Thoracic Trauma
Scott M. Austin
Thoracic injuries in the horse are uncommon but are often associated with high mortality. These injuries result from either penetrating or blunt trauma.1,2 Collision with fences is the most common cause of penetrating thoracic wounds, but running into trees and farm implements, gunshots, goring by horned animals, and impalement by high-velocity debris during tornadoes have also been reported.3,4 While penetrating wounds are usually obvious, blunt force injuries can be more difficult to diagnose and may occur after collisions with stationary objects, kicks from other horses, and athletic mishaps such as falls.
Significant internal injuries may be present in the absence of external wounds.5 Frequently, damage occurs to both internal and external structures, and a complete physical examination and ancillary diagnostic tests are necessary to determine the extent of the damage. Potential trauma includes pectoral or axillary lacerations, penetrating wounds or impalement of the thorax, rib fractures, flail chest, and lung contusions or lacerations and leads to potentially life-threatening complications such as pneumothorax, pneumomediastinum, hemothorax, pleuritis, and diaphragmatic hernia.6,7External injury can cause extensive muscle damage, rib fractures, laceration of large vessels, and significant shock and pain. Internal injuries such as pneumothorax and thoracic hemorrhage will have the additional signs of respiratory distress characterized by nostril flaring, dyspnea, tachypnea, and exaggerated thoracic excursions.1,2 In addition, horses with diaphragmatic hernias may present with signs of abdominal discomfort.1-3 Patient stabilization to alleviate life-threatening complications must be undertaken first. Initial treatment ensures a patent airway, restores ventilation and oxygenation, controls hemorrhage, addresses shock, and reestablishes circulatory volume.7
After the patient is stabilized, a complete examination of the thorax will include careful auscultation and percussion, chest wall palpation, wound exploration, blood gas analysis, diagnostic thoracentesis, radiography, and ultrasonography.
Decreased lung sounds with increased resonance over the dorsal lung field is characteristic of pneumothorax, whereas diminished lung sounds with decreased resonance over the ventral thorax is characteristic of hemothorax or pleural fluid accumulation.2 Ultrasonography is extremely valuable for evaluation of the pleural space and lung surface and can detect air, blood, or fluid. Thoracentesis can be used in conjunction with ultrasound to further characterize any abnormalities. Arterial blood gas provides information regarding ventilation and oxygenation, and serial samples can be used to evaluate response to therapy. Because of the size of the equine chest, radiography usually requires referral to a hospital with equipment sufficient to image the equine thorax.Wounds of the Axilla
Deep wounds of the axilla occur frequently because of wire cuts, running into fences, or being impaled by sharp objects.6 Axilla wounds may cause direct penetration of the thorax or develop significant subcutaneous emphysema potentially leading to pneumomediastinum and pneumothorax.6,7 Wounds should be explored and thoroughly lavaged, but excessive pressure is discouraged, as this may drive contaminants further into the wound.6 To limit subcutaneous emphysema, wounds should be packed with gauze and a stent applied to hold packing in place. Packing should be changed every 24 to 48 hours until a granulation bed has formed.7 As with any wound, broadspectrum antibiotics, pain relief, and tetanus prophylaxis are recommended. Activity should be restricted, and cross-ties have been recommended. If severe subcutaneous emphysema develops, secondary pneumomediastinum and potentially pneumothorax may occur weeks after the initial injury.3
Penetrating Thoracic Wounds
When penetrating chest wounds are suspected, the clinician must perform careful auscultation and observe the respiratory cycle for several breaths. Splinting, paradoxical movement of a chest wall segment, and obvious incongruities of the chest wall suggest serious problems in ventilation.6,8 Careful palpation may identify local pain, fractures, flail segments, or subcutaneous emphysema.
Ultrasound can confirm abnormalities detected during physical examination.6 Serial exams are necessary, as signs of pneumothorax may take time to develop. If fullthickness penetration of the chest wall is suspected, arterial blood gases should be performed to evaluate oxygenation. Chest radiographs can be used to determine if pneumothorax, pneumomediastinum, or rib fractures are present.Pneumothorax
Pneumothorax is an uncommon event and is classified as open, closed, or tension.2,3,9,10 Penetrating wounds through the chest wall result in an open pneumothorax, and air moves freely into and out of the chest during inspiration and expiration. In contrast, the chest wall is intact in closed pneumothorax, and air entering pleural space originates from lung parenchyma secondary to infection, rib fractures, or ruptured lung bulla.6 Tension pneumothorax occurs when a one-way valve develops in either the chest wall or lacerated lung parenchyma. Air is drawn into the pleural space upon inhalation but does not escape during exhalation, resulting in intrapleural pressures that surpass atmospheric pressure and causing compromise of ventilation and cardiopulmonary collapse.5
In a review of 40 cases of pneumothorax in horses, the causes were divided between open and closed trauma and surgery of the upper and lower respiratory tract.10 Closed pneumothorax secondary to pleuropneumonia (17 of 40 cases)
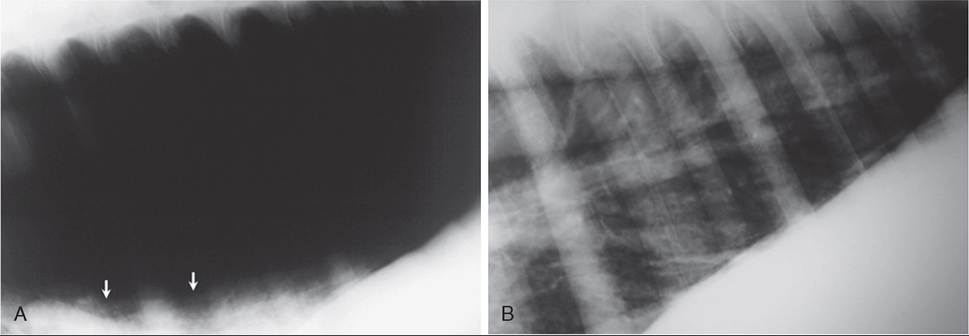
FIG. 31.32 A, Lateral radiograph of the caudodorsal thorax of a horse with bilateral pneumothorax. The dorsal borders of the lung margin are marked by arrows. B, Same view as A after thoracocentesis and resolution of the pneumothorax.
and blunt force trauma of the thorax (7 of 40) accounted for the majority. Penetrating wounds resulting in open pneumothorax accounted for 9 of 40 cases. Pneumothorax was bilateral in 19 of 40, unilateral in 17 of 40, and not stipulated as unilateral or bilateral in 4 of 40.10 Bilateral and tension pneumothorax compromise ventilation and result in obvious clinical signs, whereas unilateral pneumothorax is well tolerated in the horse.7 Unilateral pneumothorax is more likely encountered secondary to pleuropneumonia, whereas trauma usually results in bilateral pneumothorax.3,10 The survival rate was 69.6% for traumatic causes of pneumothorax as opposed to 35.3% for infectious causes.10 Clinical signs of pneumothorax include tachypnea, cyanosis, lack of lung sounds upon auscultation in the dorsal lung fields, fever, tachycardia, decreased activity, depression or anxiety, and cough. While history and clinical signs are suggestive, the diagnosis can be confirmed with radiography and ultrasonographic examinations.10 Thoracic radiographs are often not possible in the field, but ultrasonography can be used effectively.
Radiographic signs of pneumothorax include retraction of normal pulmonary parenchyma, hyperlucency within the caudodorsal thorax, and visualization of the dorsal margin of the lung lobes below the bodies of the thoracic vertebrae (Fig. 31.32). Radiography and ultrasonography have been reported to have 74% agreement, with most discrepancies occurring when the volume of air in the thorax was small.11 Ultrasonography is superior to radiography for detecting small volumes of air in the pleural space.12Normal aerated lung is characterized as a hyperechoic line on the ultrasound image. Ribs are visualized as hyperechoic curved lines that cast acoustic shadows. The appearance of two ribs with acoustic shadowing in the superficial plane and the pleural line deep is defined as the “bat sign.”12 Absence of the bat sign is characteristic of subcutaneous emphysema. Static images of air within the pleural space and the normal air-filled lung may appear similar; however, synchronous movement of the pleural line relative to the chest wall or “gliding lung sign” is characteristic of normal lung. Air that doesn't move with the respiratory cycle is seen with pneumothorax. M-mode ultrasonography can also be used to evaluate the pleural space. Normal lung on M-mode ultrasonography is represented by a series of horizontal lines representing the skin, muscular layers, and pleura. Below the pleura the normal lung appears as a granular layer. With pneumothorax, the granular layer is replaced by a continuum of horizontal lines above and below the pleura line.12 In experimentally induced pneumothorax, two-dimensional ultrasonography can detect as little as 50 mL of air within the pleural space and is superior

FIG. 31.33 Emergency stabilization of a horse with an open thoracic wound and subsequent pneumothorax. Plastic wrap has been placed around the chest to prevent air from entering the thoracic cavity, and a Heimlich drainage valve has been attached to the dorsally placed chest tube.
Intravenous fluids and intranasal oxygen are being administered.to M-mode ultrasonography and radiography for identification of pneumothorax.12
Arterial blood gas analysis should be performed when pneumothorax is suspected. Severe alterations indicate the need for immediate support of perfusion and ventilation. Pulse oximetry can provide a continuous indicator of response to treatment.6 Common complications include hypoxemia and possible metabolic and respiratory acidosis.13
Treatment for pneumothorax focuses on eliminating air from the pleural space and preventing recurrence. Obvious penetrating chest wounds should be sealed with a sterile, airtight dressing.2,4,7 Temporary wound closure, packing, petroleum dressings, and application of plastic wrap have been recommended to stop air leakage (Fig. 31.33). Stent bandages or complete circumferential bandages should be applied for added security of closure. However, bandages around the chest should not be used when flail chest is present.14 In most instances, pain is significant and can cause inadequate ventilation and hypoxemia (PaO2 4 mmol/L), venous oxygen tension (identification of minimally displaced rib fractures in adult horses may be difficult because of the large mass of the horse and superimposition of ribs on the opposite side. Indeed, in many instances, rib fracture may not be apparent until a callus has formed. Fortunately, single fractures appear to heal well without surgical intervention.2 Surgical intervention is reserved for displaced fractures that are a risk to lacerate lung, heart, or diaphragm.
Flail chest, while more common in neonates, is rarely observed in adult horses. Flail chest is defined as fracture of three or more ribs in at least two sites allowing a free-floating
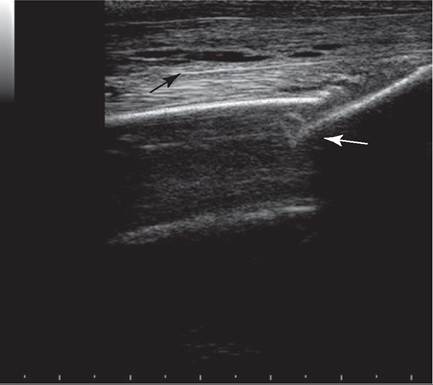
FIG. 31.34 Fractured rib (white arrow), saggital view.
Note the edema surrounding tissues (black arrow) and around the fracture site.rib segment and a characteristic paradoxical movement of the rib segment during respiration. The segment of chest wall moves inward during inhalation and outward during exhalation.6 Diagnosis is rare in the adult horse, as the trauma sufficient to cause a flail chest is often fatal. Flail chest causes severe respiratory compromise and often leads to severe hemorrhage due to trauma to the underlying heart and lung. Stabilization of the flail segment is essential, and suturing ribs in the affected segment to an external splint provides stability during healing.7
Abdominal Injury
When there is extensive thoracic trauma, the abdominal cavity should also be thoroughly evaluated. The cupula of the diaphragm can extend as cranial as intercostal space 6 during expiration, making the diaphragm vulnerable to injury with thoracic trauma. Diaphragmatic hernias can occur secondary to thoracic trauma but are rare.27 Clinical signs may include exercise intolerance, respiratory compromise, and tachypnea. In some horses, abdominal discomfort may dominate and be consistent with either a strangulating or nonstrangulating obstruction of the intestine.28-31 Thoracic radiography and ultrasonography may identify herniation of the diaphragm, and abdominocentesis may identify intestinal perforation or bowel rupture. Often tears are not identified until exploratory laparotomy, and they frequently occur along the ventral midline just dorsal to the xiphoid process.4 Conservative management of diaphragmatic hernias often results in euthanasia, so surgical repair is recommended.32,33 Multiple methods of surgical repair have been reported, and all require mechanical ventilation intraoperatively.27,32 Aftercare is similar to that for patients with colic; however, pneumothorax should be resolved before recovery.4
Summary
Injuries to the thorax of the horse can be managed with surgical or conservative strategies.3,',18,34 Initially patients require stabilization, and the extent and complicating factors of the wounds must be defined. Horses with simple rib fractures, small chest wounds, and modest pneumothorax or hemothorax are candidates for conservative management. Medical therapy includes broad-spectrum antibiotics and appropriate pain relief, thoracentesis or thoracic drain placement, second intention wound healing, and bandaging. More severe wounds require surgical intervention to exploration, lavage of wounds and body cavities, stabilization of fractures, control of hemorrhage, and removal of foreign bodies.34