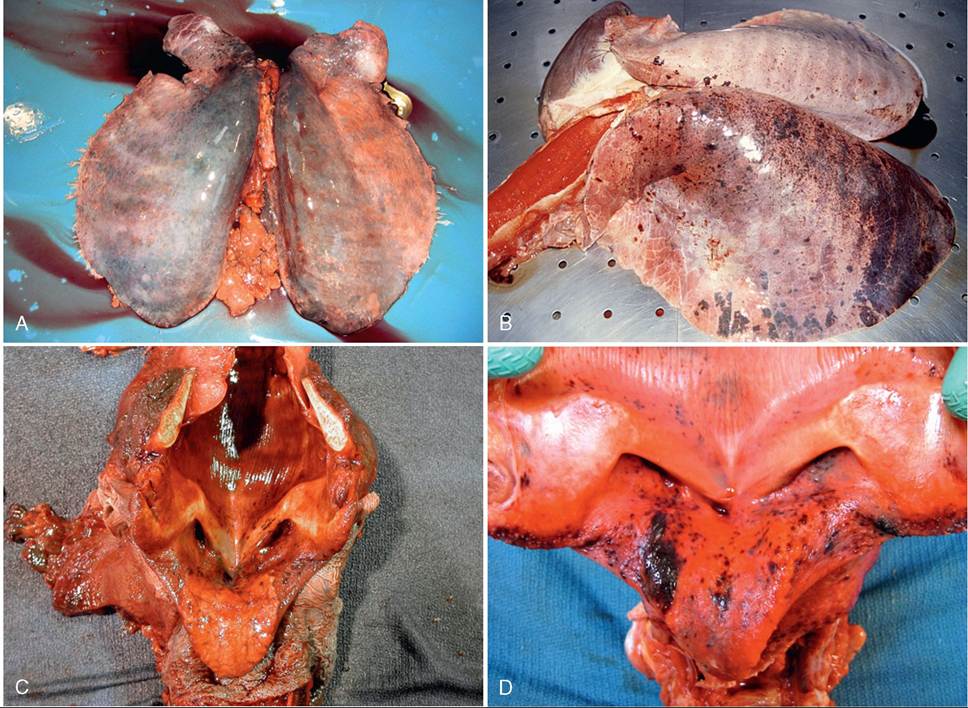
FIG. 31.35 A, Lung from a horse that suffered sudden death on the racetrack caused by fatal exercise-induced pulmonary hemorrhage (EIPH).
Note the dorsal acute hemorrhage, diffuse edema, and rib impressions present on the dorsal surface of the lung. B, Lung from a horse that suffered documented upper airway obstruction at maximal exertion on a treadmill. This horse experienced fatal EIPH. Note the severe pulmonary edema with hemorrhage, bloody froth in trachea, and ecchymotic hemorrhages in trachea. C, Larynx of a horse that suffered from fatal EIPH. Note the widespread diffuse subepithelial hemorrhage, ecchymoses, and petechia, supporting negative airway pressure as the cause. Upper airway occlusion due to left laryngeal hemiplegia is supported by the significantly decreased muscle mass of the left cricoarytenoideus dorsalis muscle bodies. D, Larynx from a horse found dead in stall with evidence of hemorrhagic pulmonary edema. Negative pressure pulmonary edema secondary to airway occlusion is supported as the cause of death because of its presence throughout the larynx and upper airway. (Courtesy Dr Fabio Del Piero, Louisiana State University, Baton Rouge, La.)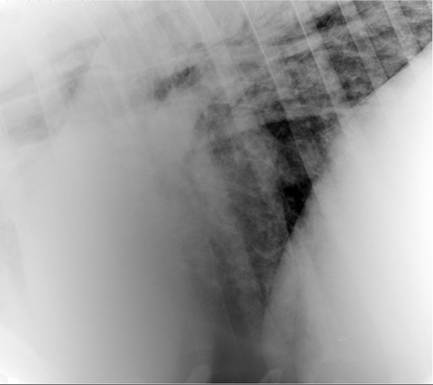
FIG. 31.36 Radiograph of caudal ventral lung of a horse with pulmonary edema. Note the mixed hazy reticular interstitial pattern. Bronchiolar cuffing is also evident. (Courtesy Dr Midge Leitch, University of Pennsylvania, New Bolton Center, Kennett Square, Penn.)

FIG. 31.37 Ultrasound image of lung of a horse with pulmonary edema. Note the multiple diffuse comet-tail artifacts. (Courtesy Dr. Kim Sprayberry, California Polytechnic State University, San Luis Obispo, Calif.)
■ TABLE 31.11
Pharmacologic Treatments for Pulmonary Edema in Horses
| Treatment | Reason | Route | Dose/Rate | Comments |
| Oxygen | Hypoxemia | Intranasal insufflation | 5-15 L/min | Aim for PaO2 >85 mm Hg, O2 sat >90% |
| Furosemide | Diuresis | Intravenous | 1 mg/kg | Repeat as needed; monitor acid-base status, hydration, and electrolyte concentrations |
| Furosemide | Bronchodilation | Nebulization | Will not be effective with concurrent NSAID administration | |
| Bronchodilators | Bronchodilation | Nebulization | See the Summer Pasture- | Many will be effective, described in |
| (various) | Oral Intravenous | Associated Obstructive Pulmonary Disease section | depth elsewhere | |
| Flunixin meglumine | Antiinflammatory | Intravenous | 1 mg/kg | bid; monitor renal function |
| Diphenhydramine | Antihistamine | Intravenous | 0.1-1 mg/kg | bid; monitor for excessive drowsiness |
| Epinephrine | Anaphylaxis | Intravenous | 3-5 mL IM for 450-kg horse | Use ONLY for treating anaphylaxis |
bid, Twice a day; IM, intramuscularly; NSAID, nonsteroidal antiinflammatory drug; O2 sat, percentage oxygen saturation; PaO2, partial arterial oxygen pressure.
oxygen saturation monitoring equipment (pulse oximetry) applied to the nasal mucosa, tongue, or other available nonpigmented mucous membrane.
In cases of NPPE, maintaining an adequate, low-resistance airway is very important to prevent further damage, and tracheostomy may be necessary. IV fluid therapy should be guided by the patient's needs and monitored by serial measurement of central venous pressure if necessary. Furosemide may be given intravenously or intramuscularly at a dose of 1 to 2 mg/kg and repeated in 1 hour (Table 31.11). If helpful, the dose can be titrated for each patient. At a dose of 1 mg/kg, approximately 8 L of urine is produced in approximately 1 hour.8 A few studies have been conducted on the effects of furosemide on pulmonary hemodynamics in the horse.8-12 Furosemide provides some relief to RAO-affected horses within 20 minutes of administration, increasing dynamic compliance without affecting PaO2.13 The beneficial effects appear to be mediated by prostaglandin E2 (PGE2), derived from either the renal or the airway epithelium, resulting in bronchial smooth muscle relaxation. Prior treatment with flunixin meglumine prevents the furosemide-induced bronchodilation.14 The effect in horses with pulmonary edema has not been reported. Colloid solutions should be administered cautiously or in conjunction with use of diuretics because they can initially increase vascular pressure. Plasma may be safer than other colloid preparations such as dextrans or hetastarch. Colloid solutions may be of little benefit in raising intravascular osmotic pressure in patients with increased microvascular permeability.Antiprostaglandin drugs (flunixin meglumine, phenylbutazone) and antihistamines may help and are indicated particularly in cases of anaphylactic reaction, as are diphenhydramine and epinephrine (see Table 31.11). Bronchodilators may be of benefit (see Table 31.11). The use of corticosteroids remains controversial; if they are used, antimicrobial coverage is advisable, as pulmonary edema has been shown to impair pulmonary bacterial defense mechanisms.