Septic Arthritis and Osteomyelitis
Rachael L. Smith
Neonatal foals are particularly susceptible to septic arthritis, osteitis, and osteomyelitis.160 The incidence of this form of sepsis was estimated at 1% of all foals in the 1970s161 but has likely reduced in recent decades as a result of improved management practices.
This manifestation of sepsis represents significant loss to the industry, with reported survival rates to discharge from veterinary facilities between 42% and 81%, but with only 30% of those with septic arthritis and 48% of those with septic osteomyelitis achieving long-term athletic soundness.162-166 Prognosis is influenced by the number of joints affected, number of bones involved, age of the foal, and presence of other medical problems.101,162,167A classification scheme for septic arthritis and osteomyelitis has been developed on the basis of radiologic and pathologic findings.168 The “S-type” describes bacterial infection of the synovial membrane of one or more joints with no radiographic changes, but there is joint effusion and possible periarticular soft tissue swelling. This form is typically seen in the first 2 weeks of life, and the most commonly affected joints include the carpus, stifle, and hock. The “E-type,” or epiphyseal, classification describes infection of the joint and osteomyelitis of adjacent subchondral bone. It is usually seen at 3 to 4 weeks of age, and common sites are femoral condyles, distal radius, distal tibia, or patella. “P-type,” or physeal-type, classification is used for cases of osteomyelitis of the physis on the metaphyseal side of the growth plate. This form occurs in foals 1 to 12 weeks of age and occurs most commonly in the distal radius or tibia, as well as the distal metacarpi/tarsi. The “T-type,” or tarsal, classification describes osteomyelitis of the cuboidal bones of the tarsus or carpus.
Etiology and Pathophysiology
Joint and bone infections of neonates most commonly result from persistent or transient hematogenous dissemination of bacteria from distant sites of infection.168,169 Gastrointestinal, respiratory and umbilical infection, and failure of passive transfer are common predisposing causes. Less commonly, infection can occur after direct trauma or penetrating wounds and extension of an infection from adjacent infected soft tissues. Common bacterial isolates include Enterobacteriaceae (Escherichia coli), Salmonella, Actinobacillus equuli, Klebsiella spp., Streptococcus, and Rhodococcus equi.170 Bacterial colonization of joints resulting from bacteremia is facilitated by the vascular pattern of neonates. Rapidly growing bones and joints require increased blood flow, derived from a main arteriole providing blood supply to the synovial membrane and epiphysis, and the nutrient artery supplying the metaphysis. In neonatal foals, transphyseal vessels connect epiphyseal and metaphyseal blood supplies. Bacterial deposition in the synovium and subchondral bone occur as epiphyseal vessels branch toward the articular surface and form hairpin bends ending in wide venous sinusoids—regions of lower blood flow, oxygen tension, and pressure. The synovial membrane lacks a basement membrane; therefore bacteria that are deposited in the subsynovial capillaries are able to readily migrate into the joint. Physeal infection is more likely to occur after closure of the transphyseal vessels, around 7 to 10 days of age, because of localization of the infection in metaphyseal vessel loops.168,171 Colonization of bacteria in the articular, metaphyseal, and synovial vessels can lead to thrombosis and subsequent ischemic necrosis.172 This can initiate a severe inflammatory response in associated tissues, producing classical clinical signs of joint effusion, heat, lameness, and pain on palpation of the periarticular tissues.
Normal synovial fluid production and drainage is also impaired, leading to compromised articular cartilage metabolism. An influx of degradatory inflammatory mediators, white blood cells, serum proteins, and proteolytic enzymes leads to further disruption of chondrocyte metabolism and degradation of the cartilage.The magnitude of the inflammatory response is determined by the virulence of the causative organisms, the size of the inoculum, and host resistance. The described sequelae resulting from infection highlight the importance of early diagnosis and treatment to achieve successful resolution before permanent degradative changes occur in the joint and periarticular tissue.
Diagnosis
Any lameness, joint effusion, or periarticular swelling in a neonatal foal should be considered significant and investigated regardless of history. Often, reporting is delayed as owners commonly suspect mare-induced trauma to the foal, or they may describe the foal as moving “stiffly” or “slowly” rather than being overtly lame. Large joints such as the stifle, hock, carpus, and fetlocks are more commonly affected.163,166,172,173 Pain in the foot or swelling of the coronary band could also be due to septic arthritis or osteitis/osteomyelitis.82,134 Other causes of lameness and swelling associated with joints include cellulitis, hemarthrosis, fracture, trauma, and subsolar/solar bruising of the foot (Box 17.1).
The most consistent and early clinical sign of joint sepsis is effusion. Periarticular swelling, heat, pain on palpation of the bone or joint, and restricted passive movement of the joint
■ BOX 17.1
Lameness in Foals
Septic arthritis/osteitis/osteomyelitis
Fracture
Common sites: PIII, physιs of P1, proxιmal sesamoid bones, olecranon
Hemarthrosis
Cellulitis
Flexural deformity
Rupture of the common digital extensor tendons Rupture of the gastrocnemius muscle Subsolar/solar bruising of the foot
Laminitis
Peripheral nerve injury
are commonly reported.
Less consistent clinical signs include lameness, an elevated rectal temperature, and hematologic changes consistent with infection. Lameness may escape identification if foals are systemically ill, weak, or recumbent. Lameness can take 8 to 24 hours to develop after bacteria have colonized the joints.174 If there is swelling detected in one joint, thorough palpation of all other joints is recommended. Regardless of history and complete diagnostic findings, it is prudent to treat any joint swelling or lameness in a neonatal foal as septic until proven otherwise.Hematologic changes can be inconsistent early in the disease course, but typically by 72 hours post inoculation there is leukocytosis and hyperfibrinogenemia. These findings lack both sensitivity and specificity. Fibrinogen levels greater than 900 mg/dL (>9 g/L) can be a useful indicator for epiphyseal or physeal osteomyelitis, but again this is neither sensitive nor specific.175 Ultrasonography can be useful in detecting bone irregularities; defining and classifying joint effusion; as well as detecting associated problems such as pneumonia, omphalitis, or omphalophlebitis.
In order to reach a definitive diagnosis of septic orthopedic disease, additional diagnostic tests are required. These include diagnostic imaging and synovial fluid analysis following arthrocentesis, including cytology, Gram stain, and bacterial culture. To facilitate these procedures, adequate restraint of the foal is required. For neonatal foals, diazepam (0.1 mg/kg body weight IV) provides around 10 to 15 minutes of sedation to perform minimally invasive procedures. Before synoviocen- tesis, the skin should be clipped and aseptically prepared at the site of needle placement. Chlorhexidine or povidone-iodine scrubs are commonly used with isopropyl alcohol. Practitioners should not be overly vigorous in preparation of the skin and should avoid use of abrasive swabs as the skin of foals is particularly susceptible to trauma.
It is likely that repeated scrubbing will be needed during the course of treatment, so preservation of the epithelial integrity is important. Lavage of the prepared area following the procedure with saline, drying the skin, and application of a topical antibiotic or antiseptic emollient cream is recommended before covering the site. Intraarticular administration of antibiotic into the joint following synoviocentesis is recommended, even if sepsis is not yet confirmed on cytology.Any region of fluid distention of the joint, identified by bulging or balloting of the joint capsule, is appropriate for sampling, provided there is awareness of local anatomy. Ultrasonography is recommended to identify pockets of synovial fluid. In joints such as the stifle, carpus, and hock where multiple joint compartments are in close proximity, the potential for communication should always be considered. For this reason, arthrocentesis from each compartment should be performed and the synovial fluid from each analyzed to determine the exact joint involvement. A 20- to 21-gauge needle can be used to aseptically collect synovial fluid. Fluid should be collected for cytologic examination into an EDTA tube and a sterile serum tube for culture. Alternatively, synovial fluid can be injected into a blood culture medium to increase the chance of a positive culture. Confirmation of synovial sepsis from synovial fluid evaluation and testing is not always straightforward.176
Normal synovial fluid is of a light yellow to straw color, is transparent (should be able to see newspaper print through the tube and fluid), and has good viscosity. Signs consistent with sepsis include increased turbidity, darkening in color (dark yellow to orange), and reduced viscosity. In severe cases, flocculent debris may be identified. The total protein (TP) of normal joint fluid is typically less than 20 g/L. Septic fluid usually has a TP greater than 40 g/L, but values greater than 20 g/L should be regarded as suspicious if other findings are supportive of synovial sepsis.
The total nucleated cell count (TNCC) and differential nucleated cell count are considered the most useful evaluation of synovial fluid when diagnosing sepsis. Typically cell counts that are considered diagnostic of septic arthritis are greater than 30 ? 109 cells/L, but infection should be suspected with values between 10 ? 109 cells/L and 30 ? 109 cells/L, particularly if the percentage of neutrophils is high.171,176 Sequestration of WBCs into fibrin clots within the joint can result in lower-than-expected cell counts. Normal synovial fluid has less than 10% neutrophils. A cytologic differential greater than 80% neutrophils is highly suggestive of sepsis.177 Synovial fluid lactate, glucose, and pH have been evaluated to improve the accuracy of diagnosis, and it appears synovial lactate may be useful; however, reference ranges are yet to be established.162Sympathetic synovitis results from increased blood flow to a region, most commonly due to adjacent infected bone. The TNCC and TP of synovial fluid in sympathetic effusions are often elevated, but the percentage of neutrophils remains less than 80%.168 Despite a low sensitivity for identification of bacteria, a Gram stain of synovial fluid should be performed. If bacteria are present, the results can guide antimicrobial selection while culture results are pending. Given the difficulty in culturing bacteria from joint fluid, a Gram stain result can sometimes be the only available option.172 Synovial fluid should be submitted for aerobic and anaerobic culture. Positive cultures are obtained in 55% to 85.7% of synovial fluid samples submitted.162,165,178,179 This range likely reflects the different inclusion criteria and culture techniques used in the referenced studies.
A positive culture more accurately guides antimicrobial selection, but it is associated with a poorer prognosis.179 Synovial biopsy for culture does not increase the chance of a positive culture compared with synovial fluid alone.178 A blood culture should also be performed, especially in the neonatal foal. If septic physitis or osteomyelitis is present, culture of debrided and necrotic bone is indicated at the time of surgery.
Ultrasonography can aid in quantifying synovial distention, identifying the presence of intrasynovial masses, thickening of the joint capsule and synovial membrane, and identifying irregularities of the subchondral bone and abnormalities of the physis. The contralateral limb is used for comparison when there are findings of questionable significance. Figs. 17.3 and 17.4 show both longitudinal and cross-sectional ultrasonographic images of the diverticulum of the lateral femorotibial joint, respectively, in a foal with septic arthritis. Radiographs of the affected and contralateral limb should be taken because concurrent infection of the physis and subchondral bone is common due to the vascular network of neonatal foal joints and extension of infection.172,180 Bone infection has been reported in 38% to 80% of foals with septic arthritis.67,101,163,166,168,172 In the initial stages of septic arthritis, radiographic changes may be absent or demonstrate mild soft tissue displacement as a result of joint distention. As progression occurs, joint
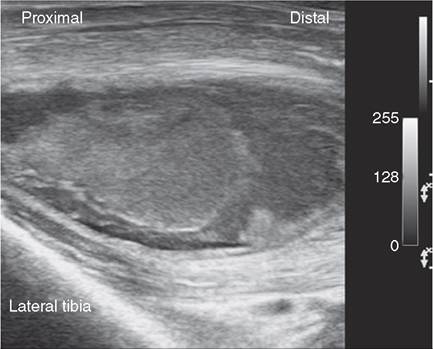
FIG. 17.3 A large mass of echogenic material consistent with fibrin. The distal aspect of the diverticulum of the lateral femorotibial joint is surrounded by hyperechoic synovial fluid.
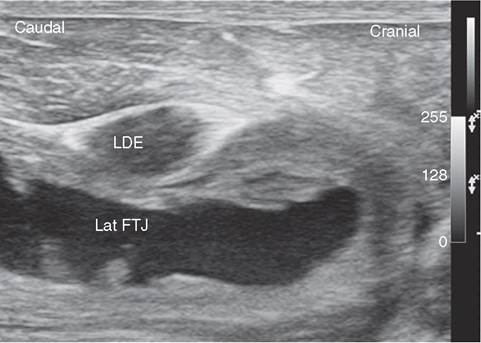
FIG. 17.4 The lateral femorotibial joint (Lat FTJ) compartment in cross-section positioned between the lateral tibia and tendon of the long digital extensor (LDE) tendon. The synovial fluid has increased echogenicity; the synovial lining and joint capsule is thickened with proliferative intrasynovial masses.
space narrowing may occur, associated with articular cartilage destruction, periosteal reaction, and subchondral bone osteolysis. Radiographic changes of bone sepsis are not evident until 7 to 10 days after the onset of infection.169 Baseline and serial radiographs over time can help to determine the progress of the disease and response to treatment.172
If radiographic examination is inconclusive or earlier identification of bone involvement is desired in cases where there is a high clinical suspicion of bone infection, advance imaging modalities should be recommended. Both computed tomography (CT) and magnetic resonance imaging (MRI) offer improved sensitivity for detection of bone and soft tissue pathology, respectively. These modalities are particularly valuable in the proximal limb or axial skeleton where overlying soft tissue and incomplete ossification of subchondral bone can limit radiographic evaluation of joint surfaces and physes.170 CT provides increased sensitivity and detail with improved detection and characterization of periarticular lesions and osteomyelitis, but it is subject to availability and often requires general anesthesia. MRI offers superior imaging of periarticular soft tissue and cartilage, but the expense of the modality, limited availability, need for general anesthesia, and time for image
acquisition limit the use of the modality for the diagnosis of septic orthopedic disease.169
It is imperative to clinically and diagnostically evaluate all other body systems in neonates with septic orthopedic disease to determine the presence of comorbidities, especially concurrent infections that have likely led to hematogenous dissemination to joints, bone, and physes. Failure to identify, diagnose, and treat comorbidities in neonatal foals will negatively influence prognosis when treating septic osteitis, physitis, or synovitis. In addition, serial body system and joint examinations are indicated on a daily basis to monitor response to therapy and identify development of additional sites of infection in joints or physes.170
Treatment
The early diagnosis of disease and initiation of aggressive therapy are paramount to successful outcomes. The cornerstones of therapy include resolution of distant underlying sources of infection, if present; systemic and local antimicrobial therapy; and drainage and lavage of the infected joint or joints. The choice of treatment regime will depend on facilities, economics, value of the foal, number and location of joints involved, any underlying disease process, presence of concurrent osteomyelitis, and identification of a causative organism.
Systemic Antibiotic Therapy
The selection of systemic antibiotics was discussed previously. Given the similarity between bacteria localized to joints of bone and those isolated from blood, the same initial protocols are warranted and should include broad-spectrum coverage, pending culture results. Despite a strong focus on local antibiotic delivery techniques for treatment of synovial or bone infection, the use of systemic antimicrobials is not negated and remains imperative for successful outcomes. This is likely due to primary and distant sources of infection and the development of multiple sites of joint infection due to hematogenous dissemination. Recently, a retrospective study of foals with septic arthritis reported that of the 85.7% of synovial fluid samples cultured that yielded growth, 62.4% were gram-negative organisms and 37.5% were gram-positive organisms.162 Antimicrobial sensitivities for the isolates in this study suggest that aminoglycosides (gentamicin and amikacin) and cephalosporins (third generations or later) would be reasonable options for empirical treatment for septic arthritis in foals if gram-negative organisms are presumed to be the cause. Gram-positive organism susceptibilities were more varied with 81% tested susceptible to trimethoprim-sulfamethoxazole and 67% to ceftiofur. Most isolates were susceptible to fluoroquinolones, but the detrimental effects on developing cartilage and tendon cells preclude routine use in foals.181,182
Doxycycline (10 mg/kg PO bid) or oxytetracycline (5 to 10 mg/kg IV q12h) have been used successfully to treat septic arthritis and osteomyelitis.164,183 Oxytetracycline has a relatively good spectrum of activity and good penetration into bone and synovial fluid. If osteomyelitis is present, continued treatment with systemic antimicrobials for up to 2 months is recommended. Serial monitoring of synovial fluid analysis is useful to determine the trend in response to therapy, but normalization should not determine when antimicrobials are discontinued due to the risk of recrudescence of infection if treatment is ceased too early.
Local Antibiotic Therapy
The local administration of antimicrobials allows delivery of higher concentrations to the tissues of interest. Intraarticular administration of antibiotics results in significantly higher synovial fluid levels than systemic routes. The technique is preferred when tourniquet application and regional perfusion are difficult, such as the proximal limb or axial skeleton. In addition, higher and more reliable antimicrobial concentrations are achieved in synovial fluid following intraarticular administration compared with regional perfusion techniques. Aminoglycosides, such as gentamicin (500 mg) and amikacin (125 to 250 mg), are commonly used (SID for 3 to 5 days) because of their effectiveness against many gram-negative pathogens. Ceftiofur sodium (125 to 500 mg) is also commonly used as an intraarticular therapy.
Regional limb perfusion techniques include intravenous (IVRP) and intraosseous (IORP) routes of antibiotic delivery, coupled with a tourniquet applied proximal to the affected joint or bone. IVRP or IORP can be performed concurrently with a joint lavage. A combination of sedation and local anesthesia or a short intravenous general anesthetic is usually required for these procedures, but these can be performed stall-side and should only take 30 to 40 minutes. The application of the tourniquet and injection of the infusate can be painful; therefore sedation and analgesia are required. Sedation can be achieved safely using diazepam (0.1 to 0.2 mg/kg IV) in combination with butorphanol (0.1 mg/kg IV). If general anesthesia is required, the regime just described serves as a good premedication, after which ketamine (2 to 2.2 mg/kg IV) can be used for induction. If additional time is required, the ketamine can be repeated. If the foal has minimal cardiovascular compromise, α2 agonists, such as xylazine (0.5 to 1 mg/kg IV) or romifidine, in combination with butorphanol, also provide good sedation and analgesia; again, general anesthesia can be achieved through a follow-up bolus of ketamine.
The antibiotic is administered into a pressurized vascular environment, which aids in diffusion of the antibiotic from the vascular system into the interstitial tissues distal to the tourniquet. This allows high concentrations of antibiotics to be achieved in the poorly perfused and infected or ischemic tissues and exudate. Regional perfusion techniques typically achieve 5 to 50 times the MIC required to inhibit common pathogens 172184185
in synovial fluid.1'2,184,185 Ihe techniques are preferred over simple intrasynovial administration, if osteomyelitis is present.
Administration of local anesthetic via the intravenous catheter or intramedullary screw before infusion of the antibiotic-saline combination is helpful in improving tolerance of the procedure, if general anesthesia is not used. The total dose of lidocaine used in the regional perfusion technique should be in the range of 1.3 to 5 mg/kg. Therefore for a 50-kg foal, the amount used should be between 3.25 and 12.5 mL of 2% lidocaine, with the lower end of the range used in very young foals because of a lack of pharmacokinetic data.
Following sedation or induction of general anesthesia, an Esmarch bandage (or equivalent 5- to 12-cm-wide elastic or rubber bandage) or a pressurized tourniquet cuff can be applied proximal to the affected region. It should only be left on for 30 minutes following infusion of the antibiotic and a maximum of 60 minutes total tourniquet application time. For IVRP a 22-gauge butterfly needle, Teflon catheter, or polyurethane over-the-needle catheter is advanced into a superficial vein below the tourniquet. A small amount of cyanoacrylate glue can be used to fix the catheter to the skin to prevent removal, kinking, or movement. Commonly used veins include the saphenous, cephalic, or palmar/plantar vessels. The perfusate (local anesthetic followed by antibiotic and saline) can be injected over 1 to 5 minutes.186 Following injection, the catheter is removed and gauze swabs are placed over the site with several wraps of tape to provide pressure. This can be removed following the removal of the tourniquet after the appropriate time. The procedure is typically repeated at 24- to 48-hour intervals for three to five treatments, depending on the response to therapy.
The intraosseous route requires a custom-made cannulated cortical screw with a welded Luer-Lok adapter or an intraosseous infusion needle (Cook Critical Care, Bloomington, Ind.). A hole is drilled through the cortex of the metacarpus or metatarsus for placement of the screw, after which time perfusate can be injected. Because of the small size of foals and the specific equipment required, intraosseous perfusion is used in limited situations or equine hospitals. In addition, increased complications are recognized with the intraosseous technique.186
The aminoglycosides amikacin and gentamicin are commonly used since most joint infections are caused by gram-negative bacteria. Penicillin, cefazolin, and ceftiofur have also been used safely in local therapy, but only in response to culture and sensitivity testing. The size of foal and the area to be infused below the tourniquet should be considered when deciding on total volume, but volumes are typically between 30 and 60 mL, with 0.9% saline used to dilute the antibiotic. If local anesthetic is used, that volume is considered as part of the total perfusate. The daily systemic dose of aminoglycoside should be reduced by the amount used in the perfusion, and the total dose used in the perfusion should not exceed the total systemic dose. The procedure should be performed at the same time of day that the systemic dose is administered. Commonly recommended doses for foals are 250 to 500 mg of amikacin, 400 to 600 mg of gentamicin, and 500 mg of ceftiofur.164,169
Complications of IVRP or IORP include soft tissue swelling at the infusion site, thrombophlebitis, difficulty in injecting during IORP, and tissue sloughing. Most of these can be avoided with careful aseptic technique, by avoiding catheter repositioning and minimizing the number of procedures.186
Antimicrobial-containing substances, including collagen or beads made of bone cement such as polymethylmethacrylate (PMMA) or Plaster of Paris (POP), can also be implanted at the site of local bone infection. Their use within joints is not recommended due to the need for removal (PMMA) and rapid dissolution or inflammation incited (PMMA/collagen sponges). These beads are readily prepared aseptically for immediate use and, when using PMMA with a heat-stabile antibiotic such as aminoglycosides, can be gas or steam sterilized for later use. The beads provide an antibiotic depot when implanted adjacent to infected bone; however, the necessity for surgical removal following resolution of infection is one of the limitations of their use. The beads can be prepared by adding 10% to 20% antibiotic (2 to 4 g) to the bone cement powder (20 g), then mixing with the liquid (monomer) until the mixture can be molded into beads or cylinders. The larger surface area allows for increased antibiotic elution.170
Intrathecal catheters and constant rate infusion pumps can also be used for local delivery of antibiotics to infected synovial cavities in foals. High antimicrobial concentrations in synovial fluid lead to high concentrations in adjacent bone and physes.187 Catheters can be passed into synovial cavities via arthroscopic guidance or placed directly. Included items are an intrasynovial catheter, flow control tubing, and an elastomeric pump (Mila International, Florence, KY.). The pump allows continuous rate delivery of the selected antibiotic solution. The flow of the pump and concentration of the solution is determined by the amount of antibiotic to be delivered over a timed period.170 Maintenance of the catheter and the pump through frequent and careful monitoring is required prevent complications, such as dislodging, blockage, or restricted delivery rates.
Drainage and Lavage of the Septic Joint
Joint drainage, lavage, and debridement are important components in the management of synovial sepsis. The aim of lavage is to reduce the number of organisms in the synovial fluid, remove debris and inflammatory products, and reduce the level of pain associated with inflammation and joint distention. Techniques include needle lavage (ingress-egress, through and through), arthroscopic lavage and debridement, or arthrotomy. Needle lavage has the most beneficial effect if performed within 24 to 48 hours after the onset of infection, or, more importantly, before accumulation of fibrin. Ultrasound can aid in determining the location for needle placement and the amount of intrasynovial fibrin. A large amount of fibrin or intrasynovial masses will compromise lavage as a result of needle plugging. It is also unlikely that fibrin will be removed by needle lavage. Aggregates of microorganisms can be sequestered in fibrin and escape the effects of antibiotics, resulting in persistence of clinical signs or recrudescence of infection once therapy has been discontinued.
For needle lavage, the skin should be clipped and aseptically prepared, and the foal sedated or anesthetized as described previously. Synovial fluid should be collected for confirmation of sepsis or for serial cytologic monitoring to assess response to treatment. If general anesthesia is not used, the joint can be distended with local anesthetic after a single needle placement. The ingress-egress lavage technique involves repeated distention of the joint with sterile saline, followed by aspiration using a single portal. The technique is indicated in joints that have difficult access or where additional needles have become plugged or displaced from the joint. Through-and-through lavage is more commonly used. After distention of the joint with sterile saline or local anesthetic, additional superficial pouches of the joint become visible, aiding in placement of further needles. Needle size is based on clinician preference, but usually 18- to 14-gauge needles are used. Practitioners placing additional needles must try to keep the joint distended to avoid iatrogenic damage to the cartilage. Precise landmarks for needle placement are not necessary, but a sound knowledge of the local anatomy and visualization of the three-dimensional structure of the joint will help to maintain correct placement of the needles during the lavage. Between 1 and 2 L of physiologic saline or lactated Ringer solution are typically used to complete the lavage. The bags can be pressurized and attached to the ingress needle, allowing the clinician to place additional needles and subtly adjust needle position to facilitate flow. The risk of using a pressure bag system is rapid delivery of saline outside the joint if the ingress needle position changes slightly. Joint lavage becomes futile once subcutaneous saline restricts the distention potential of the joint pouches. In joints with moderate periarticular soft tissue structures or swelling, the author prefers to use 20- to 30-mL syringes to lavage the joint. Any increase in resistance to injection is easily appreciated, and correction of needle placement can occur before fluid is delivered outside the joint (Fig. 17.5). The use of different ingress needles is recommended to increase turbulence and facilitate removal of joint debris, irrespective of whether syringes

FIG. 17.5 Lavage of a septic joint using a syringe and separate egress needle.
or pressurized bags are used. This also prevents the egress needles from plugging with fibrin. On completion of the lavage, as much fluid as possible should be expressed before removing all needles except one, which can then be used to administer intraarticular antibiotic.
The number and frequency of needle lavages are determined by the response to treatment. If the clinical signs progress in the face of 3 to 5 days of systemic and local antibiotic therapy and needle lavage, then reevaluation of the foal including US and radiography is indicated. Signs of treatment failure include persistent lameness or pyrexia, periarticular swelling, persistence or worsening of joint effusion, additional joint involvement, or failure to decrease synovial cell counts or differential. It is important to identify if there has been subchondral bone lysis. Treatment failure may prompt an antibiotic change and/or more aggressive joint lavage via arthroscopy or arthrotomy, if arthroscopy is not available. Arthroscopy offers many advantages over needle lavage and arthrotomy and is the preferred choice for chronic or refractory cases of synovial infection, or those where there is evidence of fibrin or subchondral defects within the joint. The technique permits superior visualization of most aspects of the joint, including the articular cartilage, bone, joint capsule, and synovial membrane. Targeted lavage and debridement can be achieved for removal of fibrin and debris, synovial resection, and debridement of necrotic cartilage or subchondral bone. Arthroscopic and arthrotomy approaches and intraarticular anatomy of commonly affected joints are reviewed comprehensively elsewhere. Arthrotomy is generally reserved for chronic or refractory cases that have been poorly responsive to other forms of lavage and debridement. It is imperative that a sterile absorbent bandage is maintained for drainage of synovial fluid to reduce the risk of ascending infection.
Generally, the duration of local antimicrobial administration (intraarticular, regional perfusions or continuous delivery systems) is determined by clinical and synovial cytologic improvements, including resolution of joint swelling, lameness, and a neutrophil percentage below 80%. Systemic antimicrobial administration is usually continued for a minimum of 2 weeks beyond the resolution of clinical signs.170
Septic Osteomyelitis
Septic osteomyelitis occurs as a primary disease entity or concurrently with septic synovitis, with infections commonly occurring at the epiphysis of long bones, metaphyseal side of growth plates, costochondral junctions, and articular facets of vertebral bodies. Radiographic evidence of osteomyelitis includes regions of focal loss of bone density, osteolysis, or sequestrum formation. Necrotic bone can act as a nidus for continued bacterial growth. The treatment of osteomyelitis includes systemic and local antibiotics and possible debridement.164,188 Necrotic subchondral bone can be debrided using arthroscopy, and infected physeal bone can be debrided under radiographic or fluoroscopic guidance. Debridement of necrotic bone is not indicated in extensive lesions where mechanical joint stability may be jeopardized or where the surgical access and debridement would create significant surgical complica- tions.4, Evidence suggests that surgical curettage may not offer significant advantages over prolonged systemic and local antibiotic therapy alone.164,183,189 In addition to the regional perfusion techniques described previously, there is occasional indication for implantation following debridement of antibiotic impregnated polymethylmethacrylate, calcium sulfate, or collagen sponges. These substances elute antibiotic at the site of bone infection.1'1
IV tetracycline (5 to 10 mg/kg IV q12h) or oral doxycycline (10 mg/kg bid PO), along with local treatment with amikacin (IVRP or IA 250 to 500 mg), is indicated if culture and sensitivity results suggest susceptibility, or if culture results are unavailable. Surgical debridement is indicated if there is radiographic evidence of sequestrum formation, chronicity of the disease in the face of medical therapy, or progression of the osseous infection.
In cases of osteomyelitis, serial monitoring of fibrinogen or SAA may aid in determining the response to therapy. A positive response results in decreasing SAA levels over 48 to 72 hours, and this commonly precedes improvement in lameness.
Management and Adjunctive Therapy
Nonsteroidal antiinflammatory drugs (NSAIDs) are indicated in the management of septic orthopedic disease resulting from antiinflammatory, analgesic, and antipyretic effects. Commonly used NSAIDs include flunixin meglumine, ketoprofen, phenylbutazone, and, less commonly, ibuprofen. Dosages cannot be directly extrapolated from adults because healthy foals have a greater volume of drug distribution and prolonged clearance.190 For flunixin and ketoprofen, this results in a dose rate that is 1.5 times that of the adult dose and extension of the dosing interval to q24h. The drugs should be used judiciously in compromised or critically ill foals because of the potential adverse effects such as gastrointestinal (GI) ulceration, nephrotoxicity, and platelet dysfunction. Oral meloxicam at a dose rate of 0.6 mg/kg q12h achieves plasma concentrations that are likely therapeutic without evidence of drug accumulation in plasma. Foals appear to be more resistant to the adverse effects of meloxicam than adult horses, and drug clearance was more rapid in foals.190 If additional analgesia is required, butorphanol (0.05 to 0.1 mg/kg IV or IM) or transdermal fentanyl patches (100 μg∕h patch) can be used safely in foals. The clearance and systemic uptake of butorphanol are faster in foals, suggesting that higher doses may be required. A dose rate of 0.1 mg/kg of butorphanol-provided analgesia for 150 minutes in 4- and 8-week-old pony foals.191
The affected limb should be bandaged during treatment to cover needle/arthroscopy portals, provide compression and support to the limb, limit swelling and reduce pain, and absorb exudate if an arthrotomy has been performed. Application of bandages with adequate padding in the secondary layer is recommended in the distal limb because of the combination of thin skin, bony protuberances, and minimal subcutaneous soft tissues. Adhesive dressings can be used over joints where a bandage cannot be maintained.
Restoration of joint health and range of movement is important following infection. Gentle forced flexion and extension of the joint while non-weight bearing will help maintain joint function and movement. The foal should be stall confined and weight-bearing exercise avoided for 3 to 4 weeks following the resolution of infection and clinical signs. The stall should have a deep bedding of clean straw to reduce the risk of pressure necrosis during recumbency. The stall should be cleaned two to three times a day to reduce the risk of the foal lying in feces or urine-soaked bedding. Handlers and clinicians should use strict personal hygiene when treating foals. Controlled hand walking of the mare on a daily basis for 1 to 2 weeks should be initiated before free turnout.
The decision to discontinue antibiotic therapy is based on clinical judgment and resolution of clinical, hematologic, radiographic, and cytologic abnormalities. Generally, local antibiotic therapy and lavage are continued until normalization of the synovial fluid and cytology, and systemic antibiotic therapy is continued for 2 to 3 weeks beyond the resolution of clinical signs.
Prognosis
The prognosis of foals with septic arthritis/osteomye litis is dependent on a number of factors, but short-term survival is considered good to excellent with studies reporting 71% to 81% survival to discharge.101,163,166 The prognosis for future athletic performance is less favorable, with 30% to 48% of foals affected with septic arthritis/osteomyelitis going on to race.101,166,167 Factors affecting prognosis include prolonged duration (>24 hours) of signs before the initiation of treatment, concurrent systemic disease or comorbidities, the number of joints infected, the location of infected joints, the presence of concurrent osteomyelitis, and the type and diversity of bacteria involved. The financial constraints for treatment, facilities, and technical skill available for treatment and the expected long-term use of the foal can also affect outcomes.164,166,167,171,172 These factors and the high cost and long duration of treatment should be considered when counseling owners. Foals that are treated expediently with appropriate systemic and local antibiotic therapy and without concurrent disease may have a more favorable prognosis for survival and athleticism than previously indicated.162,170
Noninfectious Causes of Lameness

FIG. 17.6 Rupture of the gastrocnemius muscle.
joint malformation, or other physiologic causes such as intrauterine malpositioning. They are described with reference to the affected joint and can occur in the carpus, fetlock, pastern, coffin joint, or tarsus. Diagnosis of contractural deformities is relatively straightforward based on the inability to straighten affected joints and difficulty in standing and movement at birth as a result.172 This predisposes to failure of passive transfer of immunoglobulin by impeding the ability to adequately nurse. The degree of contracture varies from mild to severe and may be associated with scoliosis and/or torticollis.193 Conservative therapy consisting of bandaging or splinting the limbs to induce tendon laxity may be helpful. Care must be taken to provide adequate padding under the splint and to reset the splint every day. Oxytetracycline (2 g slow IV) in combination with splinting induces relaxation of the musculotendinous unit, and although results can be remarkable, they are not always reliable172; repeat treatments are often required.
Twins, premature foals, foals that are small for gestational age, and foals with in utero-acquired infection are likely to have incomplete ossification of cuboidal bones at birth. Foals with substantially reduced ossification may damage bone with limb loading. Limited exercise may be prudent until ossification begins to increase radiographically, which can be within 7 days. Hypothyroidism has been identified in foals with angular limb deformities, contracted tendons, and tarsal bone collapse.
Young foals can suffer physitis when there is excess load caused by overexercise or weight on the newly forming bone, or as a result of normal loading on abnormal conformation. The physis of the distal metacarpus/tarsus or proximal phalanx is most commonly affected. Clinical signs can vary and be subtle, such as a stiff gait, shortened cranial phase of stride, trembling when standing, or buckling forward at the carpus or fetlock. Pain in the physis can lead to contracture of fetlock tendons. Treatment is aimed at reducing pain with antiinflammatory therapy and reducing exercise level or correcting underlying angular limb deformities.172
Other causes of lameness and swelling associated with joints include cellulitis, hemarthrosis, subsolar/solar bruising of the foot, and hoof wall cracks causing laminae pain.