REFERENCES
The complete list of references can be found at www.expertconsult.com.
REFERENCES
1. Code of Federal Regulations, Title 9, part 53. Animals and Animal Products. [WWW page].
https://www.gpo.gov/fdsys/pkg/CFR-2018-title9-vol1/xml/ CFR-2018-title9-vol1-part53.xml (Accessed 14 March 2018).2. The World Organization for Animal Health, Office of International Epizootics (OIE). [WWW page]. http://www.oie.int/animal-health-in-the- world/oie-listed-diseases-2018/ (Accessed 10 February 2018).
3. The USDA National Veterinary Accreditation Program. [WWW page]. https://www.aphis.usda.gov/aphis/ourfocus/animalhealth/nvap (Accessed 10 February 2018).
4. Emergency Management Institute: FEMA Independent Study Program: IS-700.A: National Incident Management System (NIMS), an introduction. [WWW page]. https://emilms.fema.gov/IS700aNEW/index.htm (Accessed 10 February 2018).
5. Center for Food Security and Public Health. [WWW page]. www.cfsph. iastate.edu (Accessed 10 February 2018). (Information and PowerPoint resources for a wide variety of transboundary, emerging, and zoonotic animal diseases, bio- and agroterrorism awareness education, biosecurity, and foreign animal disease preparedness.)
6. Foreign animal diseases: The Gray Book, revised 2008. [WWW page]. http://www.usaha.org/Portals/6/Publications/FAD.pdf (Accessed 10 February 2018). (Reference for foreign animal diseases organized by disease and including photos.)
7. USDA APHIS VS National Animal Health Emergency Response Corps. [WWW page]. https://www.aphis.usda.gov/aphis/ourfocus/animalhealth/ emergency-management/ct_naherc (Accessed 10 February 2018).
8. National Research Council of the National Academies: Animal health at the crossroads: preventing, detecting and diagnosing animal diseases, Washington,
rι δ>.administered intramuscularly generally induce a greater serologic response when an initial series of three doses is given rather than the two-dose series recommended by most vaccine manufacturers.
Whereas a 3- to 4-week interval between the first and second doses of vaccine is generally appropriate, a longer interval of 3 to 5 months between the second and third doses appears to optimize priming of the immune system and protection.The primary role of authorities charged with licensing vaccines in North America has traditionally been to ensure vaccine purity and safety, with less emphasis placed on documentation of efficacy.3-5 Consequently, little published information was available in the past documenting the efficacy of most vaccines licensed in North America. The situation has improved substantially in recent years, to the extent that published efficacy data are available for almost all equine vaccines licensed in North America since 1999. Field experience and some experimental evidence suggest that the efficacy of vaccines directed against different diseases varies considerably and that efficacy also varies among the vaccines from different manufacturers directed against the same disease.6-8
Vaccination is unlikely to confer protection more durable than that produced by recovery from natural disease, especially when the route of vaccination (usually IM) is different from the route of natural infection; this is because vaccines frequently do not evoke the full array of protective immune responses induced by natural infection.9,10 For example, the efficacy and durability of protection induced by parenteral vaccines against respiratory tract pathogens are frequently questioned.4,5,10 In part, this reflects the fact that parenterally administered vaccines are generally poor inducers of the local mucosal immune responses that are important for effective protection against infection of the respiratory tract.4,9,10 In addition, immunity achieved after natural infection with some respiratory tract pathogens is short lived.
Considerations for Use of Vaccines in Broodmares
The primary goals of vaccination programs for broodmares are (1) prevention of diseases that pose a risk to the mare or her fetus and (2) maximizing the level of colostral antibodies that will be passively absorbed by the neonatal foal after nursing, thus providing it with protection against diseases that pose a risk during the first few months of life.
Additional considerations in selecting vaccines for use in pregnant mares include (3) safety to the mare and fetus, (4) the potential for interference between multiple vaccines administered simultaneously, and (5) the influence of pregnancy on vaccine responses.PROTECTING THE MARE AGAINST DISEASES THAT POSE A RISK TO THE MARE OR HER FETUS. Broodmares are at risk of exposure to the same diseases as performance and pleasure horses, so they should be regularly vaccinated against all core and specific risk-based diseases according to published recommendations. The high horse traffic and high concentration of foals and young horses that typify many breeding farms contribute to a high risk of exposure to contagious respiratory diseases, including equine herpesvirus (EHV)-4, EHV-1, influenza, and strangles. Inclusion of influenza in vaccination protocols for broodmares is routinely recommended, and addition of EHV-4 and strangles vaccines is frequently recommended when conditions of significant risk are anticipated. Vaccination of mares against equine viral arteritis (EVA) before breeding may be indicated when they are to be bred to a known or suspected EAV carrier stallion, by either natural cover or artificial insemination. Whereas protection of the broodmare, fetus, or herdmates against the abortifacient effects of EHV-1 or EAV is the primary goal underlying inclusion of these antigens in vaccination protocols for broodmares, the goal of protecting the foal features at least as prominently in the rationale for vaccinating mares against tetanus toxoid, West Nile virus (WNV), eastern equine encephalitis (EEE) virus, western equine encephalitis (WEE) virus, rabies virus, equine influenza virus, equine herpesvirus-1 (EHV-1), EHV-4, and S. equi. Inclusion of rotavirus and botulism vaccines in protocols for pregnant mares is directed almost exclusively at protecting the young foal against these diseases.
MAXIMIZING MATERNALLY DERIVED ANTIBODY TRANSFER. Maintaining consistent broodmare vaccination protocols, which typically include administration of booster doses of vaccines during the last 2 months of gestation, will not only protect the mare but also maximize the likelihood that a uniformly high level of maternally derived antibody (MDA) transfer and passive protection will be achieved within the foal crop.
This is particularly important for diseases that pose a risk to the foal during the first few weeks of life. Whereas intranasally administered vaccines may afford good protection to the mare, they are typically less effective than parenterally administered inactivated vaccines in stimulating high levels of circulating immunoglobulin (Ig)G, the isotype that is passively transferred to the foal in highest concentration. Parenterally administered vaccines are preferred over intranasally administered vaccines for vaccination of mares during late gestation.VACCINE SAFETY IN BROODMARES. Consideration of vaccine safety in broodmares must take into account risks to the pregnancy and safety to the fetus. Potential adverse effects of vaccines on pregnancy are difficult to document even when large numbers of mares are used, unless obvious problems occur. Because fetal organogenesis occurs early in gestation, and this period is also characterized by substantial embryonic loss, even in normal mares it is sound practice to avoid administering vaccines to mares during the first 60 days of gestation unless conditions of imminent risk prevail. Few vaccines carry specific label recommendations for use in pregnant mares, and little published data exist to specifically document the safety of equine vaccines during pregnancy. Licensed vaccines that carry label recommendations for use in pregnant mares include two inactivated EHV-1 vaccines (Pneumabort-K+1b [Zoetis, Parsippany, NJ] and Prodigy [Merck Animal Health, Madison, NJ]) marketed for use in pregnant mares as an aid in prevention of EHV-1 abortion, the Calvenza line of inactivated influenza (Calvenza-03 EIV [equine influenza virus]), EHV-1 (Calvenza EHV), and influenza/EHV-1 combination (Calvenza-03 EIV/EHV) vaccines from Boehringer Ingelheim (Ingelheim am Rhein, Germany), one multivalent vaccine (Vetera Gold) from Boehringer Ingelheim containing Eastern and Western Encephalomyelitis virus, WNV, tetanus toxoid, EHV-1, EHV-4 and equine influenza virus, one inactivated Neorickettsia risticii vaccine (Equine Potomavac [Merial, Lyon, France]), one vaccine licensed for prevention of type B botulism in foals (BotVaxB [Neogen, Lansing, Mich.]), and one Leptospira pomona vaccine (LEPTO EQ INNOVATOR [Zoetis]) for the prevention of leptospiremia.
One conditionally licensed vaccine (Equine Rotavirus Vaccine [Zoetis]) for prevention of rotavirus infection in foals is labeled for use in pregnant mares. Although not specifically labeled for administration during pregnancy, widespread use in practice over many years has failed to document that any of the inactivated vaccines currently marketed for use in horses pose an unacceptable risk to pregnant mares. Therefore pregnant mares are routinely vaccinated with inactivated vaccines directed against tetanus toxoid, EEE virus, WEE virus, WNV, equine influenza virus, EHV-4, Streptococcus equi and, to a lesser extent, Neorickettsia risticii, rabies virus, and Venezuelan equine encephalitis (VEE) virus. Similarly, adverse impacts on pregnancy have not been documented for modified live, intranasally administered S. equi (Pinnacle I.N. [Zoetis]) and equine influenza virus (Flu-Avert [Merck Animal Health]) vaccines or the modified live, parenterally administered EHV-1 vaccine (Rhinomune [Boehringer Ingelheim]). Safety of the recombinant WNV and influenza vaccines (Recombitek [Merial]) should not be a significant concern, because the modified live canarypox vector lacks the ability to infect mammalian cells. In addition, the equivalent canarypox-vectored influenza vaccine (ProteqFlu [Merial]) marketed in the United Kingdom is labeled for use during pregnancy. Although the Flavivirus chimera WNV vaccine (PreveNile [Merck Animal Health]) was not specifically labeled for use during pregnancy while it was on the market, more than 300 pregnant mares were vaccinated during safety trials for licensing, without apparent adverse effects on the conceptus. In contrast, modified live virus (MLV) VEE vaccines and live anthrax spore vaccines should not be used in pregnant mares. Protection of mares against the potential abortigenic effects of EVA infection is best accomplished by completing the primary immunization series before the mare enters the broodmare band and by administering subsequent boosters during the open period before rebreeding.11The practice of booster vaccinating mares against multiple equine pathogens to maximize colostral transfer of antibodies to the foal results in the typical broodmare receiving multiple doses of many vaccine antigens and adjuvants during her lifetime.
In addition to stimulating high levels of antibody against a range of antigens, this practice may also predispose these mares to a higher rate of local and systemic adverse reactions, an issue that not only warrants further investigation but may force horse owners and veterinarians to carefully consider strategies for revaccination.POTENTIAL INTERFERENCE BETWEEN MULTIPLE ANTIGENS ADMINISTERED CONCURRENTLY. The possibility that “competition” between multiple antigens will compromise the response to some or all of the administered antigens should be considered. When administration of multiple vaccines late in gestation is indicated, it is good practice to administer no more than four antigens at one time and to allow an interval of 3 to 4 weeks between administering different vaccines.
INFLUENCE OF PREGNANCY ON VACCINE RESPONSES. It is widely assumed that pregnant mares are fully capable of mounting appropriate cellular and humoral immune responses to vaccines, but this issue has received little research attention. Mares that have been primed before breeding appear to mount appropriate anamnestic responses to vaccines, but preliminary data suggest that the humoral response to primary vaccination with several inactivated vaccines, including WNV and rabies virus, may be downregulated during gestation, resulting in failure of some vaccinated mares to passively transfer specific antibodies to the foal via colostrum.
Vaccination of Foals and Influence of Maternal Antibodies on Vaccine Responses
MDAs and perhaps other immune effectors (e.g., lymphocytes) that are concentrated in colostrum and are passively transferred to the foal play a crucial role in defense against pathogens encountered during the first few months of life while endogenous immune function continues to mature. Passive transfer of MDAs should therefore be exploited in immunization programs for foals by consistently administering booster doses of selected vaccines to mares 4 to 8 weeks before foaling and by ensuring that foals ingest adequate amounts of high-quality colostrum within 24 hours of birth. Besides passively protecting the foal, MDAs may also exert a profound inhibitory effect on the active immune response of the foal to antigens, including those contained in vaccines. This phenomenon is known as maternal antibody interference.
Several studies reported during the 1990s brought this issue into focus by demonstrating that foals younger than 6 months of age consistently failed to mount serologic responses to inactivated influenza vaccines.12-18 Of potentially greater concern was the finding that a high proportion of foals vaccinated under the cover of MDAs not only failed to seroconvert in response to the recommended primary series of two or three doses of influenza vaccine but also failed to respond to multiple additional doses administered during the next year, suggesting induction of a potentially detrimental immunotolerance-like phenomenon.15,16,19 Our studies confirmed an apparent lack of response of foals to multiple doses of inactivated influenza vaccines when the hemagglutination inhibition (HI) test was used to detect serologic responses, but responses were detected when the same samples were assayed using a sensitive isotype-specific ELISA. Rather than representing true tolerance, it appears MDAs may cause misdirection of the immune response away from the more important virus neutralizing IgGa and IgGb subisotypes in favor of the less effective IgG(T) subisotype of IgG.12 Subsequent studies in which titers of total rather than antigen-specific IgG subisotypes were determined documented that the age-related increase in concentrations of IgGb lagged significantly behind increases in concentrations of other isotypes and remained below adult levels beyond 6 months of age.20
Maternal antibody interference has now been documented to be a significant issue for many other antigens, including tetanus toxoid, EEE virus, WEE virus, EHV-1, and EHV-4, contained in vaccines administered to foals.12,21-25 Even low levels of antibody below those detectable by many routine serologic tests and below those thought to be protective can completely block the serologic response to some vaccines, resulting in a potentially prolonged period of susceptibility before the foal is capable of responding appropriately to vac- cines.24 These findings also indicate that it is not typically feasible to serologically test samples from foals to predict whether they will respond to particular vaccines. We now recommend that primary immunization with most vaccines containing inactivated antigens should be delayed until foals are 6 months of age or older, and with the exception of the rabies vaccine, three doses of vaccine should be included in the primary series rather the two doses routinely recommended by vaccine manufacturers. Typically, the third dose stimulates a serologic response of greater magnitude and durability than two doses and may also contribute to a higher “set point” for the response to subsequent booster doses.12,24,26,27 In contrast to the results cited, maternal antibodies do not appear to exert a marked inhibitory effect on the immune response of foals to the inactivated, live recombinant, live chimera, or DNA WNV vaccines, thereby permitting antibody-positive foals as young as 3 months of age to be immunized successfully.26,28,29 Similarly, the canarypox-vectored recombinant influenza vaccine has been shown to efficiently prime foals in the presence of MDA.30
Study results should be interpreted with caution because only humoral responses are typically assessed in MDA interference studies, and infectious challenge is not performed to confirm that lack of serologic response equates to lack of protection. Lack of a serologic response may correlate well with lack of protection for some diseases and some vaccines, whereas for others this may not be the case. In contrast, the presence of a serologic response may not correlate well with protection, as is frequently the case for respiratory tract pathogens. Because many commercially available vaccines are inactivated, adjuvanted, and administered by IM injection, they have limited potential to stimulate cellular and mucosal responses, so serologic responses induced by these vaccines likely correlate well with their potential to induce protection. In turn, MDA interference with serologic responses to inactivated vaccines likely equates to failure to induce protection. In contrast, failure to detect a serologic response to a modified live, vectored, DNA, or mucosally administered vaccine may not equate to lack of protection, because vaccines of these types induce a broader array of systemic and local responses that may not be affected by MDAs.
If MDA interference were not an issue, the approach to vaccination of foals would be greatly simplified because primary vaccination against all of the important diseases could be completed before MDAs had declined to nonprotective levels. In effect, the “window of susceptibility” would be eliminated. In reality, an attainable goal is to maximize the beneficial effects of MDAs while minimizing their negative impact on primary immunization. To best meet this goal, it is necessary to decide which one (or both) of the following is the primary focus: (1) to protect the foal and weanling against specific high-risk infectious diseases that affect this age group and have the potential to cause significant disease, either directly or by predisposing to other secondary infections, or (2) to initiate primary immunization to protect against disease later in life.
Assessing risk takes into account both the likelihood the foal will become infected and the risk of serious sequelae or death if the horse does become infected and does develop disease. If the disease affects the foal early in life, such as is the case with rotavirus (RV) infection, there is usually insufficient time to induce a protective immune response by actively immunizing the foal. Under these circumstances, the approach should be to maximize the degree of protection passively transferred from the dam via colostrum. Other diseases like rabies can affect horses of all ages, but the risk of acquiring infection is generally low.
Diseases of Moderate to High Risk to Young Foals but Low Risk to Adults
Diseases of moderate to high risk to young foals but low risk to adults include equine rotavirus infection (on certain breeding farms in certain years) and, in geographic areas such as Kentucky and some other Eastern states, type B botulism. For these diseases, the following approach is appropriate:
• Booster-vaccinate the dam before foaling to maximize uniformity of passive transfer.
• Ensure good passive transfer of maternal antibodies.
• Introduce management practices to reduce exposure to the infectious agent.
• Vaccinate the foal if risk continues beyond the first few months of life.
Diseases of Moderate to High Risk for Weanlings and Older Horses but Lower Risk to Young Foals Born to Vaccinated Mares
Diseases of moderate to high risk for weanlings and older horses but lower risk to young foals born to vaccinated mares include EHV-4, EHV-1, strangles, influenza, tetanus, EEE, and WNV infection. For these diseases, the following approach is appropriate:
• Vaccinate the dam before foaling to maximize uniformity of passive transfer.
• Ensure good passive transfer of maternal antibodies.
• Start foal vaccination after the risk of maternal antibody interference is no longer present in most foals. When several vaccine types are available for a particular disease, the vaccine that is least subject to MDA interference should be used. Introduce management practices to reduce exposure to the infectious agent while primary vaccination is being completed.
• If a two-dose primary series is recommended for adult horses, use three or more doses of vaccine in the primary series to improve the chances that foals that do not respond to earlier doses will respond to additional doses administered later.
Diseases of Low Risk to Foals
Diseases of low risk to foals in most circumstances include rabies, equine neorickettsiosis (EN), WEE, and EVA. For these diseases, the following approach is appropriate:
• Vaccinate the dam before foaling if the disease is a significant risk to adult horses and a vaccine shown to be safe for use in pregnant mares is available. If the available vaccines are not considered safe for use in pregnant mares, administer boosters before breeding.
• Ensure good passive transfer of maternal antibodies.
• Start foal vaccination after the risk of maternal antibody interference is no longer present in any foal (typically 9 months to 1 year of age)
Adverse Reactions to Vaccines
Though uncommon, the possibility always exists for adverse reactions (including anaphylaxis) associated with vaccine administration, so vaccines should be administered by or under the direct supervision of a veterinarian. Adverse reactions should be reported to the vaccine's manufacturer and the U.S. Department of Agriculture (USDA) (1-800-752-6255) or the U.S. Pharmacopeia (USP) Veterinary Practitioners Reporting Program (forms may be obtained or reports submitted by calling the USP at 1-800-487-7776). Anaphylaxis constitutes a life-threatening emergency requiring prompt treatment with epinephrine (1 mg/mL; equivalent to 5 to 10 mL of a 1 mg/mL dilution IM for a 450-kg horse). Repeated doses of epinephrine can be administered at 15-minute intervals if necessary. It has recently been shown that horses vaccinated with viral vaccines can develop IgE responses to nontarget antigens, including bovine serum albumin (BSA), suggesting that subsequent administration of another viral vaccine containing the same component could elicit an adverse response, including anaphylaxis.31
Local irritant tissue reactions occur more frequently, particularly when polyvalent combination vaccines and injectable strangles vaccines are used. These reactions are usually selflimiting, but resolution can be promoted by parenteral or oral (PO) administration of nonsteroidal antiinflammatory drugs (NSAIDs), topical application of warm compresses or the cutaneously absorbed NSAID diclofenac (Surpass [IDEXX Pharmaceuticals, Greensboro, N.C.]), and gentle exercise. Significant reactions in the neck muscles may make the horse reluctant to lower or raise its head; feed and water buckets should be positioned accordingly. Occurrence of externally visible local reactions can be reduced by administration of the vaccine deep in the semimembranosus and semitendinosus muscles of the hindleg rather than in the neck and by allowing the horse to exercise after vaccination. Horses that repeatedly react to polyvalent vaccines may benefit from the administration of NSAIDs or antihistamines before vaccination, administration of the individual antigenic components separately in different sites, use of a different brand of vaccine, use of a vaccine that can be administered by a route other than IM, or use of a vaccine that contains a different adjuvant or no adjuvant at all.
Some horses develop transient self-limiting systemic signs that may include fever, anorexia, lethargy, colic, diarrhea, tachycardia, and congested mucous membranes after IM administration of vaccines. Systemic signs are perhaps more common with certain vaccines but can be associated with any vaccine.32,33 In addition, inactivated Immune Stimulating Complex (ISCOM) and live recombinant vectored tetanus and influenza combination vaccines have been shown to elicit a prominent acute phase inflammatory response of several days' duration in vaccinated horses.34 A similar response likely occurs with other vaccines. It is therefore inadvisable to give horses any injectable vaccine within 2 weeks before a show, performance event, sale, or prolonged transportation. It may also be beneficial to minimize environmental dust when vaccinating horses known to have allergic airway disease or hypersensitivity.32
If unacceptable reactions occur repeatedly, the need for continued annual or more frequent revaccination against individual antigens should be carefully reevaluated, taking into account risk of disease balanced against the risk of an adverse reaction. Many horses that experience adverse reactions have received numerous doses of multiple vaccine antigens, repeated over the years. In this situation, the vaccination protocol should be “pared down” so that only the most essential antigens are administered and the maximum possible interval between boosters is employed. For diseases like rabies and tetanus, for which resistance can reasonably be correlated with circulating antibody titer, one possible approach to define the maximum or optimal interval between booster doses would be to measure the antibody titer. Unfortunately, this approach is currently limited by the paucity of laboratories that offer this type of testing on a routine basis, inexpensively, and with a short turnaround time. Introduction of commercially available ELISA testing for antibodies to the SeM protein of S. equi (Equine Diagnostic Solutions, Lexington, Ky.) and neutralizing antibody testing for WNV virus (Cornell University, Colorado State University, the University of Florida, and the USDA Animal and Plant Health Inspection Service [APHIS] National Veterinary Services Laboratory) in recent years has made it possible to refine vaccination protocols for these diseases in horses that experience adverse reactions to vaccination. Testing for rabies antibodies is available through Kansas State University, and testing for antibodies to other pathogens may be available through state diagnostic laboratories.
Available Vaccines and the Concept of Core and Noncore Vaccines
Fully licensed vaccines are now available in North America as aids to the prevention of tetanus; viral encephalomyelitis (EEE, WEE, VEE); WNV infection; influenza; EHV-1 and EHV-4 infection; strangles; rabies; EVA; EN; and type B botulism. In addition, conditionally licensed vaccines are available to immunize horses against rotavirus, equine rhinitis A virus (ERAV), and Corynebacterium pseudotuberculosis. Tetanus, rabies, and viral encephalomyelitis caused by EEE, WEE, and WNV pose a threat to horses in all geographic areas and are therefore considered to be core diseases against which all horses in North America should be vaccinated. The abortigenic potential of EHV-1 warrants inclusion of this disease in the core for all pregnant broodmares. Although influenza is not routinely included as a core disease, vaccination against this highly contagious respiratory tract infection is strongly recommended for all horses likely to be colocated with horses from other facilities during transportation or at sales, shows, trail rides, races, or other events. The remaining diseases for which vaccines are available are considered “noncore” or “risk based.” Indications for use of vaccines against these diseases are discussed in relevant sections that follow later in this chapter. Table 48.1 details the types of vaccines licensed for use in horses in the United States. Tables 48.2 through 48.4 provide general guidelines for use of the most frequently indicated equine vaccines in foals, weanlings, yearlings, and adult horses under various management conditions and in various geographic locations.
Vaccination Recommendations for Specific Diseases
Tetanus
All horses are at risk for developing tetanus, an often fatal disease caused by a potent neurotoxin elaborated by the anaerobic spore-forming bacterium Clostridium tetani. Infection of tissues typically occurs via puncture wounds (particularly those involving the foot or muscle), open lacerations, surgical incisions, exposed tissues like the umbilicus of foals, and the reproductive tract of the postpartum mare (especially in the event of trauma or retained placenta). C. tetani is present in the intestinal tract and feces of horses, other animals, and human beings, and spores are abundant, as well as ubiquitous, in soil. Spores of C. tetani survive in the environment for many years, resulting in an ever-present risk of exposure of horses and people on equine facilities. Because tetanus is expensive to treat and has a high mortality rate, all horses should be actively immunized using tetanus toxoid as part of the core vaccination program. Active immunization reduces the need to administer tetanus antitoxin, the use of which is associated with the risk of inducing potentially fatal serum hepatitis.
Protection against tetanus is mediated by circulating antibodies; toxin binding inhibition (ToBi) antibody titers of greater than 0.2 IU/mL are considered to be protective in the horse.27,35 The many available vaccines are formalin- inactivated, adjuvanted toxoids that are inexpensive, safe, and potent antigens that induce an excellent serologic response and solid long-lasting immunity when administered according to manufacturer recommendations. Primary immunization involves administration of two doses of toxoid at 3- to 6-week intervals. Titers of specific antibody increase to protective levels within 14 days after administration of the second dose in the primary Text continued on p. 1612
■ TABLE 48.1
Types of Equine Vaccines Licensed in the United States
Dead Vaccines Live Vaccines DNA
| Disease | Inactivated | Subunit | Modified Live Recombinant | Vaccine | |
| Tetanus | X | ||||
| Western equine encephalitis (WEE) | X | ||||
| Eastern equine encephalitis (EEE) | X | ||||
| Venezuelan equine encephalitis (VEE) | X | ||||
| West Nile | X | X, X (chimera) | X | ||
| Equine influenza | X | X | X | ||
| Equine herpesvirus 1 | X | X | |||
| Equine herpesvirus 4 | X | ||||
| Strangles | X | X | |||
| Equine viral arteritis | X | ||||
| Rabies | X | ||||
| Equine neorickettsiosis (Potomac horse fever) | X | ||||
| Botulism | X | ||||
| Rotavirus (conditional license) | X | ||||
| Equine rhinitis A virus (conditional license) | X | ||||
| Anthrax | X | ||||
| Leptospira interrogans serovar Pomona | X | ||||
| Corynebacterium pseudotuberculosis bacterin-toxoid | X | ||||
(conditional license)
■ TABLE 48.2
Guidelines for Vaccination of Adult Horses, Excluding Broodmares, Against Core and Noncore (Risk-Based) Diseases
■ TABLE 48.2
Guidelines for Vaccination of Adult Horses, Excluding Broodmares, Against Core and Noncore (Risk-Based) Diseases—cont'd
| Disease/Vaccine | Adult Horses (>1 Year of Age) Previously Vaccinated Against Disease Indicated | Adult Horses (>1 Year of Age) Not Previously Vaccinated Against Disease Indicated or Lacking Vaccination History | Comments | |
| Rabies | Inactivated: annual | Inactivated: 1-dose primary series | Booster vaccination induces persistently | |
| revaccination | Annual revaccination | elevated levels of antirabies antibody. | ||
| Noncore (Risk-Based) Vaccinesb | ||||
| Anthrax (rarely | Live spore vaccine: | Live spore vaccine: 2-dose | Use only in endemic areas or in the face of an | |
| indicated) | annual | primary series; second dose | outbreak. Antimicrobial drugs must not be | |
| revaccination | 3-4 weeks after first dose | given concurrently with this vaccine. | ||
| Annual revaccination | Administer subcutaneously in neck. Use caution during storage, handling, and administration. Consult a physician immediately if human exposure to anthrax vaccine occurs by accidental injection, ingestion, or otherwise through conjunctivae or broken skin. | |||
| Botulism | Toxoid: annual | Toxoid: 3-dose primary series; | ||
| revaccination | second dose 4 weeks after first dose; third dose 4 weeks after second dose Annual revaccination | |||
| Equine herpesvirus | Inactivated or | Inactivated or modified live: | A 6-month revaccination interval is | |
| (EHV) | modified live: semiannual (6-month interval) to annual revaccination (see comments) | 3-dose primary series; second dose 4-6 weeks after first dose; third dose 4-6 weeks after second dose | recommended for: • Horses revaccination to maximize immunity before expected peak challenge in summer and fall is the preferred approach if vaccination is elected as an adjunct to strategic environmental control measures. | |
| Rotavirus | Not applicable | Not applicable | ||
| Strangles | Inactivated M-protein | Inactivated M-protein subunit | Vaccination is not recommended as a strategy | |
| subunit or modified | vaccines: 2- to 3-dose series; | in outbreak mitigation, but vaccination may | ||
| live intranasal | second dose 2-4 weeks after | be warranted on farms with endemic | ||
| vaccines: | first dose; third dose (when | strangles, with the understanding that the | ||
| semiannual to | recommended by | risk of adverse vaccine reactions is higher in | ||
| annual revaccination | manufacturer) 2-4 weeks after the second dose. Revaccinate semiannually. Modified live intranasal vaccine: 2- dose primary series administered IN; second dose 3- 4 weeks after first dose Revaccinate semiannually to annually. | exposed horses. | ||
| Leptospirosis | Inactivated vaccines: annual revaccination | Inactivated vaccines: 2-dose primary series; second dose 3-4 weeks after first dose Revaccinate annually. | ||
aCore vaccines protect against diseases that are endemic to a region, are virulent or highly contagious, pose a risk of severe or fatal disease, have potential public health significance, and/or are required by law. Core vaccines have clearly demonstrable efficacy and have a sufficiently high level of patient benefit and low level of risk to justify their use in all equids in North America.
bNoncore (risk-based) vaccines are selected for use on the basis of assessment of risk performed by, or in consultation with, a licensed veterinarian. Use of noncore vaccines will vary among individuals, populations, and/or geographic regions.
Modified with permission from recommendations developed by the AAEP Infectious Disease Committee and posted on the AAEP website (aaep.org).
■ TABLE 48.3
Guidelines for Vaccination of Broodmares Against Core and Noncore (Risk-Based) Diseases
| Disease/Vaccine | Previously Vaccinated Broodmares | Broodmares Not Previously Vaccinated or Lacking Vaccination History | Comments |
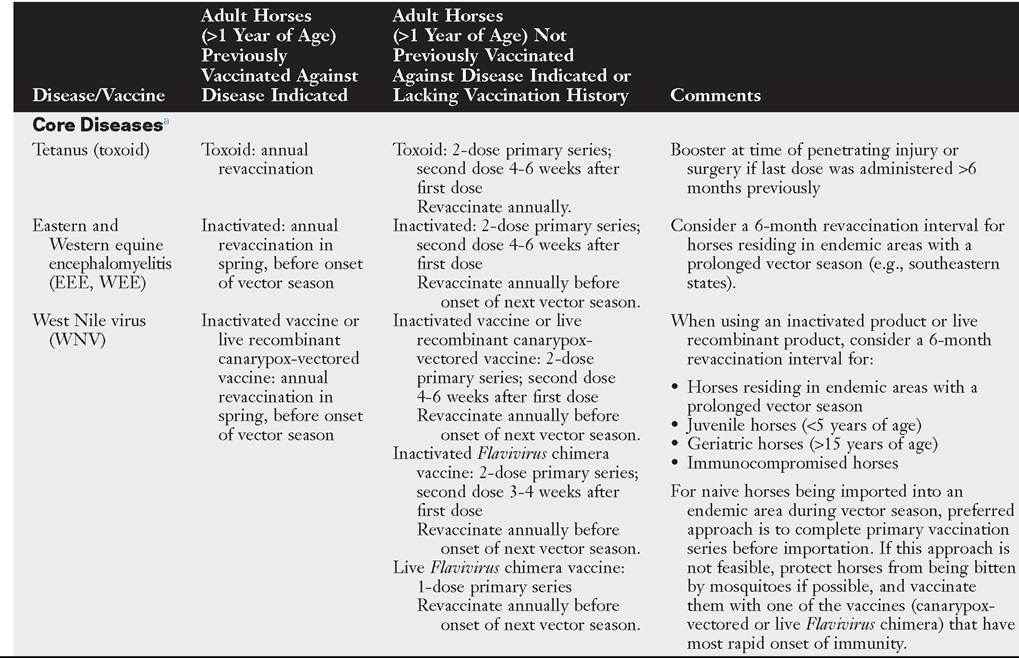
| Core Diseases3 | |||
| Tetanus | Toxoid: annual | 2-dose primary series; second dose 4-6 | Booster at time of penetrating |
| revaccination 4-6 weeks | weeks after first dose | injury or surgery if last dose | |
| prepartum | Revaccinate 4-6 weeks prepartum, depending on timing of second dose. | was administered more than 6 months previously | |
| Eastern and | Annual, 4-6 weeks | 2-dose primary series; second dose 4 weeks | Consider a 6-month revaccination |
| Western equine | prepartum | after first dose | interval for mares residing in |
| encephalomyelitis | Revaccinate 4-6 weeks prepartum, | endemic areas with a prolonged | |
| (EEE, WEE) | depending on timing of second dose. | vector season (e.g., southeastern states). | |
| ■ TABLE 48.3 | |||
| Guidelines for Vaccination of Broodmares Against Core and Noncore (Risk-Based) Diseases—cont'd | |||
| Broodmares Not Previously | |||
| Previously Vaccinated | Vaccinated or Lacking Vaccination | ||
| Disease/Vaccine | Broodmares | History | Comments |
| West Nile virus | Annual, 4-6 weeks | It is preferable to vaccinate naive mares | When using an inactivated |
| (WNV) | prepartum | when open. When risk is high, initiate | product or live recombinant |
| primary series as follows: | product, consider a 6-month | ||
| Inactivated vaccine or live recombinant | revaccination interval for mares | ||
| canarypox-vectored vaccine: 2-dose | residing in endemic areas with | ||
| primary series; second dose 4-6 weeks | a prolonged vector season. | ||
| after first dose | For naive mares being imported | ||
| Revaccinate 4-6 weeks prepartum, | into an endemic area during | ||
| depending on timing of second dose. | the vector season, preferred | ||
| Inactivated Flavivirus chimera vaccine: | approach is to complete the | ||
| 2-dose primary series; second dose 3-4 | primary vaccination series | ||
| weeks after first dose | before importation. If this | ||
| Revaccinate annually, before onset of | approach is not feasible, | ||
| the next vector season. | protect them from being bitten | ||
| Live Flavivirus chimera vaccine: 1-dose | by mosquitoes if possible, and | ||
| primary series | vaccinate them with one of the | ||
| Revaccinate 4-6 weeks prepartum, | vaccines (canarypox-vectored | ||
| depending on timing of first dose. | or live Flavivirus chimera) that have the most rapid onset of immunity. | ||
| Rabies | Annual, before breeding | 1-dose primary series | Booster vaccination induces |
| OR 4-6 weeks | Annual revaccination before breeding OR | persistently elevated levels of | |
| prepartum | 4-6 weeks prepartum | antirabies antibody. This vaccine may be given post foaling but before breeding to reduce the number of vaccines | |
| given to mares prepartum. | |||
| Equine herpesvirus | 3-dose series with | 3-dose series with product labeled for | |
| (EHV) | product labeled for | prevention of EHV-1 abortion | |
| prevention of EHV-1 | Administer during the fifth, seventh, and | ||
| abortion Administer during fifth, | ninth months of gestation. | ||
| seventh, and ninth months of gestation. | |||
| Noncore (Risk-Based) Vaccinesb | |||
| Anthrax | Not recommended for | Not recommended for use during gestation | |
| use during gestation | |||
| Botulism | Annual, 4-6 weeks | 3-dose series: first dose during eighth | |
| prepartum | month of gestation; second dose 4 weeks after first dose; third dose 4 weeks after the second dose | ||
| Equine influenza | Inactivated vaccines: | Inactivated vaccine: 3-dose primary series; | The MLV intranasal influenza |
| semiannual, with 1 | second dose 4-6 weeks after first dose; | vaccine can be used to protect | |
| dose administered 4-6 | third dose 4-6 weeks prepartum | pregnant mares against | |
| weeks prepartum | Canarypox-vectored vaccine: 2-dose | influenza, but its use for | |
| Canarypox-vectored | primary series; second dose 4-6 weeks | prepartum booster is not | |
| vaccine: semiannual, | after first dose but no later than 4 weeks | recommended because it does | |
| with one dose | prepartum | not reliably stimulate high | |
| administered 4-6 weeks | levels of circulating antibody. | ||
| prepartum | Administration of an inactivated or canarypox- vectored vaccine for the | ||
| prefoaling booster is the preferred approach. | |||
| Equine viral | Administration during | Administration during pregnancy is not | Mares potentially intended for |
| arteritis (EVA) | pregnancy is not | recommended unless risk of exposure is | export should undergo |
| recommended unless | high. | serologic testing immediately | |
| risk of exposure is high. | before initial vaccination and be confirmed negative for antibodies to EAV. | ||
Continued
■ TABLE 48.3
Guidelines for Vaccination of Broodmares Against Core and Noncore (Risk-Based) Diseases—cont'd
| Disease/Vaccine | Previously Vaccinated Broodmares | Broodmares Not Previously Vaccinated or Lacking Vaccination History | Comments |
| Equine | Semiannual, with one | 2-dose primary series: first dose: 8-10 | Strategic environmental control |
| neorickettsiosis | dose administered 4-6 | weeks prepartum; second dose 4-6 weeks | measures are important for |
| (Potomac horse fever) | weeks prepartum | prepartum | effective control. |
| Rotavirus | 3-dose series: first dose at 8 months’ gestation; second dose 4 weeks after first dose; third dose 4 weeks after second dose | 3-dose series: first dose at 8 months’ gestation; second dose 4 weeks after first dose; third dose 4 weeks after second dose | Check serum concentration of immunoglobulin in foal to verify adequate passive transfer. |
| Strangles | Inactivated M-protein subunit vaccines: semiannual, with 1 dose given 4-6 weeks prepartum | Inactivated M-protein subunit vaccines: 3-dose primary series; second dose 2-4 weeks after the first dose; third dose 4-6 weeks prepartum | MLV intranasal strangles vaccine can be used to protect pregnant mares, but its use for the prepartum booster is not recommended because it does not reliably stimulate high levels of circulating antibody. Administration of an inactivated M-protein vaccine for the prefoaling booster is the preferred approach. |
| Leptospirosis | Inactivated vaccines: annual revaccination | Inactivated vaccines: 2-dose primary series; second dose 3-4 weeks after first dose Revaccinate annually. | Inactivated vaccine can be used in pregnant mares in all 3 trimesters of gestation. |
aCore vaccines protect against diseases that are endemic to a region, are virulent or highly contagious, pose a risk of severe or fatal disease, have potential public health significance, and/or are required by law. Core vaccines have clearly demonstrable efficacy and have a sufficiently high level of patient benefit and low level of risk to justify their use in all equids in North America.
bNoncore (risk-based) vaccines are selected for use on the basis of assessment of risk performed by, or in consultation with, a licensed veterinarian. Use of noncore vaccines will vary among individuals, populations, and/or geographic regions.
Modified with permission from recommendations developed by the AAEP Infectious Disease Committee and posted on the AAEP website (aaep.org).
■ TABLE 48.4
Guidelines for Vaccination of Foals, Weanlings, and Yearlings Against Core and Noncore (Risk-Based) Diseases
| Disease/Vaccine | Foals and Weanlings (bgcolor=white>first dose at 3-4 months of | unknown vaccination | |||
| of age; second dose 4-6 | age; second dose 4-6 weeks | history, either follow | |||
| weeks after first dose; | after first dose (not necessary | approach outlined for | |||
| next dose at 10-12 | if dam is seronegative); next | foals of vaccinated mares | |||
| months of age | dose at 10-12 months of age | or determine serologic status of foal (or mare) | |||
| and use results to classify foal as either being from a vaccinated or unvaccinated mare. | |||||
| Noncore (Risk-Based) Vaccinesb | |||||
| Anthrax (rarely | Not applicable because | No age-specific guidelines are | Annual, in | Anthrax vaccination is | |
| indicated) | vaccination of pregnant | available for this vaccine. | spring | rarely indicated—only in | |
| mares is not | Manufacturer’s | focal endemic areas. | |||
| recommended | recommendation is for | Antimicrobial drugs must | |||
| primary series of 2 doses | not be given concurrently | ||||
| administered subcutaneously | with this vaccine. | ||||
| (in the neck) at a 2-3-week | Exercise caution during | ||||
| interval. | storage, handling, and administration of this live | ||||
| bacterial product. Consult a physician immediately should accidental human | |||||
| exposure (via mucous membranes, conjunctivae, or broken skin) occur. | |||||
| Botulism (type B | 3-dose primary series: | 3-dose primary series: first | Annual | Limited information | |
| toxoid) | first dose as early as | dose as early as 1-3 months | suggests that maternal | ||
| 2-3 months of age; second dose 4 weeks | of age; second dose 4 weeks | antibody does not | |||
| after first dose; third dose 4 | interfere with | ||||
| after first dose; third | weeks after second dose | vaccination, so foals at | |||
| dose 4 weeks after | high risk may be | ||||
| second dose | vaccinated as early as 2 weeks of age. | ||||
| Equine herpesvirus | Inactivated EHV-1, | Inactivated EHV-1, EHV-1/4, | Semiannual | The benefit of intensive | |
| (EHV) | EHV-1/4, or modified | or modified live EHV-1 | (6-month | vaccination programs | |
| live EHV-1 vaccine: | vaccine: 3-dose primary | interval) | directed against EHV-1 | ||
| 3-dose primary series; | series; first dose at 4-6 | and EHV-4 in foals and | |||
| first dose at 4-6 months | months of age; second dose | young horses is not | |||
| of age; second dose 4-6 | 4-6 weeks after first dose; | clearly defined because, | |||
| weeks after first dose; | third dose 3-4 months after | despite frequent | |||
| third dose 3-5 months | second dose (i.e., 10-12 | vaccination, infection and | |||
| after second dose (i.e., 10-12 months of age) | months of age) | disease continue to occur. It is difficult to induce | |||
| active immunity before weanlings experience | |||||
| field challenge. | |||||
■ TABLE 48.4
Guidelines for Vaccination of Foals, Weanlings, and Yearlings Against Core and Noncore (Risk-Based) Diseases—cont'd
| Disease/Vaccine | Foals and Weanlings (bgcolor=white>Comments | |||
| Equine influenza | Inactivated vaccine: | Inactivated vaccine: 3-dose | Semiannual | An unusually high risk of |
| 3-dose primary series; | primary series; first dose at | (6-month | exposure may warrant | |
| first dose at 6-7 months | 6-7 months of age; second | interval) | vaccination of younger | |
| of age; second dose 4-6 | dose 4-6 weeks after first | Semiannual | foals. Because potentially | |
| weeks after first dose; | dose; third dose at 10-12 | (6-month | interfering maternal | |
| third dose at 10-12 | months of age | interval) | anti-influenza antibody is | |
| months of age | Live canarypox-vectored | Semiannual | likely to be present, a | |
| Live canarypox-vectored | recombinant vaccine: 3-dose | (6-month | complete primary | |
| recombinant vaccine: 3-dose primary series: first dose at 5-6 months of age; second dose 5 weeks after first dose; third dose at 10-12 months of age Modified live cold- adapted intranasal vaccine: 1-dose primary series: first dose at 11 months of age If vaccination earlier than 11 months is elected, use a 2-dose primary series: first dose at 6-10 months of age; second dose at 11-12 months of age | primary series; first dose at 5-6 months of age; second dose 5 weeks after first dose; third dose at 10-12 months of age Modified live cold-adapted intranasal vaccine: 1-dose primary series: first dose at 11 months of age If vaccination earlier than 11 months is elected, use a 2-dose primary series: first dose at 6-10 months of age second dose at 11-12 months of age | interval) | vaccination series should be given after 6 months of age. The modified live intranasal vaccine is licensed for administration to horses 11 months of age or older with a label recommendation of 1 dose for primary immunization. If vaccine is given before 11 months of age, a second dose should be administered at 11 months or older. | |
| Equine viral | Colt (male) foals: single | Colt (male) foals: single dose at | Annual for | Before initial vaccination, |
| arteritis (EVA) | dose at 6-12 months of | 6-12 months of age (see | colts | colt (male) foals should |
| age (see comments) | comments) | intended for use as breeding stallions | undergo serologic testing and be confirmed negative for antibodies to EAV. Maternally derived anti-EAV colostral antibodies can persist in foal for up to 6 months, so testing and vaccination should not be performed before 6 months of age. Keep colts isolated for 3 weeks after vaccination. | |
| Equine | 3-dose primary series: | 3-dose primary series: first | Semiannual to | If warranted by risk, |
| neorickettsiosis | first dose at 5-6 months | dose at 5-6 months of age; | annual | vaccine may be |
| (Potomac horse | of age; second dose 3-4 | second dose 3-4 weeks after | administered to younger | |
| fever) | weeks after first dose; third dose at 10-12 months of age | first dose; third dose at 10-12 months of age | foals, in which case additional doses should be administered at 4-week intervals until foal is 6 months of age. | |
| Rotavirus | Not recommended in foals | Not recommended in foals | Not applicable |
Continued
■ TABLE 48.4
Guidelines for Vaccination of Foals, Weanlings, and Yearlings Against Core and Noncore (Risk-Based) Diseases—cont'd
| Disease/Vaccine | Foals and Weanlings (permission from recommendations developed by the AAEP Infectious Disease Committee and posted on the AAEP website (aaep.org). series and, in adult horses, persist at detectable levels for 12 months or longer, depending on the adjuvant system used in the vaccine.27,35-37 A recent study documented substantial differences between currently licensed combination tetanusencephalomyelitis vaccines with regard to the magnitude of the vaccine-induced tetanus-specific IgGb and IgG(T) antibody responses.8 The vaccine containing a Carbopol adjuvant induced substantially higher antibody titers than those containing either saponin or squaline combined with surfactants.8 Revaccination once annually is recommended. No published challenge studies are available to document the speed of onset or duration of protection induced by tetanus toxoid preparations currently licensed in North America. Conclusions regarding their efficacy are therefore based on the serologic response obtained in horses and laboratory animals and on field experience. However, a challenge study conducted in Europe over 60 years ago found that horses were resistant to challenge 8 days after receiving a single injection of tetanus toxoid, before antibody could be detected in their serum.38 A second study demonstrated that a series of three doses of tetanus toxoid induced protection lasting for at least 8 years, and perhaps for life, even when antibodies could no longer be detected.35 A recent study in Europe documented that protective levels of antibody (>0.2 IU/mL as measured by tetanus toxin-binding ELISA) persist for at least 18 months after revaccination of horses previously primed with a two-dose series of a tetanus toxoid/influenza ISCOM vaccine.39 In contrast, tetanus has been documented in vaccinated horses in North America,40 although survival was strongly associated with previous vaccination. Thus, it would not be prudent to recommend extension of the annual interval for revaccination with tetanus toxoid products available in North America, pending publication of data documenting duration of immunity (DOI). Vaccinated horses that sustain a wound or undergo surgery more than 6 months after receiving their previous tetanus booster should be revaccinated with tetanus toxoid immediately at the time of injury or surgery. Annual revaccination of pregnant mares should be completed 4 to 8 weeks before foaling to protect the mare if she sustains foaling-induced trauma or retained placenta and to enhance concentrations of specific immunoglobulins in colostrum. Colostrum-derived antibodies significantly interfere with the immune response of foals vaccinated with tetanus toxoid until they are about 6 months old.12,36 Primary vaccination of foals that have received appropriate transfer of colostral antibodies from a vaccinated mare should include three doses of tetanus toxoid beginning at age 6 months or older. Optimally, the interval between the first two doses of vaccine should be approximately 4 weeks, and the interval between the second and third doses should be 3 to 5 months. The three-dose primary series is recommended for foals because a high proportion of foals fail to seroconvert in response to two doses of tetanus toxoid regardless of whether maternal antibodies are detectable at administration of the first dose.12,36 For foals born to nonimmune mares, this initial three-dose series can start at 1 to 4 months of age. Tetanus antitoxin is produced by hyperimmunization of donor horses with tetanus toxoid. Administration of 1 vial of antitoxin (1500 IU) to nonvaccinated horses induces immediate passive protection that lasts not more than 3 weeks.36 More prolonged protection may be accomplished with higher doses. In addition to the use of high doses of tetanus antitoxin to treat tetanus, indications frequently cited include administration to newborn foals born to unvaccinated mares and to unvaccinated horses that sustain an injury. In these cases the concurrent administration of tetanus antitoxin and tetanus toxoid at different sites using separate syringes has been advocated, followed by administration of additional doses of toxoid at 4- to 6-week intervals to complete the primary series.41 Because a small but significant number of horses experience serum sickness and fatal hepatic failure (serum hepatitis) several weeks 4243 after receiving tetanus antitoxin,42,43 a preferred approach to the unvaccinated horse that sustains a puncture or deep laceration is to thoroughly clean and debride the wound, initiate active immunization by administering tetanus toxoid, and institute a course of antimicrobial treatment with penicillin or alternate antimicrobial that is active against C. tetani. Equine Encephalomyelitis (Sleeping Sickness) The equine encephalomyelitis viruses (EEE, WEE, and VEE) belong to the Alphavirus genus of the family Togaviridae. They are transmitted by mosquitoes (and infrequently by other bloodsucking insects) to horses from wild birds or rodents that serve as natural reservoirs for these viruses. Risk of exposure and geographic distribution of the encephalomyelitis viruses vary by season and from year to year with changes in distribution of insect vectors and wildlife reservoirs. The distribution of EEE has historically been restricted to the eastern, southeastern, and some southern states, with recent northward encroachment. WEE has caused minimal disease in horses in North America during the past 3 decades, but the virus continues to be detected in mosquitoes and birds throughout the western states. In the past, outbreaks of WEE have been recorded in the western and midwestern states, with sporadic cases in the northeastern and southeastern United States. Because EEE, WEE, or both are endemic in most areas of North America, vaccination against these diseases should be part of the core vaccination program for all horses. VEE is a reportable foreign animal disease. Epidemics of VEE occur when the virus undergoes genetic change and develops greater virulence for avian and mammalian hosts. These viral variants are able to multiply to high levels in the horse, and then the horse becomes a reservoir for infection in these outbreaks. VEE occurs in South and Central America but has not been diagnosed in the United States or Mexico for many years; routine vaccination of horses in these regions against VEE is not recommended at this time unless transportation to endemic areas is planned. Available vaccines are formalin-inactivated, adjuvanted, bivalent or trivalent, whole-virus products containing EEE, WEE, and VEE virus, typically in combination products containing other antigens such as tetanus toxoid, influenza virus, WNV, or EHV-1/-4. Although correlates for protection against EEE, WEE, and VEE are not well established, circulating antibodies are assumed to be important because infection is acquired by vascular injection (mosquito bites), and current inactivated vaccines appear to have good efficacy.44,45 A study evaluating the serologic response of horses to commercial encephalomyelitis-tetanus combination vaccines showed that the EEE neutralizing antibody responses to Encevac T (Merck Animal Health, Carbopol adjuvant) and Equiloid Innovator (Zoetis, squaline and surfactant adjuvant) were of greater magnitude and persistence than responses to Cephalovac EWT (Boehringer Ingelheim, saponin adjuvant).8 However, no comparative randomized challenge studies have been performed using these vaccines to document whether differences in serologic responses equate to differences in efficacy. Early testing of bivalent (EEE/WEE) vaccines was performed by intracranial challenge with either EEE or WEE; the formalin- inactivated preparations demonstrated 100% protection. Primary immunization of unvaccinated adult horses is accomplished by administering two doses of inactivated vaccine 3 to 6 weeks apart. In areas where EEE is not a threat and mosquito vectors are active for less than 6 months of the year, annual revaccination in the spring, before the peak insect vector season, is recommended. In areas like the Gulf States where EEE is endemic and mosquitoes are active virtually year-round, many veterinarians prefer to revaccinate horses semiannually to ensure more uniform protection throughout the year. Inactivated encephalomyelitis vaccines are considered safe for use during pregnancy, so booster vaccination of pregnant mares 4 to 8 weeks before foaling is routinely recommended to enhance colostral concentrations of specific immunoglobulins. Neutralizing antibodies to WEE and EEE are transferred passively to foals through colostrum and decline with an estimated half-life of 33 and 20 days, respectively. MDAs appear to confer protection and are detectable in the serum of many foals from vaccinated mares for at least 3 months and up to 7 months, depending on the postnursing titer.23,46-48 Several studies have shown that MDAs exert a profound inhibitory effect on the ability of foals to mount serologic responses to inactivated bivalent WEE/EEE vaccines, which likely accounts for some of the reported cases of vaccine failure and resultant clinical EEE in vaccinated horses, particularly those younger than 2 years of age.19,23,24,46,4' Studies have shown that 3-month-old foals born to immune mares consistently failed to mount a serologic response to two doses of inactivated bivalent WEE/EEE vaccine, and the majority had not responded even after administration of a third dose.24,26 Whereas many 6-month-old foals failed to seroconvert after administration of two doses of vaccine, most responded following administration of a third dose.24 On the basis of these data, inclusion of a third dose in the primary series, 2 to 5 months after administration of the second dose, is strongly recommended for primary immunization of foals and yearlings. WEE has a lower mortality rate than EEE, and prevalence of WEE in many western states is sufficiently low that the risk of foals acquiring infection during their first year of life is also low. Therefore primary vaccination of foals of vaccinated mares in areas where mosquitoes die off in the winter and the risk of infection is low is best completed when foals are 5 to 6 months of age or older in order to minimize the potential for MDA interference. Because foals born in the late spring and summer months are still younger than 6 months of age by the time the mosquito season comes to an end in many regions, primary vaccination of these foals can be delayed until the spring of the yearling year. In contrast, EEE is a highly fatal disease that poses a significant risk to foals during their first year of life, particularly in the Gulf States where competent vectors are present year-round.19,47,49 Most veterinarians in these regions recommend commencing primary vaccination of foals at 3 to 4 months of age using a three-dose primary series, followed by a fourth dose before the onset of the next mosquito season and semiannual boosters thereafter to maximize the chances of overcoming the inhibitory effects of MDAs and inducing protection.47 West Nile Virus Only a few years after WNV infection was first diagnosed in horses in the northeastern United States in 1999, it had spread across the entire North American continent and is now considered endemic in all mainland areas of North America and Mexico, where it has become an important consideration in the differential diagnosis of horses presenting with signs of neurologic disease. Since 1999, the disease has been confirmed in more than 25,000 U.S. horses, about 35% of which have died or been euthanized. Roughly 40% of horses that survive acute illness caused by WNV exhibit residual effects (e.g., gait and behavioral abnormalities) 6 months post diagnosis.50 WNV, a member of the family Flaviviridae, is transmitted by mosquitoes and infrequently by other bloodsucking insects to horses, human beings, and a number of other mammals from avian hosts, which serve as natural reservoirs for these viruses. Horses and humans are considered to be “dead-end” hosts of WNV and therefore do not contribute to the transmission cycle. The virus is not directly contagious from horse to horse or from horse to human. Similarly, indirect transmission via mosquitoes from infected horses is highly unlikely because horses do not experience a significant level of viremia.51 Risk of infection and death appears to increase with increasing age, but the disease has been confirmed in foals as young as 3 weeks of age. Although cases have been seen virtually year-round in the southeastern United States, the risk of acquiring infection is highest during those months in which mosquito activity peaks, typically July, August, September, and October in most areas of North America. WNV infection is a core disease against which all horses residing in the continental United States and Canada should be vaccinated. As of April 2013, six WNV vaccines (West Nile-Innovator [Zoetis], Recombitek Equine rWNV vaccine [Merial], Equi-Nile [Merck Animal Health], Vetera WNV Vaccine [Boehringer Ingelheim], PreveNile [Merck Animal Health], and West Nile-Innovator DNA [Zoetis]) are licensed for use in horses in North America. All six vaccines have met USDA requirements for safety in tests, each involving more than 640 horses. West Nile-Innovator is an inactivated whole-virus vaccine that contains a metabolizable oil adjuvant.52 This vaccine is available as either a monovalent (single-component) vaccine or as several multicomponent vaccines containing other encephalitis virus antigens (EEE, WEE, VEE) and tetanus. Recombitek Equine rWNV vaccine is a Carbopol-adjuvanted canarypox-vectored recombinant modified live vaccine,53-55 which is also available as a multicomponent containing inactivated EEE, WEE, and tetanus antigens. PreveNile is a nonadjuvanted chimeric yellow fever 17D-vectored vaccine.56-59 This vaccine was voluntarily withdrawn from the market in May of 2010 after an unacceptably high number of adverse reactions were reported and has not yet been reintroduced. Merck Animal Health has since produced and tested an inactivated version of this chimera vaccine, which was released in 2011 as a single-component vaccine (Equi-Nile), as well as several multicomponent vaccines that also contain EEE, WEE, tetanus, EHV-1, EHV-4, and influenza antigens (Encevac + WNV; Encevac T + WNV, and Prestige V + WNV). Similarly, the Vetera line of vaccines from Boehringer Ingelheim includes both single and multicomponent (up to 8 components) versions containing an inactivated WNV antigen. West Nile-Innovator DNA is a plasmid DNA vaccine with a metabolizable oil adjuvant.28 It appears that Zoetis is not currently marketing this vaccine. Needle and mosquito challenge models have shown that West Nile-Innovator, Recombitek, and West Nile-Innovator DNA all significantly reduce the magnitude of viremia in experimentally infected vaccinated horses compared with nonvaccinated control horses for as long as 12 months after 285253 primary vaccination with two doses of vaccine. ’ ’ Although viremia was reliably induced in nonvaccinated control horses in these challenge models, clinical disease was not. Therefore these vaccines are labeled as aids to the prevention of viremia due to WNV infection. In contrast, an intrathecal challenge model that reliably induced severe clinical disease was used to test the efficacy of PreveNile in studies for licensure.57 In this model, a single dose of PreveNile prevented clinical disease, as well as viremia in 4- to 6-month-old horses challenged 1 year after vaccination; therefore PreveNile was labeled for protection against viremia and as an aid in the prevention of disease and encephalitis caused by WNV.57 Subsequently, Recombitek was shown to induce a high level of clinical protection when tested using this rigorous intrathecal challenge model in a placebo-controlled study in which horses were challenged 14 days after completion of a two-dose vaccination series.54 The comparative efficacy of West Nile-Innovator, Recombitek, and PreveNile has now been tested in a randomized blinded, placebo-controlled intrathecal challenge study in which groups of 5 or 6 horses 6 months of age or older were challenged intrathecally 28 days after completion of the two-dose (West Nile-Innovator and Recombitek) or 1-dose (PreveNile) primary vaccination series.60 In this study, all six unvaccinated control horses developed grave neurologic signs post challenge, whereas all vaccinated horses survived and none developed detectable viremia. Clinical disease was prevented in 100% of PreveNile- vaccinated horses, 80% of Recombitek-vaccinated horses, and 33% of Innovator-vaccinated horses.60 These findings support the results of field studies that provide clear evidence that when used according to manufacturer recommendations, all available licensed WNV vaccines reduce the risk of disease and death after natural challenge, although clinical disease may not be fully prevented with all vaccines.61-65 Directions for primary immunization using inactivated whole virus, inactivated Flavivirus chimera, and recombinant vaccines include administration of two doses of vaccine 3 to 6 weeks apart (consult the specific label). Optimal protection cannot be expected until 2 weeks after administration of the second dose, although Recombitek has been shown to induce significant protection as early as 26 days after administration of the first dose when tested in both the mosquito challenge and intrathecal challenge models.54,55 Primary immunization with PreveNile requires 1 dose. A challenge study in yearlings showed that 83% (5 of 6) were protected when challenged intrathecally 10 days after vaccination with one dose, indicating that onset of immunity is rapid.57 Rapid onset of immunity is an important feature when faced with the challenge of protecting naive horses that are being introduced into an endemic area, as is the case when horses from Europe and other nonendemic countries are imported into North America. Vaccine manufacturers recommend revaccination of previously vaccinated horses on an annual basis, or more frequently when local conditions are conducive to a prolonged period of potential exposure to infected mosquito vectors. Annual revaccination is best completed in the spring (late February through early April), before the onset of the insect vector season. In areas like the southeastern states, where the mosquito season is prolonged, revaccination twice annually, once in the spring and again in the late summer or early fall (late July through early September), has been advocated in the past to maximize protection, although the rationale for semiannual vaccination against WNV has not been tested in controlled studies. None of the licensed vaccines currently marketed in the United States carry label recommendations for administration to pregnant mares, so mares are best vaccinated before breeding whenever possible. It is well recognized, however, that pregnant mares are at risk of acquiring infection from infected mosquitoes. Consequently, it has become accepted practice by many veterinarians to administer vaccines to pregnant mares on the reasonable assumption that the risk of adverse consequences of WNV infection far exceeds the reported adverse effects of use of vaccines in pregnant mares. Thousands of doses of West Nile-Innovator vaccine have been administered safely to pregnant mares, and a published study failed to document vaccine-associated adverse effects in a large population of pregnant mares.66 Although the Recombitek vaccine is a live vectored vaccine, the canarypox vector is incapable of replication in mammals and does not induce a viremia that could infect a fetus. In addition, a canarypox-vectored influenza vaccine available in Europe is licensed for use in horses during pregnancy, so the vectored WNV vaccine is unlikely to be associated with an increased risk of adverse effects in pregnant mares. As with other vaccines, it is sound practice to avoid administering West Nile vaccines to mares during the first 60 days of gestation unless conditions of imminent risk prevail. Booster vaccination of previously primed pregnant mares 4 to 8 weeks before foaling appears to induce a strong anamnestic serologic response that provides their foals with passive colostral protection lasting at least 3 to 4 months.26 In contrast, a significant proportion of naive pregnant mares failed to seroconvert when the primary series of WNV-Innovator vaccine was administered during the second half of gestation, perhaps reflecting pregnancy-associated downregulation of Th2 responses.26 This observation adds further justification to the recommendation that when inactivated West Nile-Innovator vaccine is used, the primary series is best completed before breeding. In a similar study, pregnancy did not appear to suppress the response of mares to primary immunization with Recombitek (Wilson WD and colleagues, unpublished observations, 2007). In contrast to findings with many other vaccines in the foals of immune mares, MDAs do not block the response of foals as young as 3 months of age to vaccination with the inactivated West Nile Innovator vaccine or the recombinant, chimera, or DNA WNV vaccines.26,29 Although this finding is somewhat surprising for the inactivated vaccine, it might reasonably have been expected for the other vaccines, because the vector systems accomplish transfection of cells and expression of the major E-peptide and M-peptide antigens of WNV on the surface of antigen-presenting cells (APCs) in association with major histocompatibility complex (MHC) class I and class II antigens. These peptide antigens are therefore not free in the tissues and circulation to be neutralized by MDAs. The impact of MDAs on the recently marketed inactivated whole virus (Vetera WNV Vaccine [Boehringer Ingelheim]) and inactivated chimera vaccines (Equi-Nile [Merck Animal Health]) is not known. Primary vaccination of foals from properly vaccinated mares can be started by administration of the first dose of either an inactivated or recombinant vaccine as early as 3 to 6 months of age (consult the specific product label), followed by a second dose approximately 3 to 6 weeks later, and then a third dose 3 to 5 months after the second dose. This third dose increases the likelihood that foals with high MDA levels that may have attenuated the response to the first dose of vaccine will become primed and protected. Even in foals that have no maternally derived WNV antibodies after nursing, the third dose of inactivated vaccine in the primary series induces significantly higher and more persistent levels of antibody than two doses. A booster should be administered during the spring of the yearling year, after which the recommendations for vaccination of adult horses should be followed. Primary vaccination of foals from unvaccinated unexposed mares should commence at 3 months of age or younger (as early as 1 month of age), depending on month of birth and seasonal level of activity of mosquito vectors in the area. The three-dose primary vaccination protocol previously outlined should be followed. Revaccination should be performed before the onset of the next mosquito season. The influence of MDAs on the response of foals to PreveNile was recently evaluated in 3-month-old and 5-month-old foals vaccinated with a single dose. Although significant titer responses were not observed post vaccination, sensitization of cell-mediated responses was accomplished, as evidenced by significant increases in expression of granzyme B, interleukin (IL)-2, perforin, and transforming growth factor (TGF)-β and nonsignificant increases in interferon (IFN)-γ expression in WNV-stimulated PBMC from foals vaccinated at 5 months of age.29 Similar, although nonsignificant, trends were seen in 3-month-old foals.29 When available, PreveNile was labeled for administration of a single priming dose to foals 5 months of age or older, primarily because 5 months was the minimum age of foals used in challenge trials for licensure. Results of the previously cited study suggest that foals younger than 5 months of age could be immunized successfully with PreveNile. Regardless, a second dose of vaccine should be administered before the onset of the next mosquito season. Preliminary data suggest that the plasmid West Nile-Innovator DNA vaccine is able to circumvent the potentially interfering effects of MDA, but the vaccine was labeled for use in horses 8 months of age or older.28 As with EEE, horses that have recovered from clinical WNV infection will likely be protected for the reminder of their lives and should not need to be revaccinated unless changes in their immune status, as might occur with prolonged corticosteroid administration, alter their susceptibility to infection.67 It is remarkable that in little more than 10 years after WNV disease was first encountered in the Americas, six vaccines with documented efficacy based on challenge studies were licensed for the benefit of horses, including three that apply the most modern technologies available for either animals or humans at the time. Rabies Rabies is an infrequently encountered neurologic disease of equids resulting from inoculation of the rabies virus through the bite of infected (rabid) wildlife. Wildlife species that serve as the natural reservoirs for rabies virus differ among regions of North America but include raccoons, foxes, skunks, and bats. Horses most often sustain bites on their muzzle, face, or lower limbs. The rabies virus then migrates via nerves to the brain, where it initiates rapidly progressive encephalitis. Even though the incidence of rabies in horses is low, the disease is invariably fatal and has considerable public health significance. All horses kept in areas where rabies is endemic in the wildlife population are at risk and should be vaccinated as part of the core vaccination program. Therefore vaccination of horses against rabies virus is recommended by, or under the direct supervision of, a veterinarian using one of the three inactivated tissue culture-derived products currently licensed for use in horses (Rabvac3 [Boehringer Ingelheim], RM Imrab3 [Merial], and EquiRab [Merck Animal Health]). These vaccines are potent immunogens that induce strong serologic responses that peak within 28 days after IM administration of a single dose. Although correlates for protection against infection with rabies virus in horses are not well defined, it is logical to assume that protection correlates with titers of circulating antibody. In humans, postvaccination antibody titers are used to predict protection. In dogs, however, postvaccination serologic test results were not found to be completely predictive of resistance to challenge exposure during tests performed with certain inactivated vaccines.68 Challenge studies demonstrating efficacy are required for licensing of all rabies vaccines, including those labeled for use in equids in the United States. The challenge studies are conducted by the vaccine manufacturers as outlined in the Code of Federal Regulations (CFR) from the USDA. These studies indicate a DOI of 12 months, and a minimum of 80% of vaccinated animals must be resistant to severe challenge with the rabies virus. A DOI of 14 months was documented in a placebo-controlled challenge study in which 4-month-old foals were vaccinated with one dose of EquiRab and challenged by masseter injection of virulent rabies virus 14 months later (see product data sheet). For primary immunization, label directions on inactivated rabies vaccines licensed for use in horses suggest administration of one dose to horses aged 3 months or older followed by a second dose 1 year later. Thereafter, annual revaccination is recommended. Although none of the licensed vaccines carries a specific label approval for use in pregnant mares, it is important to acknowledge that only a limited number of equine vaccines are specifically licensed for use in pregnant mares and veterinarians do administer inactivated rabies vaccines to pregnant mares. Alternatively, veterinarians may recommend that mares be vaccinated against rabies before breeding in order to reduce the number and type of vaccines given in the period before foaling. Because rabies antibodies persist in serum for a prolonged period, foals born to mares that are revaccinated while open acquire substantial titers of rabies antibody after ingesting colostrum. Documentation of rabies in supposedly vaccinated horses, most of which were younger than age 2, brought into question the efficacy of label recommendations for primary vaccination of foals against rabies.69 Recent studies in our laboratory have shown that the serologic response of most 3-month-old foals from antibody-positive mares is completely blocked, even when a two-dose primary vaccination series is used. Although the response to the first dose of vaccine is typically blocked in 6-month-old foals from antibody-positive mares, these foals appear to seroconvert after administration of a second dose 4 weeks later. Primary vaccination of foals from vaccinated mares should therefore be delayed until they are 6 months of age or older and should include two doses of inactivated vaccine administered approximately 4 to 6 weeks apart, followed by a third dose at 1 year of age. For foals of mares known not to be vaccinated against rabies, the primary vaccination series can be started according to manufacturers’ recommendations as early as 3 months of age and may comprise only 1 dose, followed by a second dose at 1 year of age. For foals from mares of unknown vaccinal history, either of the two following options is rational and can be used: (1) Assume the mare to be antibody positive, and follow the previous recommendation for foals from mares known to be vaccinated against rabies, starting at 6 months of age. (2) Document the serum antibody status of the foal by testing serum collected from the foal at 24 hours of age or older or from the dam during the periparturient period, and determine which of the approaches to follow on the basis of the presence or absence of rabies antibodies. Equine Influenza Infection of the respiratory tract of horses with the orthomyxovirus influenza A/equine/2 (H3N8) remains one of the most common causes of rapidly spreading outbreaks of respiratory disease. The influenza A/equine/1 subtype (H7N7) has not been recognized as a cause of clinical disease for many years and is likely extinct in nature. Influenza is endemic in the equine populations of the United States and much of the world. Evidence of influenza infection has never been documented in resident horses in New Zealand and Iceland. Whereas outbreaks of influenza have previously been reported in Singapore, Japan, South Africa, and Australia, rigorous control measures have apparently been successful in eliminating the virus from these countries. Rapid national and international transportation of horses facilitates spread of the virus. Concentrating young horses at racetracks, training facilities, boarding stables, breeding farms, shows, or similar athletic events increases the risk of infection, as does a low serum concentration of specific antibody.70 Older horses are generally less susceptible to infection but may become ill when partial protection is overwhelmed by exposure to horses excreting large amounts of virus. Explosive outbreaks occur at intervals of several years when immunity of the equine population wanes and sufficient antigenic drift has occurred to generate a new viral strain. In contrast to herpesviruses, EIV is not maintained in asymptomatic carrier horses and does not circulate constantly, even within large groups of horses. Rather, the disease is introduced sporadically by a symptomatic or an asymptomatic infected horse. This epidemiologic finding and rapid elimination of the virus by the equine immune response suggest that infection can be avoided by preventing entry of the virus into an equine population (e.g., quarantine of newly arriving horses for at least 14 days) and appropriate vaccination.71 EIV is highly contagious and spreads rapidly through groups of horses in aerosolized droplets dispersed by coughing. Contaminated buckets, grooming or feeding equipment, tack, and transport vehicles may serve as fomites because the virus can survive for hours on such objects. Severity of clinical signs of influenza, which include nasal discharge, fever, lethargy, anorexia, cough, and myalgia, depends on the degree of existing immunity and other factors. Infected horses shed virus for up to 10 days in their nasal secretions. Inactivated vaccines do not induce sterile immunity, so recently vaccinated horses can become infected, shed virus, and contribute to interepidemic persistence of infection within the equine population and propagation of infection during outbreaks.6 Immunity to the same (homologous) strain of H3N8 virus after natural infection persists for more than a year and involves both local and systemic humoral and cellular mechanisms. These include induction of large amounts of virus-specific neutralizing IgG and secretory IgA antibody in nasal secretions, high levels of circulating IgG antibodies, and genetically restricted antigen-specific cytotoxic T lymphocytes (CTLs) that kill infected cells.72-76 Memory CTLs can be detected in peripheral blood for at least 6 months after infection, and solid immunity persists even when circulating antibody titers have declined to low or undetectable levels.73,74,77,78 Similarly, protection induced by the licensed modified live intranasal (IN) influenza vaccine (Flu-Avert I.N. [Merck Animal Health]) is presumably mediated through induction of local immune responses in the respiratory tract because this vaccine does not typically induce high levels of circulating antibodies.7,79 With the exception of ISCOM vaccines, inactivated vaccines administered by IM injection have limited potential to induce CTL or nasal secretory IgA responses and induce only low levels of neutralizing antibody in nasal secretions.’’’ The degree of protection induced by inactivated influenza vaccines is highly correlated with postvaccination titers of circulating antibody, predominantly of the IgGa and IgGb subisotypes, as measured by HI or single radial hemolysis (SRH) tests.70,82-84 SRH levels of 100 mm2 or greater are considered to be at least partially protective, but levels above 140 mm2 are required for successful prevention of disease.82 The partial protection induced by inactivated vaccines is of limited duration (up to about 7 months, depending on the vaccine) and is manifested as a reduction in clinical signs and attenuation of viral shedding in horses exposed to infection. 1,2 The magnitude of the serologic response to inactivated influenza vaccines depends on many factors, the most important of which are the quality and quantity (mass) of the viral antigen and choice of the adjuvant.82,85,86 Carboxypolymer-based compounds (carbomer, Carbopol) and ISCOMs are contained in some of the most efficacious inactivated influenza vaccines, whereas some commonly used adjuvants (e.g., alum) have been associated with induction of a nonproductive immune response.72,85 History of previous vaccination or infection, interval since the last dose of vaccine, antibody titer at the time of vaccination, age, maternal antibody status, and relatedness of the vaccine strain to circulating field strains of influenza virus are other important determinants of efficacy, at least for 84 87 88 inactivated influenza vaccines.’’ Antigenic drift of the A/equine/2 subtype has resulted from point mutations in the genes encoding the amino acid sequences of the hemagglutinin (H) and neuraminidase (N) glycoprotein antigens on the surface of the virus. The result is emergence of viral strains representing two antigenic lineages, American and Eurasian, of the H3N8 virus. Further antigenic drift within each lineage has generated variants that, as with the prototypical strain A/equine 2/Miami 63, are named according to the location and year in which they were first isolated. The American lineage further evolved during the 1990s into Kentucky, Florida, and South American sublineages.89 For the Florida sublineage, two clades have been identified: clade I, represented by Ohio 03 and South Africa 03, and clade II, represented by Richmond 07. According to the 2017 report of the OIE expert surveillance panel on EIV, only clades I and II Florida sublineage EIV strains are circulating worldwide. Clade I representatives of the Florida sublineage are present in North America, Europe, South Africa, and Japan, and clade II representatives are present in Europe, India, and China.89 Antigenic drift, by generating antigenically heterologous viruses, reduces the degree and duration of protection conferred by previous infection or vaccination because of the specificity of immunoglobulins, and it allows horses with high titers to become infected and develop clinical signs of disease if the vaccine strain is not closely related to the drifted infectious field strain.90 Although antigenic drift of EIV is slower than that of human influenza viruses, it is recommended that inactivated equine influenza vaccines include viral antigens from isolates obtained within the most recent 5 years. An expert surveillance panel meets annually to recommend strains that should be included in influenza vaccines in subsequent years (www.equiflunet.org.uk). In the past, federal U.S. regulations made updating of equine influenza vaccines through inclusion of recently isolated strains so costly and timeconsuming that vaccines typically lagged more than the recommended 5 years behind the antigenic drift of field viruses, resulting in suboptimal protection. Recent changes in vaccine licensing regulations should make more frequent updating of equine influenza vaccines feasible. Even though Flu-Avert I.N. contains only a 1991 H3N8 strain of North American lineage, it has been shown to be protective against challenge with Eurasian strains and recently isolated North American strains. The short-lived immunity after vaccination with inactivated equine influenza vaccines was the impetus for past recommendations for frequent revaccination, at intervals as short as 2 months. However, too short an interval may compromise efficacy because an optimal anamnestic response to influenza vaccination is inhibited in horses with a high antibody titer.91 An additional consideration that potentially limits the efficacy of influenza vaccines is the phenomenon termed original antigenic sin, whereby horses exposed to a drifted field A/equine/2 virus will mount an anamnestic immune response directed more strongly against the strain with which they were vaccinated initially than against the drifted field virus.86 A considerable amount of published efficacy data based on both challenge studies and field epidemiology studies has been available for many years in Europe to support the use of influenza vaccines. In contrast, information regarding the efficacy of influenza vaccines marketed in North America has remained sparse until recently. Furthermore, studies conducted in North America during the late 1990s showed that the inactivated influenza vaccines in use at the time failed to provide much benefit in terms of reducing the risk of infection and clinical disease during field outbreaks.6,70 Serologic testing performed during these and other studies indicated that vaccine failure was caused by failure of the influenza vaccines in use at the time to induce protective antibody titers.6,70,92 Fortunately, vaccine manufacturers in North America have responded to the challenge of producing more efficacious equine influenza vaccines during the past 15 years by incorporating more relevant recent viral strains, increasing antigenic mass of relevant strains, eliminating the seemingly irrelevant H7N7 strain, modifying adjuvant systems, and introducing novel technologies. An important advance occurred in 1999 when Heska Corporation marketed an attenuated live cold-adapted influenza vaccine (Flu-Avert I.N. [Merck Animal Health]) for IN administration. This vaccine, which contains a Kentucky/1991 strain of North American lineage, was found to be highly efficacious in blinded controlled challenge studies conducted 5 weeks, 6 months, and 1 year after administration of a single dose to naive horses.7 Subsequently, Flu-Avert I.N. was shown to cross protect against European H3N8 strains, as well as against North American strains isolated during the late 1990s and early 2000s, and to induce a rapid onset of protection within 7 days of administration of a single dose to naive horses.79,93 Although horses challenged 1 year after administration of a single dose showed a significant but only partial reduction in severity of clinical signs and virus shedding, a more marked reduction in clinical signs and viral shedding was found when the challenge was performed 6 months after vaccination.7 On the basis of these results, revaccination at 6-month intervals is recommended. Field experience indicates that this regimen induces solid clinical protection after natural challenge. Currently, Flu-Avert I.N. is licensed for use in nonpregnant horses 11 months of age or older, primarily because this was the youngest age of the horses used in the challenge studies for licensing. Horses may shed small amounts of vaccinal virus for several days after vaccination with Flu-Avert I.N., but the amount of virus shed is so low that in-contact horses will not generally become infected or immunized with vaccinal virus shed by recently vaccinated horses, and the likelihood of reversion to virulence is extremely low.94 In recent years, several vaccine manufacturers in North America have updated their inactivated vaccines and demonstrated efficacy in challenge studies. Inactivated influenza vaccines containing one or more relevant H3N8 strains are currently marketed by Boehringer Ingelheim (Calvenza EIV), Zoetis (Fluvac Innovator), and Merck Animal Health (Prestige II). These companies also market a large number of multicomponent combination vaccines that contain the same inactivated influenza antigens as in their single-component products but also contain tetanus, WEE and EEE virus, EHV, or WNV antigens. A study in which naive 9-month-old horses were challenged by aerosol with a recent influenza H3N8 strain (KY/99) 16 weeks after the last dose of a three-dose vaccination series (0, 4, and 16 weeks) documented that Calvenza EIV and two EIV/ EHV combination vaccines (Prestige II and Fluvac EHV-4/1) reduced clinical signs and viral shedding in vaccinated horses compared with nonvaccinated control horses.96 The group vaccinated with Calvenza EIV developed significantly higher serum antibody titers after vaccination and experienced less fever, nasal discharge, and viral shedding than horses vaccinated with either Prestige II or Fluvac EHV-4/1. On the basis of these findings, the authors concluded that Calvenza EIV, a vaccine developed, formulated, and efficacy tested according to European Union guidelines, was the most effective inactivated influenza vaccine available in North America at that time. This vaccine is adjuvanted with Carbopol and contains the KY/95 and Ohio 03 North American strains and the Newmarket 93 Eurasian H3N8 strains. The initial two doses of this vaccine are administered intramuscularly; subsequent doses may be administered intramuscularly or intranasally. It is proposed, but not proved, that administration of booster doses by the IN route may provide a stronger local mucosal immune response. This vaccine is licensed for use in horses older than 6 months of age, including pregnant mares. Only two commercially available EIV vaccines commercially available in North America (Vetera 2xp [Boehringer Ingelheim] and Prestige II [Merck Animal Health]) do follow the OIE recommendations by including contemporary relevant clades I and II EIV strains. Vetera 2xp contains representatives of both clade I (A/eq/Ohio/03) and clade II (A/eq/Richmond/1/07) Florida sublineage EIV, as well as an American lineage EIV strain (A/eq/Kentucky/95). The newly formulated Prestige II is the most recently updated EIV vaccine available in North America and contains A/eq/ Florida/13 (Florida sublineage clade I), A/eq/Richmond/1/07 (Florida sublineage clade II), and A/eq/Kentucky/02 (American lineage). The metabolizable oil (MetaStim) adjuvanted Fluvac vaccine evaluated in the challenge study mentioned previously contained the KY/92 strain of the H3N8 virus. This strain has since been replaced with a KY/97 strain, and the product is now named Fluvac Innovator. In 2006, Merial was granted a North American license to market an injectable canarypox-vectored recombinant equine influenza vaccine that has been used with success in Europe for several years. This vaccine, Recombitek Equine Influenza Virus vaccine, has been shown to induce strong protection in challenge studies and has the potential to positively impact influenza prevention in North America.95 The vaccine incorporates the HA gene from the Ohio 03 and Newmarket 93 H3N8 strains into the same vector delivery platform as the efficacious WNV virus vaccine (Recombitek) and contains a carbomer polymer adjuvant in the diluent.95 Consequently, this vaccine invokes a broad array of humoral and cellular immune responses. Challenge studies document onset of protection as soon as 2 weeks after completion of a two-dose primary series and persistence of solid protection for at least 5 months. Administration of a booster dose at 5 months induced a strong anamnestic response that provided solid protection persisting for at least 12 months.96 This vectored influenza vaccine can circumvent the inhibitory effect of maternal antibodies, an issue that significantly impacts primary immunization of foals using inactivated influenza vaccines.30 Recombitek Equine Influenza Virus vaccine is licensed for vaccination of healthy horses as young as 5 months of age. VACCINATION PROTOCOLS FOR INFLUENZA. Influenza should be considered a core vaccine on all facilities that are not totally closed so as to preclude contact with “outside” horses from other locations. As with other diseases, the full benefit of vaccination against influenza can be realized only if the primary vaccination series is completed, or if booster doses of vaccine are administered, several weeks before anticipated exposure. The following issues should be considered when planning an influenza vaccination program: (1) primary vaccination of adult horses, (2) routine revaccination, (3) vaccination of pregnant mares, (4) primary vaccination of foals, and (5) vaccination in an outbreak. Primary Vaccination of Adult Horses The following are options for primary vaccination of adult horses that have not previously been vaccinated: • Flu-Avert: administer a single dose intranasally. A second dose administered 3 months later may be beneficial, particularly for horses vaccinated at younger than age 11 months. • Inactivated intramuscularly administered vaccines: administer two doses 3 to 6 weeks apart according to label directions. Although not specifically recommended by some manufacturers, administration of a third dose of vaccine 3 to 5 months after the second dose is indicated because it significantly enhances the magnitude of the primary response and duration of persistence of antibodies at protective levels. • Recombitek Equine Influenza Virus vaccine: administer two doses 4 to 6 weeks apart, and revaccinate 5 months later. Routine Revaccination Improvements in injectable vaccines and introduction of new vaccine types during the past 10 years has extended the duration of clinical protection achievable through vaccination. A routine revaccination interval of 6 months appears to be appropriate for most of the influenza vaccines currently marketed in North America. This routine protocol should be customized by adjusting timing of boosters or inclusion of an additional booster to achieve maximum protection during periods when the risk of exposure is high. For example, strategic revaccination 1 month before being placed at high risk of exposure, such as at a show or sale or being transferred to a training or boarding facility, is justified to maximize protection. Vaccination of Pregnant Mares For the mare to produce colostrum that contains a high level of antibodies against equine influenza, she should be revaccinated 4 to 8 weeks before foaling with a vaccine that stimulates a robust serologic response. Although the intranasally administered Flu-Avert I.N. vaccine induces good protection, it does not routinely stimulate high levels of circulating antibody, at least when used for primary immunization. An inactivated injectable vaccine is therefore recommended for prefoaling booster vaccination of pregnant mares at this time.26 Vaccination of Foals The antibody status of a mare at the time of foaling is the main determinant of the postnursing circulating antibody titer in her foal and therefore has a profound impact on the ability of the foal or weanling to respond to influenza vaccines administered during the first year of life. Foals born to seronegative nonvaccinated mares respond appropriately to influenza vaccines, so primary vaccination can commence at 3 months of age or younger if significant risk of exposure to influenza exists. In contrast, maternal antibodies have been shown to completely block the serologic response of foals to a primary immunization series comprising two or more doses of inactivated influenza vaccines when the first dose is administered at 6 months of age or younger.12-18,24 Interference from MDA may persist until 9 months of age or beyond for foals with high antibody titers post nursing.12-18,24,26 Studies in Newmarket, United Kingdom, have shown that influenza virus infection is rare in Thoroughbred yearlings before they enter training, suggesting that the risk of influenza is low in horses younger than age 1 year born to 889798 mares in herds that are well vaccinated.’’ There appears to be little justification to vaccinate young foals from vaccinated mares against influenza, as was recommended in the past.48,99,100 The IN modified live vaccine (Flu-Avert I.N.) is licensed for vaccination of horses 11 months of age or older. Whereas this vaccine has been shown to be safe in foals as young as 2 months of age,101 published data regarding the potential for MDAs to interfere with the response are lacking. Unpublished observations suggest that MDA interferes with the response of foals between 3 and 6 months of age, whereas foals with maternal antibody vaccinated at 7 months of age were protected against virulent challenge (Holland and Chambers, personal communication). Pending publication of well-controlled studies, it is recommended that if the first dose of Flu-Avert I.N. vaccine is administered before 11 months of age, a second dose should be administered at 11 months of age or older.102 The European-licensed live canarypox-vectored recombinant influenza is labeled for use in pregnant mares and foals as young as 4 months.78 The North American-licensed Recombitek EIV vaccine has been shown to be safe in foals as young as 4 months, but the minimum age recommended for vaccination of foals from immunized dams is 5 months. The recombinant vaccine has been shown to efficiently prime foals aged 10 to 20 weeks that had detectable MDA at the time of vaccination.30 These foals showed clear evidence of an anamnestic antibody response when a secondary vaccination with the same vaccine was performed. The canarypox-vectored recombinant influenza vaccine therefore offers a unique opportunity to overcome the limitations of early-life vaccination in the face of maternally derived immunity in foals.30 If the foal experiences failure of passive transfer of maternal antibodies, or if the mare is seronegative for influenza, the manufacturer recommends commencing vaccination at 4 months of age and including an additional dose in the primary series. Vaccination in an Outbreak Definitive diagnosis of equine influenza infection should be pursued during outbreaks of suspected viral respiratory disease because specific measures can then be instituted to contain spread of the disease. Rapid (same-day) diagnosis of influenza can be accomplished using the highly sensitive and specific polymerase chain reaction (PCR) or antigen-capture ELISA tests. In addition, virus isolation should be pursued during outbreaks to characterize new isolates and assess efficacy of current vaccines. The decision to vaccinate in an outbreak is dependent on many factors, the most important of which are the age, vaccination status, and size of the population of horses at risk; the elapsed time since onset of the outbreak; the rapidity with which a diagnosis can be confirmed; the layout of the physical facilities; and availability of personnel. Outbreaks of influenza at racetracks and similar large facilities typically take 1 month or more to spread through the entire population. Therefore sufficient time exists to enhance immune protection of many at-risk horses while implementing other management strategies to minimize disease spread.93 It is prudent to booster- vaccinate those horses that have been on a regular influenza vaccination program but have not been revaccinated within the previous 3 months. It is also important to induce protection as quickly as possible in horses that have not previously been vaccinated. Of the vaccines currently available, Flu-Avert I.N. induces protection most rapidly, within 7 days of administration of a single IN dose. This is currently the product of choice for vaccination of naive horses and those of unknown vaccination status in the face of an outbreak.93 Adverse effects have not been reported when Flu-Avert I.N. is administered to horses that are incubating infection, although vaccination of horses that are already clinically ill is not recommended. Alternatively, an accelerated vaccination schedule using the canarypox- vectored vaccine with a primary intervaccination interval of 14 days and booster at 105 days has been shown to quickly confer long-lasting protective antibody levels.103 All 14 vaccinates demonstrated high SRH antibody titers 14 days following V2, thereby achieving 100% herd immunity to homologous viral challenge. Rapid induction of high levels of acquired herd immunity is critical in containing an outbreak of such a highly contagious pathogen as EIV103 In addition to reducing clinical and economic impacts, early vaccination clearly played an important role, together with biosecurity measures and movement restrictions, in containing the 2007 equine influenza outbreak in Australia, as well as ultimate eradication of the disease from that country.104 FUTURE INFLUENZA VACCINES. A recombinant modified vaccinia Ankara (rMVA) vector that delivers genetic material encoding for relevant hemagglutinin (H) antigens of an H3N8 influenza virus has been developed.105,106 The rMVA system is designed to focus the CTL response on the recombinant antigen and was initially tested in a prime-boost strategy in which the priming dose consisted of a DNA plasmid encoding for expression of the H antigen. The intent of this DNA prime-rMVA boost regimen was to invoke both cellular and humoral immune responses involved in protection.106 A subsequent study showed that the rMVA system was capable of inducing virus-specific lymphoproliferative and IFN-γ messenger ribonucleic acid (mRNA) responses; antigen-specific IgGa, IgGb, and IgA antibodies; and protection from challenge, both with and without a priming dose of the DNA vaccine.105 These data indicate that vaccination of horses with rMVA alone or as part of a prime-boost regimen is an effective means of inducing protective immunity to influenza virus infection.105 Considerable research has been performed to document the efficacy of the DNA vaccine used in the previously mentioned studies against equine influenza. However, the delivery system used (multiple sublingual, conjunctival, and subcutaneous [SC] injections delivered with a gene gun under general anesthesia) is impractical for use in the field.105,107 Recent licensing of a naked plasmid DNA vaccine that can be conveniently administered to horses by IM injection to prevent WNV infection clearly documents the potential for development of a DNA vaccine to prevent influenza in horses in the future. In addition, a DNA vaccine expressing the hemagglutinin protein of H3N8 influenza virus was recently shown to protect ponies against challenge when administered subdermally using a needle-free delivery system.108 Equine Herpesvirus (Rhinopneumonitis) The respiratory tract is the primary route of infection for EHV-1 and EHV-4, both of which cause respiratory tract disease that varies in severity from subclinical to severe and is characterized by fever, lethargy, anorexia, nasal discharge, and cough.109 Seroepidemiologic studies indicate that the vast majority of foals become infected with EHV-1 and EHV-4 during the first year of life, but the clinical disease syndromes resulting from these infections are not always well defined, perhaps reflecting the modulating effect of MDAs.110-112 Recurrent or recrudescent clinically apparent infections are seen in weanlings, yearlings, and young horses entering training, especially when horses from different sources are commin- gled.109,113 In contrast, surveillance studies involving racehorses document that seroconversion to both EHV-1 and EHV-4 occurs sporadically during the course of a racing season, but these seroconversions are often not clearly associated with outbreaks of respiratory disease that follow an epidemiologic pattern consistent with an infectious agent.114,115 EHV-1 and EHV-4 are spread by direct and indirect (fomite) contact with nasal secretions, by aerosolized secretions from infected horses, and in the case of EHV-1, by aborted fetuses, fetal fluids, and placentae associated with abortions. Management practices are therefore of primary importance for control of clinical disease caused by equine herpesviruses. Viremia occurs frequently after infection with EHV-1, potentially leading to paralytic neurologic disease (equine herpes myeloencephalopathy [EHM]) secondary to vasculitis of the spinal cord and brain, abortion of virus-infected fetuses, or birth of infected nonviable foals. In contrast, manifestations of infection with EHV-4 (rhinopneumonitis) are generally confined to the respiratory tract, because EHV-4 does not typically infect endothelial cells or produce a cell-associated viremia.116 As with herpesvirus infections in other species, horses typically fail to clear primary infections with either EHV-1 or EHV-4, the result being that most horses in the population remain latently infected with both viruses.109,112,117 Latently infected horses do not show clinical signs but may experience recrudescence of infection with or without clinical signs, an increase in antibody titer, and shedding of the virus when stressed. Consequently, many horses have detectable levels of SN antibody to both EHV-1 and EHV-4 in their serum.109,112,117 These features of the epidemiology of herpesvirus infections seriously compromise efforts to control these diseases and explain why outbreaks of EHV-1 or EHV-4 can occur in closed populations of horses. Whereas most mature horses have developed some immunity to EHV-1 and EHV-4 through repeated natural exposure and do not typically show respiratory signs when they become reinfected, horses do not appear to become resistant to the abortigenic or neurologic forms of infection with EHV-1 even after repeated exposure.118 In fact, previously exposed mature horses are more likely than juvenile horses to develop the neurologic form of the disease.119,120 The genetic basis underlying the apparent increased likelihood that some EHV-1 isolates will cause EHM appears to involve a single-point mutation in the DNA polymerase (DNApol) gene.121 This mutation results in the presence of either aspartic acid (D) or an asparagine (N) residue at position 752 of the DNA polymerase. More than 80% of EHV-1 isolates associated with EHM are of the D752 genotype, whereas less than 20% are of the N752 genotype.121 Isolates of the D752 genotype have been designated as “neuropathogenic strains” in recent publications, lay articles, and laboratory PCR result reports, whereas N752 isolates have been designated as “wildtype,” “abortigenic,” or “non-neuropathogenic” strains. The latter terminology is unfortunate because both the D752 and N752 isolates are capable of inducing all syndromes (i.e., respiratory disease, abortion, neonatal death, and EHM). Correlates for protection against EHV-1 and EHV-4 infection have been investigated extensively but are not yet fully defined. Infection with EHV-1 induces a strong humoral response, but protection from reinfection is short-lived and is not achieved until the horse has experienced multiple infections with homotypic virus.109,116 No clear relationship exists between protection from EHV-1 or EHV-4 infection and concentrations of circulating antibody induced by vaccination or infection, but clinical manifestations of disease and the duration and amount of virus shedding from the nasopharynx are reduced in animals with high levels of circulating neutralizing anti- body.116,122-126 Mucosal immunity and cell-mediated responses likely play a role at least as important as circulating neutralizing antibodies in protection against EHV-1 infection127 because the presence of MHC class 1-restricted CTL precursors in peripheral blood is correlated with protection.116 Because EHV-4 replication is largely confined to epithelial cells of the upper respiratory tract, mucosal immunity is likely important in protection.116 Currently available vaccines include inactivated vaccines containing only EHV-1 or both EHV-1 and EHV-4 and one MLV EHV-1 (Rhinomune [Boehringer Ingelheim]). Several inactivated products are licensed only for protection against respiratory disease; currently, all contain a low antigen load. Two inactivated products (Pneumabort-K + 1b [Zoetis] and Prodigy [Merck Animal Health]) that contain a high antigen load are licensed for protection against both abortion and respiratory disease. Performance of the killed low-antigen-load respiratory vaccines is variable, with some vaccines outperforming others. Performance of the killed high-antigen-load abortion/respiratory vaccines is superior, resulting in higher antibody responses and some evidence of cellular responses to vaccination. This factor may provide good reason to choose the high-antigen-load abortion/respiratory vaccines when the slightly higher cost is not a decision factor. Alternatively, the Calvenza EIV/EHV (Boehringer Ingelheim) respiratory vaccine induces high titers of VN antibody comparable with those induced by the high-antigen-load abortion/respiratory vaccines.8 The MLV EHV-1 vaccine (Rhinomune [Boehringer Ingelheim]) has been shown to induce a level of clinical protection and reduction in viral shedding of similar magnitude to that provided by an inactivated high-antigen-load vaccine (Pneumabort-K + 1b) and of greater magnitude than is provided by one of the killed low-antigen-load respiratory vaccines.128 Whereas vaccination with either EHV-1 or EHV-4 can provide partial protection against the heterologous strain, vaccines containing EHV-1 may be superior in this regard. The principal indication for use of equine herpesvirus vaccines is prevention of EHV-1-induced abortion in pregnant mares and reduction of signs and spread of respiratory tract disease (rhinopneumonitis) in foals, weanlings, yearlings, and young performance and show horses that are at high risk of exposure. Many horses do produce postvaccinal antibodies against EHV, but the presence of those antibodies does not ensure complete protection. Consistent vaccination appears to reduce the frequency and severity of herpesvirus-induced disease. Although convincing evidence is lacking, field experience suggests that whereas the incidence of sporadic EHV-1- induced abortion in individual mares has not changed, the incidence of abortion storms caused by EHV-1 has declined significantly since the introduction and widespread use of EHV-1 vaccines in the United States.117,118 Outbreaks of abortion and associated perinatal foal death, however, do continue to occur on occasion in herds of vaccinated mares. Of the vaccines currently licensed for use in pregnant mares in North America, only inactivated monovalent EHV-1 vaccines (Pneumabort-K + 1b [Parsippany-Troy Hills, NJ] and Prodigy [Merck Animal Health, Madison, NJ]) containing abortigenic strains of EHV-1 carry a label claim for preventing abortion, whereas at least one bivalent EHV-1/4 vaccine is licensed for prevention of abortion in Europe (Duvaxyn EHV-1/4 [Intervet]). One of the vaccines available in North America, Pneumabort-K + 1b, incorporates both the 1p and 1b subtypes of EHV-1 to reflect the documented increase in the proportion of EHV-1 abortions caused by the 1b subtype that occurred during the 1980s as compared with earlier years.129 Pregnant mares should be vaccinated during the fifth, seventh, and ninth months of gestation. Some veterinarians also recommend a dose during the third month of gestation. Similarly, vaccination of mares with an inactivated EHV-1/-4 vaccine at the time of breeding and again 4 to 6 weeks before foaling is commonly practiced to enhance concentrations of colostral immunoglobulin for transfer to the foal. However, no published reports document the effectiveness of this approach in raising titers of specific antibody in mares that have already been vaccinated against EHV-1 3 times during the previous 5 months. Vaccination of barren mares and stallions with either a bivalent EHV-1/-4 vaccine or a monovalent EHV-1 vaccine before the start of the breeding season and thereafter at 6-month intervals is recommended, with the goal of increasing herd immunity in an attempt to reduce viral shedding and challenge to pregnant mares on breeding farms.117 An MLV EHV-1 vaccine (Rhinomune) has been used as an aid in prevention of EHV-1 abortion by some practitioners for many years,130 even though this vaccine is not currently labeled for this use. Several recent developments have created renewed interest in the potential for use of MLV vaccines to protect horses against manifestations of EHV-1 and EHV-4 infection. Sequencing of the EHV-1 genome has made it possible to document the nature of the mutation encoding for attenuation, mediated through truncation of the gp2 glycoprotein of the KyA strain.131 Similar studies may soon yield information regarding the mutation underlying attenuation of the RAC-H strain from which Rhinomune was derived. Because currently available inactivated vaccines do not block infection with equine herpesviruses, the most we can hope for when using inactivated vaccines is reduction of severity of clinical signs and attenuation of virus shedding to help protect herdmates. Challenge studies in weanlings aged 5 to 8 months have clearly demonstrated the efficacy of an inactivated whole virus EHV-1/-4 vaccine in reducing clinical manifestations and virus shedding induced by virulent EHV-1 challenge administered 2 weeks after completion of the two-dose primary series.125 Efficacy was clearly correlated with vaccine-induced antibody levels at the time of challenge in this study.125 Specific antibodies against both EHV-1 and EHV-4 are passed in colostrum.22,25,132-134 Field studies with EHV-1 MLVs indicate that colostral antibodies exert a profound inhibitory effect on serologic responses to vaccination up to at least 5 months of age.21,135,136 However, a cytotoxic cellular immune response to both EHV-1 and EHV-4 was induced in a substantial percentage of foals vaccinated with an EHV-1 MLV in the presence of maternal antibody, even though humoral responses were often absent.137 It is uncertain whether these responses would provide protection against natural challenge. Recent studies with two different commercially available inactivated bivalent EHV-1/-4 vaccines and one inactivated EHV-4/EIV vaccine have shown that the majority of foals from EHV- vaccinated mares do not mount a detectable neutralizing antibody response to vaccines administered at 3 and 4 months of age, even when three doses are administered in the primary series.22,24,25 An increased proportion of foals responded when vaccinated with a three-dose series starting at 5 or 6 months of age, but a substantial number still failed to seroconvert.24,25 Some foals with low or undetectable levels of SN antibody at the time of vaccination failed to mount a serologic response, suggesting that low levels of antibody, below the lower limit of detection of the SN test based on EHV-1 antigen, are capable of inhibiting the serologic response to inactivated EHV-1/-4 vaccines.25 The failure of a large proportion of foals younger than 6 months of age to mount serologic responses to inactivated EHV-1/-4 vaccines and the influence of antibody titer at the time of vaccination on failure to respond has been confirmed using sensitive gD and gG ELISAs in studies on commercial stud farms in Australia.138 In parallel studies, these researchers concluded that mares were the source of infection for foals, and intensive use of inactivated EHV-1/-4 vaccines on breeding farms in Australia had a minimal impact on the infection rate of young foals and weanlings with EHV-1 and EHV-4.110,112,139 Considering the uncertainty regarding the role of EHV-1 and EHV-4 as causes of clinically important respiratory disease, the lack of published data regarding the efficacy of available vaccines in preventing infection and establishment of latency, and results of a recent study documenting the poor serologic responses of naive horses to a number of killed low-antigen- load EHV respiratory vaccines currently marketed in North America,8 there appears to be little rationale to support the common practice of frequent revaccination of foals, weanlings, yearlings, and young performance horses against EHV-1 and EHV-4.5 Furthermore, an obvious dilemma in designing a vaccination strategy to prevent EHV-1 and EHV-4 infection in foals and weanlings is that if primary immunization is delayed until 6 months of age or older to reduce the likelihood of MDA interference, foals are likely to encounter field infection before the three-dose primary series can be completed. It is therefore unreasonable to expect a high degree of efficacy for vaccination programs designed to protect foals and weanlings against EHV infection using available vaccines. Despite these uncertainties, many practitioners elect to vaccinate against both EHV-1 and EHV-4. Under these circumstances, a reasonable compromise would be to start foal vaccination at 4 to 6 months of age using two doses of an inactivated bivalent vaccine or an EHV-1 MLV administered 3 to 4 weeks apart, followed by administration of a third dose 2 to 5 months later. Revaccination at 4- to 6-month intervals, thereafter using either an inactivated bivalent EHV-1/-4 vaccine or a modified live EHV-1 vaccine, appears appropriate for yearlings and young performance or show horses that experience contact with other horses. Frequent vaccination of nonpregnant mature horses (except those on breeding farms) with EHV vaccines is generally not indicated. Available vaccines make no labeled claim to prevent EHM, and there is no evidence that current vaccines can prevent EHM in the field. Frequent revaccination of mature horses to help prevent EHM is not justified in most circumstances because EHM is a relatively rare disease from a population standpoint, and most mature horses have previously been infected with EHV-1 and are latent carriers. Currently available vaccines do not reliably block infection, development of viremia, or establishment of latency, and EHM has been observed in horses vaccinated against EHV-1 regularly at 3- to 5-month intervals with inactivated or modified live vaccines. ’ ’140’141 On the basis of the presumed similar pathogenic mechanism between EHV-1 abortion and neurologic disease,142,143 parallels likely exist in terms of the requirement for immunologic protection. The control of cell-associated viremia is thought to be critical for preventing EHV-1 abortion and, presumably, neurologic disease. Therefore the goal of any vaccination program aimed at the prevention of EHV-1 abortion or neurologic disease is to stimulate those immune responses that can reduce or eliminate cell-associated viremia. Two recent studies have investigated the protective effect of commercially available killed and MLV vaccines against experimental challenge with neurotropic EHV-1 strains 24 or 29 days after completion of 122123 a three-dose vaccination series.122,123 A significant reduction in the level of viremia was noted in ponies challenged after vaccination with either Calvenza or Pneumabort-K + 1b, both of which are inactivated vaccines.122,123 Reduction in viremia post challenge was not observed in ponies vaccinated with another inactivated vaccine (Prodigy) or the MLV vaccine (Rhinomune). A challenge study performed almost 30 years ago to test the efficacy of Pneumabort-K + 1b in preventing abortion and a recent study to test the efficacy of Rhinomune against challenge with a “neuropathogenic” strain of EHV-1 provided some evidence that these vaccines may have a place in control of outbreaks of EHM.126,128 Interestingly, the Army 183 EHV-1 strain used as the challenge virus in the Pneumabort-K + 1b efficacy study has now been shown to carry the D752 mutation, as has the Findlay 03 strain used in the Rhinomune study. However, the low numbers of horses used in these studies, the failure of either vaccine to prevent infection or significantly reduce the level of viremia, the lack of statistical significance of results pertaining to prevention of neurologic signs, and the well-known difficulties encountered in accomplishing a consistent and reproducible challenge model for neurologic EHV-1 infection justify caution in interpretation. The significant reduction in viral shedding observed in vaccinated horses provides reasonable justification for booster vaccination of nonexposed horses at risk for infection to reduce viral shedding in the event they do become exposed to EHV-1. By enhancing herd immunity, it is hoped that the level of infectious virus circulating in the at-risk population will be reduced, and in turn the risk that individual horses in the population will develop disease may be reduced.140 This approach also relies on the assumption that the immune system of most mature horses has already been “primed” by prior exposure to EHV-1 antigens through field infection or vaccination and can therefore be “boosted” within 7 to 10 days of administration of a single dose of vaccine. Although the validity of this approach has not been critically evaluated for prevention of EHV-1 neurologic disease, its implementation seems rational when faced with one or more horses with confirmed clinical EHV-1 infection (any form) at a particular facility. Whereas booster vaccination of horses likely to have already been exposed is not recommended, it is rational to booster vaccinate nonexposed horses, as well as those that must enter the premises, if they have not been vaccinated against EHV-1 during the previous 90 days. Use of the Rhinomune MLV or one of the inactivated EHV-1 vaccines known to stimulate high circulating titers of neutralizing antibody appears justified for this purpose. Horse owners must develop an understanding of the concept of boosting herd immunity to help protect the group of horses rather than focusing on the as yet unattainable expectation that the veterinarian can reliably protect an individual horse from developing potentially fatal EHM by administering one of the vaccines currently marketed as aids to prevention of clinical manifestations of EHV-1 infection. Ultimately, enforcement of strict biosecurity measures and hygiene practices are likely to be more effective than widespread vaccination in reducing the risk of acquiring infection. FUTURE VACCINATION STRATEGIES TO PREVENT HERPESVIRUS INFECTION. To be completely effective in blocking primary infection and establishing a lifelong carrier state with EHV-1 and EHV-4, future vaccination strategies should be directed at inducing a strong mucosal immune response in the upper respiratory tract during the first few weeks of life, at a time when high levels of maternal antibodies are present. Promising progress toward this goal was reported by Patel and colleagues,144 who documented that IN administration of a single dose of temperature-sensitive modified live EHV-1 vaccine to maternal antibody-positive foals aged 1.4 to 3.5 months afforded partial but significant protection against febrile respiratory disease, viremia, and virus shedding after IN challenge with virulent EHV-1 performed 8 weeks after vaccination. This vaccine has also been shown to provide significant protection against abortion in challenge studies, and because it is capable of preventing the development of viremia, it shows potential to prevent EHM.127,145 Recent studies with vaccinia and canarypox-vectored recombinant vaccines and DNA vaccines have generated promising results, but more research is necessary to identify the immunodominant protective antigens of EHV-1 and their interaction with the equine immune system before these approaches will be applicable for use in the field 146-150 The recent Third International Havemeyer Workshop on Equine Herpesvirus Type 1 highlighted the need to improve vaccines, with MLV being identified as the vaccine type most likely to be successful in inducing a protective immune response.151 The identified goals of future vaccine candidates will be to stimulate both humoral and cell-mediated immunity, differentiate infected from vaccinated animals (DIVA), provide minimal gaps in immunity, induce a rapid onset and long-lasting immunity, be effective in the presence of MDAs to prevent infection early in life, provide a wide clinical and virologic cross-protection, be safe and effective against the development of EHM, suppress reactivation of latent EHV-1 infection, and be safe when used in the face of an outbreak.151 Streptococcus equi subsp. equi Infection (Strangles) Strangles is a highly contagious disease caused by the bacterium Streptococcus equi subsp. equi (S. equi). Strangles primarily affects young horses (weanlings and yearlings), although horses of any age can become infected if not protected by previous exposure to the organism or vaccination. The organism is transmitted by direct contact with infected horses or subclinical carriers or indirect contact with water troughs, feed bunks, pastures, stalls, trailers, tack, or grooming equipment contaminated with nasal discharge or pus draining from lymph nodes of infected horses. The organism survives for several weeks in the environment, particularly in aquatic locations and when protected from exposure to sunlight and disinfectants, and can be a source of infection for new additions to the herd. Because S. equi is a clonal organism, there is minimal antigenic variation between different isolates even though isolates vary in their pathogenicity. Most horses develop a solid immunity during recovery from strangles, which persists in over 75% of animals for 5 years or longer,152 indicating that induction of durable protection through vaccination is biologically feasible if the protective antigens can be identified and presented in an appropriate manner.153 Although the basis for acquired resistance to strangles is not completely understood, the finding that recovered horses rapidly clear intranasally inoculated S. equi despite not making circulating antibody to its surface proteins indicates that to be highly effective a strangles vaccine must stimulate local nasopharyngeal tonsillar immune clearance responses and that serum antibody is of lesser importance.154 This conclusion is further supported by the finding that ponies with high levels of circulating antibody to multiple unique surface-exposed and secreted proteins after systemic vaccination remained susceptible to challenge with S. equi.154 The cell wall M protein of S. equi (SeM) is recognized in the acquired immune response to S. equi infection, a response that involves both production of local antibodies in the nasopharynx and circulating opsono- phagocytic antibodies.155-157 The predominant opsonophagocytic antibodies are of the IgGb subisotype but also include IgGa and IgA, whereas IgGb and later mucosal IgA predominate in nasopharyngeal secretions.156,158 Strangles vaccines licensed and marketed for use in North America include one inactivated adjuvanted M-protein cell wall extract (Strepvax II [Boehringer Ingelheim]) and one attenuated live vaccine (Pinnacle I.N. [Zoetis]) derived from a nonencapsulated mutant of S. equi for IN administration.159 Infection of horses with S. equi continues to cause troublesome outbreaks of strangles throughout North America, despite the availability and widespread use of these vaccines, indicating that their efficacy is suboptimal.160 M-protein vaccines induce a good opsonophagocytic antibody response in serum but a minimal mucosal IgA response, which likely accounts for the incomplete protection observed when they are used in the field.156,161 However, data do exist to document that vaccination using injectable SeM vaccines reduces the attack rate and severity of strangles in herds with endemic infection.161-163 The live IN vaccine has been shown to induce a relevant mucosal immune response and partial or complete protection but may do so without inducing a strong serologic response.160,164 Because vaccinal organisms in the IN vaccine must reach the inductive sites for immunity in the pharyngeal and lingual tonsils, accurate vaccine delivery is critical to vaccine efficacy. Vaccination against S. equi is not routinely recommended for pleasure or performance horses kept in low-risk situations, but it is a consideration for horses that are resident on or being transported to premises like breeding farms, where strangles is a persistent endemic problem or where a high risk of exposure is anticipated. The bacterial MLV is generally preferred over the inactivated injectable vaccine for primary vaccination of foals and weanlings and for routine use in older horses at high risk for infection. On breeding farms, efforts should be concentrated on preventing infection of foals and weanlings by booster-vaccinating broodmares 4 to 6 weeks before foaling to maximize colostral content of antibodies. Whereas the IN vaccine has been shown to be safe for use in mares at all stages of pregnancy and can be used in mares in the face of an outbreak, it does not reliably stimulate high levels of circulating antibody. For this reason, the intramuscularly administered inactivated SeM product is preferred for prefoaling booster immunization of mares. Antibodies of the IgG and IgA class recognizing the SeM are passively transferred to the foal through colostrum and are also present in the milk of immune mares.165 Antibodies of predominantly the IgGb isotype are absorbed from colostrum and redistribute to the nasopharyngeal mucosa.158 These IgGb antibodies, along with the SeM-specific IgA antibodies that are present in milk and passively coat the pharyngeal mucosa of nursing foals, provide protection to most nursing foals up to the time of weaning.157,158,165 Resistance of nursing foals to strangles during the first few months of life appears to be mediated by IgGb antibodies in nasal secretions and milk and not by IgA.165 Serologic (ELISA) responses to M-protein vaccines are poor in foals, most likely owing to the inhibitory effect of maternal antibodies. Whereas the IN MLV may be less susceptible than the inactivated extract vaccines to MDA interference, this issue has not been investigated and the manufacturer does not recommend administration of this vaccine to horses younger than 9 months of age. Considering that on farms where strangles is endemic, foals often become infected around the time of weaning (age 4 to 8 months), it is difficult to protect them if vaccination is delayed until age 9 months. A reasonable compromise on breeding farms where the risk of strangles infection is high and mares are on a regular vaccination program would be to begin primary vaccination of foals using the IN live vaccine as early as 4 months of age. The recommended two-dose primary series administered 2 to 3 weeks apart should be followed by a third dose 3 to 4 months later and boosters at 6- to 12-month intervals thereafter, depending on risk of infection. The IN vaccine has been administered to foals as young as 5 or 6 weeks of age during outbreaks. If a vaccine is used in this manner, a third dose of the vaccine should be administered 2 to 4 weeks before the foal is weaned to optimize protection during this high-risk period. Although there are few reports of adverse effects attributable to use of the IN strangles vaccine in young foals, the inability of foals to mount an adequate mucosal IgA response during the first month of life and the potential for interference by maternal antibodies suggests that foals are unlikely to fully benefit from IN strangles vaccine administered before 4 months of age. When an inactivated M-protein vaccine is used for primary vaccination of foals, it is recommended that the initial series begin at 4 to 6 months of age, using three doses administered at 4- to 6-week intervals, followed by semiannual boosters for as long as high- risk conditions prevail. Strangles vaccines should be administered only to healthy, nonfebrile horses free of nasal discharge and should not be administered to those that are known to have had recent direct exposure to clinically ill animals.153 However, outbreaks of strangles generally persist for several months to more than 1 year, particularly on breeding farms where each foal crop adds new susceptible animals to the population. Thus, strangles vaccines are frequently administered in the face of an outbreak as an adjunct to management practices designed to bring outbreaks under control, and it is not always possible to accurately determine the exposure status of each horse. Under these circumstances, the likelihood of preventing strangles is greatest for horses that have not yet been exposed and can be kept isolated from infected horses until 2 weeks after the vaccination protocol can be completed. Horses that have been vaccinated previously will generate a response more rapidly than naive horses. Similarly, the IN MLV is preferred over inactivated vaccines for immunization of naive horses in an outbreak because it is likely to generate a protective immune response more rapidly. Injectable strangles vaccines tend to cause local reactions at the site of injection more often than other equine vaccines. Injection in the gluteal muscles is not recommended because gravitational drainage along fascial planes can prove troublesome in the event an abscess develops at the injection site. In addition, purpura hemorrhagica, a serious and sometimes life-threatening systemic immune complex (Arthus-type) vasculitis manifested as edema with or without petechial hemorrhages on mucosal surfaces, has been observed with low frequency in the weeks after administration of strangles vaccines. Inactivated extract vaccines are implicated more often than the IN MLV, but all strangles vaccines have the potential to induce purpura hemorrhagica. The antigen present in immune complexes is SeM, along with antibodies of the IgA class. Because a high serum IgG titer against S. equi appears to be associated with an increased risk of developing purpura, routine testing for specific IgG antibodies using a commercially available ELISA test has been recommended as a means of preventing vaccine-associated purpura hemorrhagica.160 Horses with titers of 3200 or greater in the SeM ELISA and those known to have had strangles during the previous year should not be vaccinated.160 Recent studies investigated the factors associated with likelihood of horses having a high serum S. equi SeM- specific antibody titer.166,167 This study indicated that older horses, horses other than Thoroughbreds and warmbloods, and horses that had been vaccinated with an attenuated live IN S. equi vaccine between 1 and 3 years previously had an increased likelihood of having a serum SeM-specific antibody titer of 3200 or higher. Recommendations of when to vaccinate horses after an S. equi outbreak largely depend on how long horses maintain a serum SeM-specific antibody titer of 3200 or higher, which can range from 9 to 27 months. Therefore the recommendation is to wait at least 1 year after an outbreak before vaccinating horses against S. equi and to test for S. equi SeM-specific antibody titer 12 to 24 months following the outbreak.167 The bacterial modified live vaccine for IN administration will cause injection site abscesses if inadvertently injected intramuscularly. To avoid inadvertent contamination of other vaccines, syringes, and needles, it is advisable and considered good practice to administer all parenteral vaccines before handling and administering the IN strangles modified live vaccine. Other reported adverse responses after administration of the IN modified live vaccine include nasal discharge, submandibular or retropharyngeal lymphadenopathy with or without abscessation, limb edema, internal abscesses (bastard strangles), and purpura hemorrhagica. The overall frequency of adverse events is low but appears to be higher than reported to the manufacturer (4.8 per 10,000 doses). The majority of reported adverse events, including the development of nasal discharge, lymph node abscesses, and purpura hemorrhagica, occurs in horses on farms with endemic or epidemic strangles, so it is often uncertain whether the adverse event was caused by the vaccine or by a wild strain of S. equi. RECENT DEVELOPMENTS IN STRANGLES VACCINES. The nonspecifically attenuated Pinnacle strain of S. equi was produced by chemical mutagenesis to induce random mutations throughout the bacterial genome.157,168 Because the point mutations responsible for attenuation have not been specifically defined, the potential exists for back mutation and reversion to full virulence.168 In contrast, the live attenuated vaccine strain TW 928 contained in a strangles vaccine (Equilis StrepE [Intervet]) formerly licensed in Europe was stably attenuated by targeted deletion of the aroA gene.169 This allowed development of a companion PCR test that was used in molecular epidemiologic studies to determine whether strangles in vaccinated horses was caused by the vaccine or wild-type strains.170 Although this development proves that targeted gene deletion is a promising route for generating stable candidate mutants for inclusion in future vaccines, the high residual virulence, unconventional route of administration (submucosal in the upper lip), and short duration of immunity induced by Equilis StrepE limited its use to the extent that the vaccine was recently withdrawn from the market. The incomplete protection afforded by bacterins and SeM extracts administered parenterally or by attenuated live vaccines administered intranasally or submucosally, as well as the undesirable side effects associated with some of these products, has prompted research to investigate other potential vaccine antigens and vaccination strategies. Promising results have recently been achieved in challenge studies involving horses vaccinated intramuscularly and intranasally with combinations of up to seven recombinant antigens including EAG (a protein that binds α2-macroglobulin, albumin, and IgG), CNE (a collagen-binding protein), SclC (a collagen-like protein), and two IgG endopeptidases, IdeE and IdeE2.171,172 Equine Neorickettsiosis (formerly termed Potomac horse fever) Equine neorickettsiosis (EN), formerly known as Potomac horse fever (PHF), is caused by Neorickettsia risticii (formerly Ehrlichia risticii). Originally described in 1979 as a sporadic disease affecting horses residing in the northeastern United States near the Potomac River, the disease has since occurred in horses in 43 U.S. states, three Canadian provinces (Nova Scotia, Ontario, Alberta), South America (Uruguay, Brazil), Europe (The Netherlands, France), and India. The disease does not appear to be directly contagious, and it now appears that accidental ingestion of aquatic insects harboring metacercaria infected with N. risticii is at least one documented mode of transmission.173 EN is seasonal, occurring between late spring and early fall in temperate areas of the northern hemisphere, with most cases in July, August, and September at the onset of hot weather. The disease may sporadically affect individual horses or cause outbreaks involving multiple horses. Foals appear to be at low risk for the disease. If EN has been confirmed on a farm or in a particular geographic area, cases will likely occur in future years. Documentation of the involvement of operculate freshwater snails and aquatic insects like caddis flies and mayflies in the life cycle of N. risticii has permitted formulation of focused control measures directed at minimizing exposure of horses to the habitats occupied by these species during the summer and fall months, when disease risk is highest in endemic areas.173 Risk reduction is best accomplished by turning off barn lights at night, covering hay or storing it indoors, preventing horses from drinking at natural water sources like ponds or streams, and staying informed about local hatches of aquatic insects.174 Recovery after natural infection with N. risticii induces a strong antibody response and durable protection from reinfection lasting 20 months or longer. However, the presence of antibodies does not necessarily correlate with protection, and cell-mediated responses likely play a crucial role.175 A β-propiolactone inactivated host cell-free N. risticii vaccine protects mice against homologous challenge.176 Only one inactivated vaccine against N. risticii for IM administration (Equine Potomavac [Boehringer Ingelheim]) is licensed and available for use in horses as an aid in prevention of PHF. The high rate of serious complications and mortality associated with this disease has been considered adequate justification for vaccinating horses residing in or traveling to endemic areas. In a series of studies in which ponies were challenged intravenously with N. risticii approximately 4 weeks after completion of the two-dose primary vaccination series using a formalin-inactivated aluminum hydroxide-adjuvanted vaccine (PHF-Vax [Schering- Plough, Union, N.J.]) that is no longer marketed, Ristic's group (1988) reported that 78% of experimentally infected ponies were protected against all clinical manifestations of disease except fever and 33% were protected against all signs including fever.177 A published noncontrolled field study involving the same vaccine documented induction of serologic responses in most vaccinated horses and a substantial reduction in disease prevalence, morbidity, and mortality compared with data collected in a previous year when horses were not vaccinated.175,178 In contrast to the results of the studies cited, epidemiologic investigations involving a large number of horses failed to demonstrate any clinical benefit from annual vaccination with currently available vaccines in the states of New York, Indiana, and Kentucky.179,180 Failure of a substantial number of individual horses to mount an immune response to inactivated vaccines against N. risticii, heterogeneity of N. risticii isolates, the presence of only one N. risticii strain in vaccines, and much more rapid waning of immunity after vaccination than after natural infection likely account for the observed failure of vaccines to provide protection against field infection.175,181 Despite the lack of documented efficacy of approved vaccines to prevent infection in the field setting, many practitioners who work in endemic areas believe that severity of disease is attenuated and mortality is reduced in vaccinated horses when vaccines are administered at 4- to 6-month intervals, with administration of one booster timed to precede the anticipated period of peak challenge. If vaccination is elected, a primary series of two doses should be administered 3 to 4 weeks apart. The manufacturer recommends revaccination at 6- to 12-month intervals, but some veterinarians encourage a shorter revaccination interval. Because the disease has a distinct seasonal pattern, revaccination in the late spring, about 1 month before the first cases are expected, followed by a second dose 4 months later, appears to be a reasonable approach for strategic immunization to maximize the chances of protection during the period of peak challenge. The available vaccine is licensed for use in stallions and pregnant mares and can be administered to gestating mares 4 to 8 weeks before foaling to maximize passive transfer of specific antibodies to foals through colostrum. Whereas about 67% of foals from antibody-positive mares were antibody negative by 12 weeks of age, antibody was detectable in 33% of foals up to 5 months of age. On the basis of these findings, the low risk of clinical disease in young foals, and the apparent susceptibility to infection of two foals vaccinated earlier than 12 weeks of age, primary vaccination of foals from antibody-positive dams should begin with a two-dose primary series starting at age 5 months or older, followed by administration of one subsequent booster dose 8 to 12 weeks later.178 However, the efficacy of this recommended regimen requires further study. If the primary series of two vaccinations is initiated before age 5 months, additional doses should be administered at monthly intervals up to 5 months of age to maximize the likelihood that an immunologic response is achieved. Vaccination of foals in endemic areas is further complicated by the distinct seasonal incidence of disease in July, August, and September, a time when most foals are between 2 and 6 months old and may be subject to maternal antibody interference with vaccination. Botulism Botulism is a neuromuscular paralytic disorder caused by one of eight distinct neurotoxins (A, B, Ca, Cb, D, E, F, G) produced by Clostridium botulinum, a soilborne, spore-forming, saprophytic, anaerobic, gram-positive bacterium.182 Botulinum toxins are among the most potent biological toxins known and act by blocking transmission of impulses at motor end plates, resulting in weakness progressing to paralysis, inability to swallow, and frequently death. Of the seven serogroups (A through G) of C. botulinum, types A, B, C, and D have been reported to cause disease in horses, with types B and C responsible for most cases.182 Three forms of botulism— toxicoinfectious botulism (shaker foal syndrome), forage poisoning, and wound botulism—have been observed in horses. Forage poisoning results from ingestion of preformed toxin produced by decaying plant material or animal carcasses present in feed, whereas wound botulism results from vegetation of spores of C. botulinum and subsequent production of toxin in contaminated wounds. Shaker foal syndrome, almost all cases of which are caused by C. botulinum type B, results from toxin produced by vegetation of ingested spores in the intestinal tract. This syndrome is a significant problem in foals between the ages of 2 weeks and 8 months in Kentucky and the Mid-Atlantic seaboard states and occurs sporadically in other areas.183-185 Toxicoinfection with C. botulinum type C is currently being investigated as a cause of equine grass sickness, a largely fatal pasture-associated dysautonomia mainly affecting horses in Great Britain, continental Europe, and Australia, with reports of isolated U.S. cases. A toxoid vaccine (BotVax-B [Neogen Corporation, Tampa, Fla.]) directed against C. botulinum type B is licensed for use in horses in the United States. Its primary indication is prevention of shaker foal syndrome via colostral transfer of antibodies induced by vaccination of the mare. For primary vaccination, mares should be vaccinated during gestation with a series of three doses administered 4 weeks apart, scheduled so that the last dose will be administered 4 to 6 weeks before foaling to enhance concentrations of specific immunoglobulin in colostrum (i.e., months 8, 9, and 10 of gestation). Subsequently, mares should be revaccinated annually with a single dose 4 to 6 weeks before foaling. A similar type B toxoid is available to protect foals in endemic areas in Australia.186 Passively derived colostral antibodies appear to protect most foals for 8 to 12 weeks, although foals from properly vaccinated dams can present with botulism.184-186 Insufficient production of specific antibody by the dam in response to the vaccination, failure of passive transfer of specific immunity to botulinum toxin, overwhelming toxin production, and loss of passive immunity by the time exposure to the toxin occurs may be reasons for vaccine failure. The clinician should be aware of the status of MDA transfer of each foal. Maternal antibodies do not appear to interfere with the response of foals to primary immunization against botulism,187 so a primary series of three doses of vaccine administered 4 weeks apart can be started when foals in endemic areas are 2 to 3 months of age or older. Other horses can be immunized using a primary series of three doses of vaccine administered at 4-week intervals, followed by annual revaccination. No licensed vaccines are available at present for preventing botulism due to C. botulinum type C or other subtypes, and because cross-protection between the B and C subtypes does not occur, routine vaccination against C. botulinum type C is not currently practiced. A type C toxoid approved for use in mink was administered to horses under special license to protect them during an outbreak of forage poisoning caused by contaminated alfalfa cubes in southern California in 1989. The C-terminal part of the heavy chains of botulinum neurotoxin types C and D (HcBoNT/C and D) has been expressed in Escherichia coli and has been shown to effectively immunize horses when administered as a recombinant monovalent or bivalent vaccine.188,189 These vaccines are not yet licensed. Horses and foals with clinical botulism may be treated with botulinum antitoxin administered intravenously. Antitoxin is not effective against toxin that has been translocated to motor end plates, so clinical signs may progress for 12 to 24 hours after administration of the antitoxin or until all internalized toxin has attached to motor end plates. The dose of botulinum type B antitoxin recommended for treating a foal is 30,000 IU and for an adult is 70,000 IU. Foals of unvaccinated mares born in or being moved to endemic areas may benefit from transfusion with plasma from a vaccinated horse or from administration of C. botulinum type B antitoxin. The efficacy of these practices warrants further study. Vaccination with type B toxoid as described earlier is an alternative to passive immunization. Equine Viral Arteritis Equine viral arteritis (EVA) is a contagious disease of equids caused by equine arteritis virus (EAV), an RNA virus found in the horse populations of many countries. EAV is the prototype virus in the family Arteriviridae of the genus Arterivirus, order Nidovirales. Although all horse breeds appear to be equally susceptible to EAV, the prevalence of infection, as determined by seroconversion, is much higher in some breeds (notably Standardbreds and warmbloods) than in others. Despite the high seroprevalence of infection in Standardbreds, clinical disease is rarely observed in this breed, indicating that subclinical infection is common.11,190 Conversely, Thoroughbreds and most other breeds have a low seroprevalence of infection but are more likely to show fulminant clinical signs when they become infected. Most primary EAV infections are subclinical or asymptomatic. Clinical signs, if they occur, typically develop 3 to 7 days post infection and vary in severity, both within and between outbreaks, but may include some or all of the following: fever, anorexia, depression, localized or generalized urticaria, supraorbital or periorbital edema, conjunctivitis, lacrimation, serous or mucoid nasal discharge, and dependent edema involving the limbs, prepuce, scrotum, mammary glands, or ventrum. EVA is of special concern because abortion is a frequent sequel to infection in the unprotected pregnant mare. EAV can also cause life-threatening pneumonia or pneumoenteritis in young foals, and infection of the postpubertal colt or stallion may establish a long-term carrier state.11,191 Transmission most frequently occurs through direct or aerosol contact with virus-infective respiratory secretions, leading to widespread dissemination of the virus among susceptible horses in close proximity. Indirect transmission, though less significant, can occur through contact with virus-contaminated fomites. Venereal transmission from infected carrier stallions to mares via semen during natural breeding or artificial insemination with fresh, chilled, or frozen semen can play a significant role in introduction and spread of infection on or between breeding farms or other equine facilities. The virus can persist in the reproductive tract of stallions for many years and possibly result in lifelong infection. Historically, large-scale outbreaks of EVA have been relatively infrequent. However, the number of confirmed occurrences appears to be increasing, likely because of increased global movement of horses, increased accessibility of carrier stallions, and increased utilization of shipped cooled or frozen virus-infected semen. Outbreaks can be associated with serious economic consequences, as clearly exemplified by the 2006 multistate outbreak in Quarter Horses that was propagated by widespread shipment of semen from the index cases, two inapparently infected carrier stallions in New Mexico. Because the carrier stallion is widely accepted as the natural reservoir of EAV and the source of diversity among naturally occurring strains of the virus, identifying these individuals through serologic testing followed by PCR testing or virus isolation from semen forms the cornerstone of eradication measures. Vaccination also constitutes an important means of controlling spread and minimizing the consequences of infection. A modified live vaccine based on an attenuated strain of EVA virus was developed by researchers in Kentucky in 1969.192 This vaccine (Arvac [Zoetis]) was first used extensively in the field during the 1984 outbreak of EVA in Kentucky and proved safe and effective in bringing the outbreak under control.11 This vaccine was developed further and licensed for use in North America. Vaccination of stallions, nonpregnant mares, and prepubertal colts has been shown to be a safe and effective means of controlling EVA. Strategic use of the MLV has formed the cornerstone of a highly successful program to control EVA in the Kentucky Thoroughbred breeding population for many years.11 Indications for vaccination against EVA are to: • Protect stallions against infection and subsequent development of the carrier state • Immunize seronegative mares before being bred with EAV- infective semen • Curtail outbreaks in nonbreeding populations. Vaccination in the face of an EVA outbreak in concentrated populations of performance horses at racetracks has been successful in controlling horizontal disease dissemination within 7 to 10 days. Primary immunization with the modified live vaccine involves IM administration of a single dose, with a booster administered annually thereafter. Virus-neutralizing antibodies are induced within 5 to 8 days after vaccination and persist for at least 2 years.11,193 Revaccination induces high VN antibody titers that persist for several breeding seasons.194 Although the current modified live vaccine is highly attenuated and has been shown to be safe and effective in stallions and nonpregnant mares, a small proportion of first-time vaccinated horses develop mild febrile reactions and transient lymphopenia after vaccination, and vaccine virus may be isolated sporadically from the nasopharynx and buffy coat for 7 days (occasionally up to 32 days) after vaccination.11,193,195,196 Vaccinated stallions do not 194 shed vaccine virus in either semen or urine.194 Primary vaccination provides sustained clinical protection against EVA but does not prevent reinfection and subsequent limited replication and shedding of field strains of virus.197 However, the frequency, duration, and amount of viral shedding via the respiratory tract are significantly reduced in vaccinates. Vaccinated mares may transiently shed field virus after being bred to carrier stallions, so isolation of these individuals for 21 days after breeding is recommended.11 Annual revaccination of breeding stallions 28 days before the start of breeding season is highly recommended as a means of preventing establishment of the carrier state.11 Annual revaccination of mares being bred to carrier stallions should occur at least 21 days before breeding. The modified live vaccine is not recommended for use in pregnant mares, especially during the last 2 months of gestation, or in foals younger than 6 weeks of age, except in emergency situations when there is a high risk of exposure. Apparent fetal infection with the modified live vaccine strain after vaccination of pregnant mares has been documented in rare instances.193,198 A recently published study in which 73 pregnant mares were vaccinated during midgestation to late gestation concluded that it is safe to vaccinate healthy pregnant mares up to 3 months before foaling and during the immediate postpartum period. Vaccinating mares during the last 2 months of gestation was associated with an increased risk of abortion.199 The authors concluded that when faced with a substantial risk of natural exposure to EAV, the risk associated with vaccination must be weighed against the much greater risk of widespread abortions in 199 unprotected populations of pregnant mares.199 Foals born to seropositive mares become seropositive after ingesting colostrum. MDAs decay with a mean half-life of approximately 32 days, with the result that foals become seronegative between 2 and 7 months of age.200,201 Maternal antibodies are unlikely to interfere with the response to vaccine administered at 7 months of age or older.200 However, when foals younger than 6 months are vaccinated during conditions of high risk, they should be revaccinated after age 6 months. Establishment of the carrier state appears to depend on the high levels of androgens circulating in intact stallions and can be prevented by vaccinating colts, preferably before puberty and before they are used for breeding.11 Vaccination of prepubertal colts at age 6 to 12 months is therefore central to effective control of the spread of EAV infection and should be strongly encouraged in breeds like Standardbreds and warmbloods in which EVA is prevalent and on facilities where risk of infection is high. Persistent infection has never been documented in a stallion properly vaccinated with the licensed modified live vaccine before exposure.11 REGULATORY AND EXPORTATION CONSIDERATIONS WITH VACCINATION AGAINST EVA. Horses vaccinated with the MLV can be expected to become seropositive for life. Titers resulting from vaccination cannot be distinguished from titers resulting from natural infection, so vaccination may complicate testing of horses for export. When planning a vaccination program against EVA, it is important to consult with state and/or federal animal health officials to ensure that any such program is in compliance with the state's control program for EVA if one exists. It is strongly recommended that before vaccination, all first-time male vaccinates be tested and confirmed negative for antibodies to EAV by a USDA-approved laboratory (http:// www.aphis.usda.gov/cvbapps/Labs.jsp). Mares intended for export should be similarly tested. In instances where there is uncertainty or concern over whether vaccination against EVA could prevent export of a horse to a particular country, it is advisable to consult the federal area veterinarian (http:// www.aphis.usda.gov/vs/area_offices.htm#CO) in charge in the state to determine the specific import requirements of that country. Several countries bar entry of any equid that is serologically positive for antibodies to EAV, regardless of vaccination history. Countries that do accept EVA vaccinated horses typically require stallions or colts to have a certified vaccination history and confirmation of prevaccination negative serologic status. FUTURE DIRECTIONS. Development and marketing of a marker vaccine that not only affords protection but also allows vaccinated horses to be distinguished serologically from inap- parently infected carriers would greatly facilitate control and even eradication of EAV from horse populations. Several new-generation EAV vaccines that potentially meet these criteria have been developed in recent years. These include an MLV DIVA vaccine with a deletion in the GP5 ectodomain,202,203 a DNA vaccine that incorporates open reading frames (ORFs) 2b, 5, and 7,204,205 and a subunit EAV vaccine using recombinant replicon particles derived from a vaccine strain of VEE virus that includes genes encoding both major envelope proteins (GP5 and M) of EAV206,207 Rotaviral Diarrhea Equine rotavirus (ER), a nonenveloped icosahedral RNA virus possessing a genome comprising 11 segments of dsRNA, is one of the most important causes of infectious diarrhea in foals during the first few weeks of life and often causes outbreaks involving the majority of the foal crop on individual farms.208-210 Older foals and adult horses are more resistant to infection. Equine RV is transmitted via fecal-oral contamination and causes diarrhea by damaging the tips of villi in the small intestine, resulting in cellular destruction, maldigestion, malabsorption, and diarrhea. The genus Rotavirus is one of five genera of the family Reoviridae and is divided into seven serogroups (A through G) based on differences in the inner capsid protein, VP6.210,211 All equine rotavirus isolates to date are in group A, which is further subdivided using neutralizing antibodies to the VP4 and VP7 outer capsid proteins into P (protease-sensitive, VP4-positive) and G (glycoprotein, VP7positive) serotypes, respectively.211 Five P serotypes (P1, P6, P7, P12, and P18) and eight G serotypes (G1, G3, G5, G8, G10, G13, G14, G16) have been identified and characterized in horses.212-214 Molecular genome analysis strongly suggests that the vast majority of the currently circulating equine group A rotavirus strains are highly conserved, with only limited genetic diversity.215 Most are of the P12 and G3 serotype and include two subtypes (A and B).216 An inactivated rotavirus A vaccine (Equine Rotavirus Vaccine [Zoetis]) containing the P12, G3 serotype (H2 strain) in a metabolizable oil-in-water emulsion is conditionally licensed in the United States and is indicated for administration to pregnant mares in endemic areas as an aid for preventing diarrhea in their foals caused by infection with ERs of serogroup A. Foal vaccination is not indicated; no data suggest that vaccinating the newborn foal with inactivated rotavirus A vaccine has any benefit in preventing or reducing infection severity. Label recommendations call for a three-dose vaccine series to be administered to mares during each pregnancy at 8, 9, and 10 months' gestation. This protocol has been shown to induce significant increases in serum concentrations of neutralizing antibody in vaccinated mares and in antibody concentrations of the IgG (but not IgA) subclass in colostrum and milk of vaccinated mares.217,218 It is essential that the newborn foal receive an adequate amount of good-quality colostrum so that it absorbs sufficient anti-ER antibodies. After nursing from vaccinated mares, the concentration of passively derived ER- specific antibody of the IgG subclass in the serum of foals up to 90 days of age is significantly higher than that measured in serum of foals born to unvaccinated mares.217,218 A field study showed this vaccine to be safe when administered to pregnant mares and provided circumstantial evidence of at least partial efficacy. An approximately twofold higher incidence of rotaviral diarrhea was found in foals from unvaccinated mares compared with those from vaccinated mares, although this difference did not prove to be statistically significant.217 Similarly, a controlled field study in Argentina in which an inactivated aluminum hydroxide-adjuvanted vaccine containing the SA11 (G3P2), H2 (G3P12), and Lincoln (G6P1) strains of equine rotavirus was administered to 100 mares at 60 days before foaling and again 30 days later demonstrated a substantial reduction in the incidence and severity of rotaviral disease in foals from vaccinated mares compared with foals from unvaccinated mares.219 As MDA titers wane at about 60 days of age, foals may develop rotaviral diarrhea, but the severity of diarrhea is generally milder and of shorter duration than in foals that become infected during the first 30 days of life. Challenge studies involving two inactivated rotavirus vaccines administered in a similar manner to pregnant mares in Japan showed that their foals were not completely protected against infection but had a substantial reduction in severity of clinical signs after challenge.214 The major correlate for protection against rotaviral infection appears to be mucosal immunity, predominantly mucosal IgA, in the gastrointestinal tract. Studies of the immunoglobulin isotype responses of mares after parenteral vaccination with inactivated ER vaccines, and of antibodies passively transferred to their foals via colostrum, indicate that this approach is unlikely to provide foals with intestinal mucosal protection in the form of IgA.218 Consequently, it is not surprising that current protocols do not provide complete protection. In addition, because the conditionally licensed vaccine available in the United States contains only the G3 serotype of the A serogroup, it cannot be expected to protect against infection with all field strains. Equine Rhinitis A Virus Two rhinitis viruses, equine rhinitis A virus (ERAV; formerly known as equine rhinovirus 1, genus Aphthovirus, family Picornaviridae) and equine rhinitis B virus (ERBV; formerly known as equine rhinovirus 2, genus Erbovirus, family Picor- naviridae), have been identified in horses.220-225 Seroprevalence studies confirm that both viruses are active in horse populations worldwide, with prevalence ranging from 20% to 90%, depending on the age group and use of the horses sampled.221,222,226 The rhinitis viruses have been largely overlooked as potential causes of clinically apparent respiratory disease for many years, but recently investigated outbreaks of contagious respiratory disease, as well as challenge studies, suggest that ERAV and ERBV may indeed be important pathogens of horses, causing both lower and upper respiratory tract disease.223,225,226 Clinical manifestations include pyrexia, nasal discharge, cough, lethargy, anorexia, pharyngitis, and submandibular lymphadenopathy.223,225 It has also been suggested that ERAV may play a causative role in inflammatory airway disease.226 A unique feature of ERAV is persistent shedding in urine but only short shedding in nasal secretions after respiratory tract infection.220 An inactivated ERAV vaccine (Equine Rhinitis A Vaccine [Boehringer Ingelheim]) was granted a conditional license in late 2012; efficacy and potency tests are in progress. The vaccine is labeled for vaccination of healthy horses 4 months of age or older. The manufacturer recommends a primary vaccination series of three 1-mL doses administered IM at 3- to 4-week intervals, followed by revaccination annually or before anticipated exposure. Pending publication of more data regarding vaccine efficacy, as well as the role of ERAV as a cause of respiratory disease, these authors are unable to provide recommendations regarding use of this vaccine at the present time. Anthrax Anthrax is a serious and rapidly fatal septicemic disease caused by proliferation and spread of the vegetative form of Bacillus anthracis in the body. B. anthracis is acquired through ingestion, inhalation, or skin penetration through contamination of wounds by soilborne spores of the organism. Anthrax is encountered only in limited geographic areas where moist alkaline soils, particularly those with high organic content, favor survival, germination, and sporulation of the organism. Vaccination is indicated only for horses pastured in endemic areas. The only vaccine currently licensed for vaccination of livestock, including horses, contains viable live Sterne's strain 34F2 nonencapsulated spores in saponin (Anthrax Spore Vaccine [Colorado Serum Company, Denver, Colo.]). A primary series consisting of two doses of that vaccine should be administered SC 2 to 3 weeks apart, followed by annual revaccination. Mild to moderate swelling at the injection site is common, and adverse systemic reactions may occur occasionally, particularly in young and miniature horses. Little objective information is available regarding use of this vaccine in horses, but clinical evidence suggests that it provides protection. Vaccination of pregnant mares is not recommended.227 Because it is a live bacterial product, appropriate caution should be used during storage, handling, and administration of the vaccine to prevent accidental inoculation of people and maintain vaccine potency. Concurrent administration of antimicrobial drugs effective against B. anthracis is contraindicated if the vaccine is to function as intended. Leptospirosis Leptospirosis is a bacterial disease with a worldwide distribution caused by spirochetes of the genus Leptospira. Classification of Leptospira spp. is fairly complex and is performed either via the traditional phenotypic classification based on serotyping or via genotypic classification based on DNA homology.228 In North America the most prominent pathologic serovar associated with disease of equids is Leptospira interrogans serovar Pomona type kennewicki.229 Opossums, raccoons, skunks, foxes, and deer are believed to be the most common maintenance host of this serovar. In horses Leptospira infection has most often been associated with abortion, equine recurrent uveitis, and renal and hepatic disease.230 Horses are typically exposed to Leptospira by ingestion of wet vegetation or water that has been contaminated by urine of a carrier or reservoir host, after which Leptospira spirochetes penetrate mucous membranes or breaches of skin, although other routes of exposure include contact with aborted fetuses, placentas, uterine discharge, or milk or with water contaminated by any of these materials.230 A diagnosis of leptospirosis in horses can be challenging due to the difficulty in identifying Leptospira spp. and the high seroprevalence in the equine population.231A combination of serology, culture, direct detection, and qPCR testing is used to support a diagnosis of leptospirosis. A single leptospirosis vaccine (LEPTO EQ INNOVATOR [Zoetis]) is licensed for horses in the United States. The vaccine contains a whole-cell monovalent Leptospira bacterin with a label claim to use as an aid in prevention of leptospiremia caused by Leptospira interrogans serovar Pomona in healthy animals 6 months of age or older, as well as in pregnant mares in all three trimesters of gestation. The manufacturer recommends a primary vaccination series of two 1-mL doses administered IM at 3- to 4-week intervals, followed by revaccination annually. Corynebacterium pseudotuberculosis Infection (Pigeon fever) C. pseudotuberculosis, an agent of pigeon fever or dryland distemper, is a gram-positive, intracellular, facultative anaerobic bacterium. Flies act as a mechanical vector for this microorganism, and transmission occurs generally through abrasions or wounds in the skin or mucous membranes.232 Pigeon fever has a seasonal incidence with the highest number of cases occurring during the dry months of the year, which is late summer and fall in the southwestern United States.233 In recent years, pigeon fever cases have been diagnosed with increased frequency outside the western states. There are three forms of the disease, which are external infection, internal infection, and ulcerative lymphangitis. A diagnosis of pigeon fever infection is based on clinical signs, clinicopathologic data, diagnostic imaging, bacterial culture of an aspirate, and serology.234 A conditionally licensed inactivated C. pseudotuberculosis bacterin-toxoid (C. pseudotuberculosis bacterin- toxoid [Boehringer Ingelheim]) is available in the United States. The vaccine is labeled to be used in horses 12 months of age or older for the immunization against disease caused by C. pseudotuberculosis. The manufacturer recommends a primary vaccination series of two 1-mL doses administered IM at 3- to 4-week intervals, followed by revaccination annually. Pending publication of more data regarding vaccine efficacy, these authors are unable to provide recommendations regarding use of this vaccine at the present time.
More on the topic REFERENCES:
-
Veterinarian -
|