Septic (Infectious) Arthritis and Osteomyelitis
Joanne Hardy
■ Incidence and Risk Factors Septic arthritis can result from extension of a periarticular wound infection, traumatic inoculation, iatrogenic inoculation, or hematogenous inoculation.
The hematogenous route is the most common avenue of inoculation of organisms in a joint in foals, and bacteremia and septicemia are the most important risk factors for septic arthritis in foals. In one study, septicemia was the most common cause of death (30%) in foals younger than 7 days of age; septic arthritis was identified as the cause of death in 12.5% of foals ages 8 to 31 days.1 In adults, articular wounds are reported to be the most common cause of joint infection, followed closely by iatrogenic intraarticular injection; postsurgical infection and idiopathic (unidentified cause) infection are also reported in association with septic arthritis in adult horses.2-4 Although uncommon, hematogenous spread from a distant focus is possible in adult horses.5Establishment of infection depends on several factors, including size of inoculum, host defense, virulence of the organisms, and local joint factors. In foals, host defense is mainly associated with passively acquired immunity. Failure of transfer of passive immunity (FTPI) is the greatest risk factor for development of septicemia in foals.6 The incidence of disease resulting from FTPI has been reported to be as high as 78%. Organism virulence is related to the ability to establish infection. Attachment factors, ability to resist phagocytosis, and resistance to cell killing all contribute to the establishment of infection. Local joint factors that may predispose to establishing or maintaining infection include low blood flow, particularly in end-capillary loops, and poor blood supply, more prominent in bone. In adults, certain intraarticular medications (e.g., corticosteroids, hyaluronate, polysulfated GAGs) have been associated with a higher risk for septic arthritis, potentially by decreasing articular defense.7,8
In calves, septic arthritis is associated with FTPI and septicemia and with feeding of mastitic milk (Mycoplasma).9,10 In older cattle, direct spread from a perisynovitis is the most common cause, and the distal interphalangeal joint (DIJ) is most often involved.

FIG. 38.13 Radiograph of a foal with type E septic arthritis, showing involvement of the distal femoral epiphysis (arrows).
■ Pathogenesis Articular blood supply is provided through a main arteriole that branches to the synovial membrane and epiphysis. Blood supply to the metaphysis is provided by the nutrient artery, but in young foals transphyseal vessels exist that connect the metaphyseal and epiphyseal blood supply.11 Experimental intravenous (IV) injection of bacteria results in rapid inoculation of articular and periarticular capillaries. Five types of hematogenous articular infection have been described: type S (synovial), where a septic arthritis results from inoculation of the synovial membrane; type E (epiphysis), where subchondral bone infection is present (Fig. 38.13); type P (physis), where infection of the physis occurs on the metaphyseal side of the growth plate (Fig. 38.14); type T, observed in premature foals, with infection of the small tarsal or carpal bones (Fig. 38.15); and type I, where joint invasion occurs after a periarticular soft tissue abscess (Fig. 38.16).12 In young foals, functional trans- physeal vessels allow communication of the metaphysis and epiphysis, such that bacteria localize preferentially in the synovial membrane and subchondral bone. Thus young foals predominantly have infectious arthritis types S and E. Closure of transphyseal vessels occurs after about 7 to 10 days of age, such that localization of infection to the metaphyseal vessel loops occurs in older foals.11 Although bone inoculation can occur simultaneously with synovial inoculation in young foals, determination of bone involvement can be delayed until radiographs identify the lesions. In foals the hock, carpus, and stifle are frequently involved in hematogenous joint infection, but it is important to remember that any joints, including those of the vertebral column, can be affected.
In young foals, Actinobacillus equuli, Salmonella spp., Escherichia coli, and other Enterobacteriaceae are often involved; in older foals, Streptococcus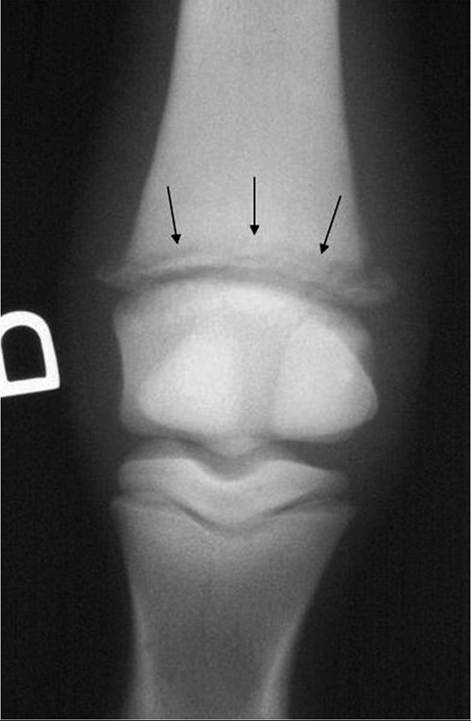
FIG. 38.14 Radiograph of a foal with type P septic arthritis, showing involvement of the distal metacarpal physis (arrows).
spp. and Rhodococcus equi are common isolates. In foals with type P (physeal) involvement, Salmonella and Rhodococcus spp. are typically involved.
In adults, inoculation of the joint from an articular wound is the most common cause of joint sepsis. The establishment of infection will depend on size of the inoculum, pathogenicity of the bacteria, and duration before treatment. In one study, 53% of horses examined within 24 hours of an open joint wound developed septic arthritis, versus 92% of horses examined within 2 to 7 days of injury and 100% of horses examined after 7 days.13 However, two studies failed to find a relationship between interval before admission and outcome.14,15 This suggests that many other factors influence the prognosis following joint infection. Joints of the lower limb (fetlock, coffin joint) are often involved in open joint injuries because of the poor tissue coverage in those areas.3,16 Organisms frequently encountered in open joint wounds include Enterobacteriaceae, streptococci, and staphylococci.3,16 These injuries are also likely to have multiple bacterial infections. Wounds near the hoof are more likely to have anaerobic infection, and Clostridium is the most common isolate. Fungal organisms are a rare cause of septic arthritis in horses but should be considered if isolated in pure culture more than once.5
Iatrogenic joint injection is the second most common cause of septic arthritis in adults, followed by postoperative infection. The tarsus is the joint most often involved in septic arthritis after joint injection, whereas the carpus is the most common joint

FIG.
38.15 Radiograph of the tarsus of a premature foal with type T septic arthritis, showing involvement of the distal tarsal bones (arrows).
FIG. 38.16 Photograph of a foal with type I septic arthritis where a soft tissue abscess (arrow) dissected down into the coxofemoral joint.
involved after surgery.2,3 Staphylococci, particularly Staphylococcus aureus, are the most common organism isolated after iatrogenic joint injections or surgery. When S. aureus is isolated from a joint infection, care should be taken to determine the possibility of methicillin resistance.17,18 The risk of septic arthritis after
arthroscopic surgery is low, seen in only 8 of 627 joints (1.3%) in one study.19 Interestingly, in these horses clinical signs did not develop until several days after discharge.
In calves, the most common isolates are Streptococcus spp. and Mycoplasma bovis.2 In adult cattle, common pathogens involved in septic arthritis include Mycoplasma bovigenitalium, Mycoplasma mycoides, Brucella spp., and Trueperella pyogenes (formerly Arcanobacterium pyogenes), which is most often involved.21 In sheep, goats, and calves, Chlamydia psittaci polyarthritis can occur as an endemic or epidemic disease and may be accompanied by keratoconjunctivitis.22,23 In lambs, Erysipelothrix rhusiopathiae is also a cause of polyarthritis, gaining systemic entrance through the stump of docked tails or a castration site. Improving hygiene during these procedures helps prevent the disease.22 In sheep and cattle, the obligate intracellular organism Chlamydia pecorum has received increased recognition.24 Involvement of this organism is thought to be underrecognized because diagnosis is based on serology and histopathology, which are not necessarily diagnostic methods used in the early stages of the disease.
■ Diagnosis Septic arthritis, osteomyelitis, or physitis should be ruled out in any lame foal.
Foals with septicemia are at high risk of developing septic arthritis, which generally is noted clinically hours to days after the initial signs of septicemia. Although owners often complain of external trauma, septic arthritis is the most common cause of lameness in foals. In young foals with types S and E arthritis, inoculation of the synovial membrane is the first event, which the astute clinician can identify as periarticular edema. Joint effusion rapidly follows. Involvement of multiple joints is common, and identification of all affected joints is essential for successful management. Because effusion of the shoulder, elbow, or hip joints is more difficult to detect by palpation, arthrocentesis of these joints should be performed in foals with an unidentified lameness. In the stifle, femoropatellar joint involvement results in marked effusion, but femorotibial joint effusion is usually more difficult to discern. Because of the usual communication between the femoropatellar and the medial femorotibial joint, both are typically involved concurrently. Lateral femorotibial infection is more subtle and can occur separately. Distention of the long extensor pouch is often present in lateral femorotibial infection and suggests involvement of that joint. In foals older than 7 days, physeal infection may be observed. With physeal infection, presence of concurrent synovial effusion depends on the intraarticular or extraarticular localization of the growth plate. For example, distal metacarpal physeal infection results in periphyseal edema, initially without joint effusion. The infection can break through the skin rather than involve the joint. In foals with septic arthritis, the CBC is consistent with an inflammatory response and includes a neutrophilic leukocytosis and hyperfibrinogenemia. In one study in foals, a plasma fibrinogen concentration of 900 mg/dL or higher (as measured by the heat precipitation method) was useful as an indicator of physeal or epiphyseal osteomyelitis, with positive and negative predictive values of 84.2% and 98.2%, respectively.25Adult horses usually show minimal changes on the CBC and little change in systemic signs, so development of or increasing lameness after a wound, joint injection, or surgery indicates the need for further examination.
In one study, the mean and median times for readmission for septic arthritis after an elective arthroscopic procedure were 47 and 20 days, respectively.19 In that study, the authors speculated that the delay in onset of septic arthritis following surgery was an indication that joint inoculation occurred in the postoperative period rather than intraoperatively, supporting careful joint closure and continued aseptic technique when changing bandages in these horses.19 Because of their potent antiinflammatory properties, corticosteroids may delay the onset of clinical signs of septic■ TABLE 38.1
Characteristics of Synovial Fluid According to Condition in Large Animal
Degenerative
| Characteristic | Normal | Septic | Joint Disease | Inflammatorya |
| Color | Clear | Yellow/green, serosanguineous | Yellow | Yellow to iridescent |
| Clarity | Transparent | Turbid | Transparent | Translucent |
| Fluid volume | Low | Increasedb | Low | Increased |
| Viscosity | High | Low | Variable | Low (usually) |
| WBCs∕μL | 30,000 | 75 | ||
| Total protein (g/dL) | 2.5 | 1 | ||
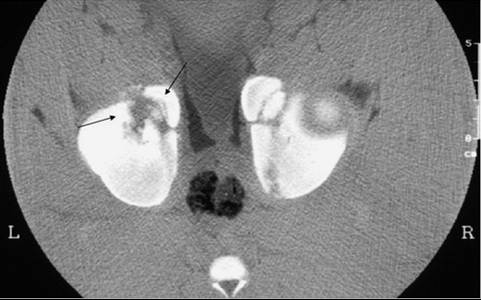
| Glucose | Equal to blood | 2.5 g/dL) and high white blood cell (WBC [leukocyte]) count are observed. Classic counts diagnostic for septic arthritis in foals exceed 30,000 cells/jL, with more than 80% neutrophils; cell counts above 10,000/jL may indicate early infection. Neutrophils are not always degenerate. Gram stain is a useful diagnostic tool because it may identify the etiologic agent in up to 25% of cases in which culture results are negative.27 In foals with a separate physeal infection where the physis is extraarticular, sympathetic joint inflammation and effusion can occur.28 This manifests as a moderate increase in WBC count, with less than 90% neutrophils. The presence of such cytologic findings should alert the clinician and practitioner to the presence of physeal sepsis. Several studies have examined the usefulness of synovial fluid markers to predict joint sepsis. In one study, synovial fluid D-dimer concentration was markedly increased in septic joints, and this was not influenced by the presence of septicemia.29 However, inclusion criteria for the study included the presence of a synovial fluid analysis consistent with sepsis, so it is not known whether D-dimer concentration would be a useful marker earlier in the disease process or when results of synovial fluid analysis are equivocal. In another study, synovial fluid equine myeloperoxidase (MPO) activity was compared in different forms of joint disease. In cases of septic arthritis, MPO activity in synovial fluid was significantly increased compared to control. Although the study concluded that synovial fluid MPO may be useful as a marker of septic arthritis in horses, further studies are needed because horses were included in the study when they already had synovial fluid analysis indicative of septic arthritis.30 Serum amyloid A (SAA) is an acute-phase protein that is markedly increased (>1000 mg/dL) in horses with septic arthritis.31 Interestingly, SAA concentration was not increased in synovial fluid collected after repeated intraarticular injections of amikacin in healthy horses.32 Intraarticular injection of various substances such as antibiotics, saline, or therapeutic agents often cause a transient inflammatory reaction where total protein and nuclear cell counts are consistent with sepsis.33 The use of SAA to differentiate inflammation from infection warrants further study. Increased lactate concentration has recently been measured and used as a rapid test for identification of septic arthritis, but the sensitivity and specificity of this measurement are currently unknown. In adult horses with a wound localized near a synovial structure, it is crucial to identify as early as possible whether there is synovial involvement. The most convincing evidence is demonstration of synovial communication with a wound by injecting a sterile solution into the synovial structure and observing fluid exiting the wound. For this purpose, a site remote from the wound and covered with normal skin should be prepared aseptically, and depending on the structure involved, 20 to 200 mL of a sterile solution (e.g., saline, balanced electrolyte) is injected after collecting synovial fluid samples using aseptic technique.34 If synovial involvement is detected, therapy is immediately instituted. Radiographs of all affected joints are essential. The presence of osteomyelitis may affect prognosis and dictate prolonged antibiotic therapy. Radiographs should be repeated weekly until clinical signs resolve themselves or at any time there is deterioration in the clinical condition. Radiographs are also indicated whenever a change in therapy is planned (e.g., from IV to oral antibiotics). Nuclear scintigraphy has been used to diagnose infectious foci in odd localizations in foals. For example, vertebral and atlantooccipital involvements have been diagnosed using this imaging modality. It must be remembered that local bone infarcts, which are often present in osteomyelitis, will result in areas of decreased rather than increased uptake. Scintigraphy using technetium-99m (99mTc)-labeled WBCs or ciprofloxacin labels has potential uses in foals with multiple-limb involvement and warrants further investigation as an imaging modality for septic arthritis.35 Computed tomography (CT) is a useful imaging modality to identify osteomyelitis (Fig. 38.17). It is particularly useful for imaging areas that are difficult to detail with radiography.36 The main disadvantage is that it is currently limited by the size of the animal. Magnetic resonance imaging (MRI) has been used in foals and adults with septic arthritis.37,38 In a limited series comprising 6 foals with infectious arthritis, 4 of the 6 had infectious lesions on MRI indicative of osteomyelitis, and only 4 of 19 lesions were detected on digital radiographs. Osseous lesions in the T2-weighted, short tau inversion recovery (STIR), and proton density MRI sequences appeared as hyperintense foci.38 In addition, joints with infectious arthritis had heterogeneous signals within the synovial fluid, whereas all nonseptic joints
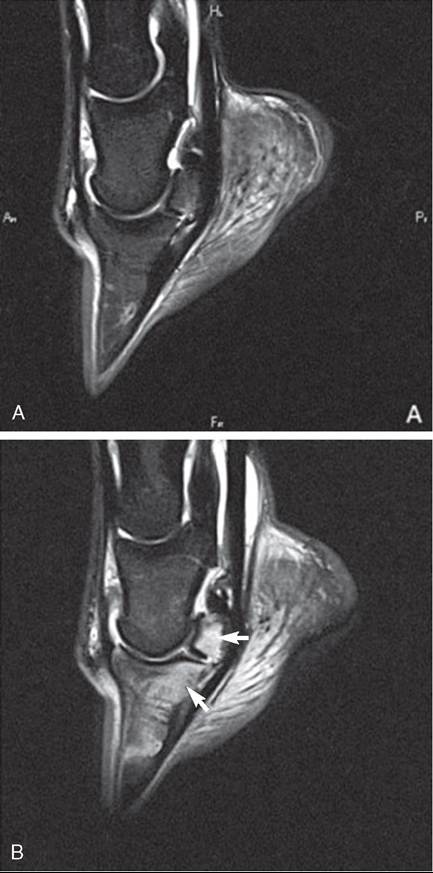
FIG. 38.17 Computed tomography scan of a foal with septic arthritis of the left coxofemoral joint, showing osteomyelitis of the acetabulum (arrows) that was not radiographically evident. had homogeneous fluid signals.38 In adult horses with septic arthritis, MRI findings included diffuse hyperintensity within bone and extracapsular issue on fat-suppressed sequences (Fig. 38.18). The study concluded that MRI may allow earlier and more accurate diagnosis of septic arthritis in horses, particularly when the clinical diagnosis is challenging.37 Identification of the organism should be attempted in all cases of septic arthritis. Gram stains, culture of synovial fluid in blood culture bottles, and culture of synovial biopsies have been suggested to increase the likelihood of identifying the organism. In general, the positive culture rate from synovial fluid samples is approximately 50%, and synovial biopsy culture has a low yield to increase this figure.39 Appropriate culture techniques should be used for organisms such as Chlamydia or Mycoplasma spp., and special stains may be required. Serology and histopathology are required for the diagnosis of C. pecorum in sheep and cattle.24 In foals, because bacteremia or septicemia precedes the local signs, blood cultures should be obtained. In addition, any other local sites of infection should be cultured. In cases of septic physitis, needle aspiration of the affected site under radiographic or fluoroscopic guidance can be performed. In the future, other techniques for early identification of synovial sepsis may become available.39 ■ Treatment Septic arthritis is an emergency. Assessment followed by institution of treatment should be done as soon as possible after problem identification. The principles of treatment of septic arthritis include systemic broad-spectrum antibiotics, local joint lavage and debridement, and local antibiotic delivery. Systemic antibiotics are best administered intravenously to ensure adequate tissue concentrations. Most often the combination of a β-lactam and an aminoglycoside or fluoroquinolone is used in adults; a β-lactam and aminoglycoside combination is most often used in foals, because fluoroquinolones may have detrimental effects on articular cartilage in young animals. In open joint injuries, particularly if an anaerobic organism is suspected, metronidazole may be added to the antibiotic regimen. Gram-positive organisms can be isolated from blood cultures in up to 33% of foals with sepsis, so gram-positive coverage is also important.40,41 In foals with physeal involvement, Gram stain and culture of a physeal aspirate are helpful to identify the causative agent. The most common organisms isolated from septic physitis are Salmonella spp. and R. equi. If R. equi is identified, appropriate therapy with macrolides and rifampin should be instituted, keeping in mind that macrolide-resistant organisms have been reported; obtaining susceptibility patterns may be warranted.42 Intestinal uptake of clarithromycin is significantly impaired when it is
FIG. 38.18 Sagittal short tau inversion recovery weighted magnetic resonance imaging sequence of the left (A) and right (B) feet of a horse with septic navicular bursa and septic navicular bone, showing severe hyperintensity of the navicular bone and distal phalanx (arrows). administered in combination with rifampin, so use of that combination should be questioned.43 The presence of osteomyelitis warrants an antibiotic combination that reaches effective bone levels; rifampin with another antibiotic is often used. Rifampin should not be used as the sole antimicrobial because resistance is acquired rapidly with this antibiotic. Other antibiotics that reach effective bone concentrations include tetracyclines, chloramphenicol, fluoroquinolones, and cephalosporins. If cephalosporins are chosen, third-generation agents (e.g., ceftiofur, cefotaxime, ceftriaxone, ceftazidime) are preferred because they are more effective against gram-negative bacteria. In foals, fluoroquinolones should be reserved for organisms that are only susceptible to this class of drugs because evidence shows cartilage lesions developing in immature animals with their use.44,45 Local lavage of the joint or synovial structure is an important component of therapy; removal of debris, fibrin, and inflammatory mediators helps minimize damage and eliminate the organism. In foals, joint lavage can be performed under heavy sedation or short-term general anesthesia. In adults, sedation and a regional block or short-term general anesthesia can be used. Joint lavage can be performed using through-and-through needle technique; use of a pressure bag or a pump will facilitate efficient lavage of several liters of fluids through the joint. This technique may be sufficient in joints where the diagnosis was made early, where the infection is not severe, and in simple joints (fetlock, carpus). If there is poor response to treatment after one or two sequential joint lavages, arthrotomies should be performed without hesitation. Often fibrin accumulation in the affected joint precludes effective lavage and allows sequestration of bacteria. Once arthrotomies have been performed, the affected joint needs to be covered with a sterile bandage. During subsequent lavages, a teat cannula inserted in the arthrotomies may be used to lavage the joint. The arthrotomies are left to heal by second intention; the joint needs to remain bandaged until the arthrotomies are closed. Occasionally, delayed closure of the arthrotomies is necessary, particularly in arthrotomies localized over high-motion joints. In joints with multiple compartments (stifle, hock), in severe infection or osteomyelitis, in cases of longer duration, or in animals with poor response to joint lavage, arthroscopic debridement is indicated.15 Arthroscopy has several advantages over simple needle lavage. It allows thorough debridement, removal of fibrin, and lavage of all compartments; evaluation and debridement of cartilage and underlying bone lesions; and in the case of wounds, identification and removal of foreign material. In one study, foreign material was identified on arthroscopy in 41 of 121 (43%) horses and 34% of joints with wounds involving synovial structures; these were predicted in only 15% of cases, suggesting that endoscopic evaluation is important diagnostically in wounds involving synovial struc- tures.15 In addition, arthroscopy may have prognostic value when radiographic lesions are equivocal. The arthroscopic portals can be left open for drainage and subsequent lavage but must be kept under a sterile bandage. Local or regional delivery of antibiotics is advocated for the management of septic arthritis.46 Delivery of local antibiotics to the affected joint can be achieved by intraarticular injection, isolated IV or intraosseous (IO) infusion, isolated retrograde venous injection, continuous antibiotic delivery, or implantation of antibiotic-impregnated biocompatible materials. Intraarticular injection is the simplest method but requires repeated injections. Aminoglycosides (gentamicin, amikacin) and ceftiofur have been shown to maintain levels above the minimum inhibitory concentration (MIC) for 24 hours after a single intraarticular injection.47,48 Intrasynovial catheter placement and repeated antimicrobial injection was described successfully in one study where a modified over-the-wire catheter system was placed directly in the synovial structure and used for antibiotic injection and lavage of the synovial structure.4 Continuous infusion of antibiotics can also be accomplished by placing a small catheter into the affected synovial structure and attaching it to an infusion system, providing constant rate infusion of the antibiotic.49,50 Isolated regional IV perfusion or IO perfusion techniques are also advocated for the treatment of septic arthritis.51,52 Although the term perfusion is often used in the veterinary literature, the term infusion should probably be used, because in most studies a single injection of the antibiotic is made at the start of the treatment period, whereas perfusion techniques establish an extracorporeal bypass system for the extremity or organ under treatment.53 Isolated limb infusion techniques are based on isolating the area of interest with a tourniquet, followed by a single IV or IO injection of the antimicrobial. These techniques rely on transient pressure and concentration gradients to distribute a drug to the tissues. The type of tourniquet used is important; escape into the systemic circulation must be avoided during the treatment period. Wide rubber or pneumatic tourniquets are recommended.54 An Esmarch tourniquet has also been shown to be effective.51,53 Tourniquets should be 20% wider than the diameter of the limb on which they are used.54 After tourniquet placement, a regional vein is catheterized using a 23-gauge butterfly catheter for isolated limb infusion. Alternatively, a long-term indwelling catheter can be placed in the vein to facilitate treatment and avoid repeated injection and possible damage to the vein.57,58 The antibiotic is diluted in a volume of sterile fluid (20 to 120 mL have been reported) and subsequently injected, and the tourniquet is left in place for 30 to 45 minutes. In theory, the increased volume serves to increase the vascular pressure and therefore antibiotic distribution, but it remains unknown whether distribution of the antibiotic is a result of a pressure gradient or a concentration gradient. The increased pressure generated after a single infusion of 60 mL returned to baseline after 10 minutes in one study.53 For IO infusion, a tourniquet is placed in a similar manner, and an IO screw is placed in the medullary cavity and used to inject the antibiotic. Alternatively, a sterile infusion line can be placed in a hole drilled into the medullary cavity. In one study, the IV infusion method had fewer complications than the IO route.59 Several drugs have been used for IV infusion, including aminoglycosides, cephalosporins, erythromycin, enrofloxacin, vancomycin, and amphotericin B.51,60-64 The irritating property of drugs like enrofloxacin makes their repeated use undesirable unless no alternative is available.65 Isolated limb retrograde venous injection (ILRVI) was compared to isolated limb infusion (ILI).53 The ILRVI technique was similar to that reported for regional limb perfusion in horses. The ILI technique consisted of catheterization of one digital artery and vein followed by application of a tourniquet. The antibiotic was then injected over 3 minutes, followed by circulation of infusate and blood from the venous to the arterial circulation in 5-minute aliquots for 25 minutes. In the ILI technique, high pressure within the venous system was sustained for the duration of treatment, compared to the ILRVI technique. There was no difference between the two techniques in the pharmacokinetics of synovial fluid amikacin in the metacarpophalangeal joint, but significantly higher amikacin concentration was measured in the DIJ.53 The authors concluded that either ILRVI or ILI may be used for antibiotic delivery, but that the technically less demanding ILVRI technique may be more practical.53 Recently, time to reach maximal concentration of amikacin in the DIJ after ILVRI was shown to be only 15 minutes,66 suggesting that tourniquet application could be shortened to 15 minutes, compared to the traditional 30 minutes. This would be an advantage when the technique is used in standing horses, who often become uncomfortable after approximately 20 minutes of tourniquet application, resulting in motion and possibly systemic leakage of the antibiotic. Antibiotic-impregnated polymethylmethacrylate (PMMA) beads can also be used, although direct implantation into a joint can result in cartilage damage.67-69 PMMA implants are fabricated by mixing the desired antibiotic with the powder before adding the polymerizer. Antibiotics evaluated for inclusion in PMMA include gentamicin, metronidazole, vancomycin, ceftiofur, cefazolin, and amikacin.70-77 Antibiotic combinations have also been used, but combining antibiotics can change their elution properties. For example, cefazolin or amikacin elute at concentrations greater than MIC for 30 days in vitro, but the combination elutes above MIC for only 6 days.76,77 Antibiotic-impregnated biodegradable implants include synthetic and natural carriers. The advantage of these implants is that 7880 a separate procedure for their removal is unnecessary/8-80 Synthetic carriers are degraded by hydrolysis, which may affect the antibiotic prior to its implantation.46 Although synthetic biodegradable carriers have been evaluated in an experimental model of synovial membrane sepsis, they are not currently clinically available.78 Gentamicin-impregnated collagen sponges consist of highly purified cattle collagen; the gentamicin molecules are embedded within the pores of the collagen. No stabilizing agents or foreign substances are added. Clinical use of successful treatment of septic arthritis in horses and cattle has been reported.80-82 However, a recent study performed in healthy horses failed to detect sustained antibiotic release beyond that obtained with a single intraarticular injection.83 As high levels of antibiotics are reached within the targeted tissues with these techniques, it remains unknown whether systemic antibiotics are still required. In addition, the best dosing interval between treatments is unknown; for example, with concentration-dependent aminoglycosides, there is a transient reversible adaptive resistance for some bacteria to a second dose of aminoglycoside up to concentrations 128 times MIC. These same bacteria revert to original susceptibility when exposed to drug-free media.53,84 Another unknown is the potential interaction of aminoglycosides and β-lactam combinations, which depending on the drug combination, can be synergistic or antagonistic. Although inactivation of certain β-lactam antibiotics by certain aminoglycosides in vitro has been documented, several studies document in vivo syner- gism.85,86 Significant postantibiotic effects were detected with several antibiotic combinations.87 With extensive physeal lesions in foals, curettage, autologous bone grafting, and external coaptation may be required.88,89 The addition of tricalcium phosphate granules or bioresorbable paste may be considered.90 Angular limb deformities may result from growth disturbances or collapse of the physis on the affected side. In adults with septic arthritis and osteomyelitis, curettage of the bone lesion followed by bone grafting and external coaptation may also be indicated.91 Adjunctive therapies that may help alleviate inflammation include sodium hyaluronate, polysulfated GAGs, and dimethyl sulfoxide (DMSO). Sodium hyaluronate and polysulfated GAGs can be used systemically or locally, but local use should be reserved for when infection is under control because these agents decrease joint defense mechanisms.8,92 Although DMSO has significant antiinflammatory properties in joints, it should be used with caution because of its negative effects on cartilage metabolism.93 In addition to specific therapies, management of pain, stress, and other metabolic disturbances are indicated. Pain can be managed by judicious use of NSAIDs, using the smallest dose that will keep the animal comfortable. If a foal continues to show severe pain despite appropriate treatment, it is important to ensure that other joints in the limb are not involved. Other pain management modalities (e.g., opiates, fentanyl patches, epidural analgesia) can be used. It is important to remember that in foals, continued pain in one limb may result in development of a varus deformity in the contralateral weight-bearing limb owing to the tripod stance these foals acquire to maintain the weight-bearing limb under the center of gravity. Application of a lateral extension to the contralateral foot may help increase the weight-bearing surface and prevent development of this complication. Continued pain is a negative prognostic indicator in the affected foal. In adults, continued pain in one limb may result in the development of contralateral limb laminitis.94 When continued pain in the treated limb is a problem, preventive measures (e.g., hoof support, therapeutic shoeing) should be undertaken. Gastroprotective agents are indicated in foals and adult horses that are in pain, stressed, and receiving high doses of NSAIDs. Omeprazole is currently the only medication that has been shown to significantly prevent formation of gastric ulcers and promote healing of existing ulcers in adult horses. Although evidence for its efficacy in preventing and treating NSAID-induced ulcers is lacking, omeprazole is still indicated when NSAIDs are used in stressed animals. In cattle, facilitated ankylosis is a reasonable alternative when the disease is too advanced, and it is a particularly good option for involvement of the DIJ. Articulations of the distal limb in general are well suited to facilitated ankylosis. In brief, the involved joint is opened and debrided of all debris, all infected tissue is curetted and removed, and a cast is applied and maintained until ankylosis is achieved.95 Alternatively, the digit may be amputated, although a reduced production life should be expected.96 ■ Prognosis In clinical studies, treatment is often limited by economic considerations, so the true long-term outcome of treatment is unknown. Outcome variables used in clinical studies range from discharge from the hospital to pasture soundness to racing potential. Owner expectations should be clear, keeping the animal's welfare in mind. The prognosis for septic arthritis should always be guarded, and owners should be informed of the high cost of treatment. In foals, factors that influence prognosis are systemic condition of the foal, number of joints involved, localization of joint involvement, severity of the infection, early versus delayed identification and institution of treatment, presence of osteomyelitis, and virulence of the organisms. In one study, 73 of 93 (78%) foals survived to discharge, but only a third reached racing perfor- mance.97 Isolation of Salmonella spp. and presence of multisystem diseases were negatively associated with survival and ability to race.97 A multidrug-resistant Enterococcus species was associated with unresponsive septic arthritis in three horses.98 In another study, 58 of 69 (84%) foals survived to discharge, although signs were present for less than 24 hours in 74% of foals, only 5 foals had more than one joint involved, and only 1 foal had osteomyelitis.99 This population of foals therefore appeared to be less severely affected. Of the affected foals, only 40.5% started in one race, and of the affected foals that were discharged, only 48.3% raced versus 66.2% in the control (sibling) group. This study concluded that even if foals are successfully discharged from the hospital, they are significantly less likely than their siblings to start in at least one race. Furthermore, these foals took significantly longer to appear on the track than their siblings. In another study of foals with osteomyelitis of hematogenous origin, 87 of 108 (80.6%) foals were discharged from the hospital, and 79 of 87 foals reached racing age.100 Overall, 52 of 108 (48%) foals raced. Of the 21 nonsurvivors, only 1 died; the other 20 were euthanized, but none was euthanized for economic reasons. Factors associated with nonsurvival in that study included foals less than 30 days of age, critical illness, multisystem disease, multiple bone lesions, lesions of the proximal phalanx, concurrent septic arthritis, multiple septic joints, and involvement of the coxofemoral, stifle, hock, or navicular bursa. In that study, the bacterial isolate involved had no significant effect on short-term outcome.100 In a study evaluating the factors associated with survival and racing performance in 423 neonatal Thoroughbred foals with bacteremia, the presence of septic arthritis increased the likelihood of nonsurvival by 4.54 times.101 In adults with open joint injuries, the prognosis can be favorable if the joint is contaminated but not yet infected and if aggressive treatment is started immediately. However, with established infection, the prognosis should always be guarded. In one study of horses with open joint injury, 53% of those examined within 24 hours developed septic arthritis, and overall survival was 65%. In horses presented within 2 to 7 days of injury, septic arthritis developed in 92%, and survival was 38.5%; in horses examined more than 7 days after injury, septic arthritis developed in all, and survival was 50%.13 In one study of 101 horses with heel bulb lacerations, those with involvement of synovial structures had worse outcomes than those that did not; 5 of 17 horses with synovial involvement were euthanized.16 Horses with contaminated or infected synovial structures treated by arthroscopic debridement appeared to have a better longterm outcome, with 106 of 118 (90%) surviving and 96 (81%) returning to previous use.16 In a study of horses with septic tenosynovitis, 40 of 51 (78%) horses were discharged, and 37 of 40 (73%) survived long term, with 21 (57%) returning to intended use.102 Surgical technique did not influence outcome in this study. One study reported on the use of matrix metalloproteases 2 (prommp2) and 9 (prommp9) and WBC count to monitor treatment and predict outcome in horses with septic arthritis.14 In that study, survivors had a significantly lower WBC count, prommp9, and ratio of prommp9/prommp2, with the latter being the best predictor for survival. In cattle the prognosis for septic arthritis is generally better than in horses, probably because of the lack of expectation for athletic use. Prognosis depends on time of presentation, degree of bone involvement, and degree of extracapsular ankylosis. In two studies the success rate was reported as 72% and 85%; cattle 103104 with septic tarsi had a worse prognosis.103,104 In another study, arthroscopic lavage and implantation of gentamicin-impregnated collagen sponges resulted in recovery in 12 of 14 cattle.105 After arthrodesis of the DIJ, 85% success was reported.96 For carpal arthrodesis, 87% success was reported if no carpal bone was removed, 72% success if one row of carpal bones was removed, and 35% success if both carpal rows were removed. Tarsal arthrodesis has a reported success rate of 87% in cattle.96 A recent study indicated a positive outcome in 55% (35 of 62) of calves affected with septic arthritis.20
More on the topic Septic (Infectious) Arthritis and Osteomyelitis:
-
Veterinarian -
|