Skin Diseases and Injuries ofthe Udder
Skin diseases that are frequently localized to the udder include bacterial folliculitis and contagious ecthyma (sore mouth). Readers should refer to Chapter 2 when additional information is desired or when signs are more general (e.g., capripox infection, bluetongue).
Contagious Ecthyma
Parapoxvirus infection may be limited to the teats or present elsewhere on the body. In regions where capripox virus also occurs, both viruses cause similar lesions on the udder and teats of lactating goats (Okoh and Obasaju 1983).
Pathogenesis and Clinical Signs
Contagious ecthyma (sore mouth) lesions predispose to mastitis by interfering with the function of the streak canal while simultaneously harboring many pathogenic bacteria. The virus also may interfere with local defense mechanisms, including macrophage function, in the udder (Spyrou and Valiakos 2015). A kid with sore mouth lesions can pass the infection to a doe's teats during suckling (Figure 14.4). Milking equipment and bedding contaminated by other infected does are other possible sources. The lesions are proliferative and crusty. Often they are secondarily infected with staphylococci.

Figure 14.4 Soremouth lesions on the teats of a doe that had been suckled by a kid with lip lesions. Source: Courtesy of Dr. M.C. Smith.

Figure 14.5 Pustules on the skin of the udder and moist dermatitis between the udder halves caused by Staphylococcus aureus infection. The doe later developed gangrenous mastitis due to S. aureus. Source: Courtesy of Dr. M.C. Smith.
Treatment and Prevention
Affected goats should be milked last, and an antiseptic udder salve may be applied to keep the scabs pliable and control bacterial proliferation until self-healing occurs.
The arguments for and against herd vaccination are discussed in Chapter 2. The zoonotic potential of the virus must not be forgotten.Staphylococcal Dermatitis
Lesions of the udder caused by staphylococcal infection include folliculitis, moist dermatitis in the intramammary sulcus, and deep furuncles.
Etiology
Staphylococcus aureus is the most important cause of folliculitis and furunculosis of the teats and udder skin of goats, but other staphylococci (Foster 2012) and streptococci may be involved.
Clinical Signs and Diagnosis
Pinhead- to pea-sized pustules typically develop on the skin on the back of the udder, base of the teat, or intramammary sulcus (Figure 14.5). Lesions are usually not painful. When a deeper furuncle develops, there is a reddened, warm, and tender swollen area that develops into an abscess (Fontanelli and Caparrini 1955; Heidrich and Renk 1967).
Cultures are rarely performed unless the condition is unresponsive to conventional therapy or spreads to other parts of the goat. Important differentials include contagious ecthyma, capripox, and warts when lesions are superficial; furuncles can be differentiated from milk cysts by careful palpation and, if necessary, aspiration. Enlarged or abscessed supramammary lymph nodes are located more dorsally than furuncles.
Therapy and Prevention
Lesions should be washed with a mild disinfectant and dried with single-service towels. Disinfectant ointment or spray is applied after milking. Affected animals are to be milked last, and the milker should wear gloves or wash hands to avoid spread to other goats. Furuncles can be encouraged to point with ointments containing iodine or ichthyol. The abscess is then lanced and flushed. Autogenous S. aureus vaccine (two doses) has appeared to limit the course and spread of the disease in some goat herds (Heidrich and Renk 1967). Careful attention to milking hygiene and maintaining a dry environment are probably more effective than vaccination.
Nodular Tubercular Thelitis
A large machine-milked dairy goat herd in France experienced an outbreak of skin lesions on the lower udder and upper teat that affected approximately 100 mature goats over the course of several years (Chartier et al. 2016). Circular indurated erythematous areas progressed to dark raised crusts over ulcerative plaques. Some animals had enlarged mammary lymph nodes, but milk production was not affected and the lesions eventually healed. Histology revealed tuberculoid granulomas with Langhan's-type multinucleated giant cells and caseous necrosis; polymerase chain reaction (PCR) techniques demonstrated the presence of non-culturable bacteria closely related to Mycobacterium leprae and Mycobacterium Iepromatosis. The source of the infection was not identified.
Caseous Lymphadenitis
In herds in which Corynebacterium pseudotuberculosis is endemic, wounds to the teats or udder permit penetration of the organism. Infection of the wound may be noted, but more commonly, the problem first becomes obvious when an abscess develops in a supramammary lymph node (Figure 14.6). This abscess may break and drain pus down the back of the udder, or additional enlarged nodes may appear in a chain that extends upward toward the vulva. Caseous lymphadenitis is discussed in detail in Chapter 3.
Dermatomycosis
Flat, slightly thickened, circular, non-painful skin lesions on the udders of goats in Florida have been diagnosed as tinea versicolor, a dermatomycosis of humans resulting from Malassezia furfur (Bliss 1984). Lesions on dark skin appeared depigmented, whereas on lightly pigmented skin they were lightly colored. Biopsy specimens contained basophilic, periodic acid-Schiff (PAS) stain-positive filamentous organisms and oval, thick-walled cells (nicknamed “spaghetti and meatballs”) in the stratum corneum. No treatment was attempted in these animals, but topical antifungal treatments have been used to treat Malassezia
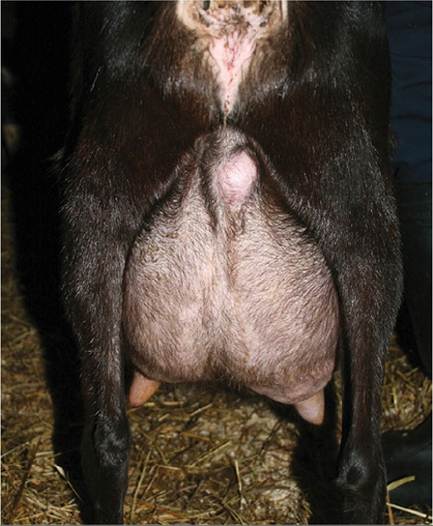
Figure 14.6 Abscess in the supramammary lymph node of a doe in a herd with endemic caseous lymphadenitis.
Source: Courtesy of Dr. M.C. Smith.infections elsewhere on the skin of goats (Eguchi-Coe et al. 2011).
Frostbite
If the teats are wet from inadequate drying after udder preparation for milking or from confinement in a wet environment, frostbite may occur when the goat is exposed to extreme cold and wind. Pendulous or edematous udders are especially vulnerable. Mildly chapped teats may be treated with protective ointments. If the full thickness of a teat is frozen, thawing in warm water at 41-44 °C (106-111 °F) and protecting from refreezing are advised (Scott 1988). Sloughing of skin on the teat and secondary bacterial mastitis are to be expected. Powder teat dips are available for dipping in cold weather after milking.
Sunburn
Does with light-colored udder and teat skin are subject to sunburn when first turned out in the spring, even with cloud cover. The best means of avoiding a painful burn is to initially permit only very brief grazing, then drive the animal back into the barn. With succeeding days the exposure to sunlight is gradually lengthened. This protocol also avoids indigestion in goats changing from dry hay to green grass. Many owners lack time, patience, or both. Their animals can be protected by application of colored teat dip or a sunscreen sold for human use. All such material must be washed off before the next milking to avoid contamination of the milk. Primary or secondary photosensitization (see Chapter 2) should be ruled out.
Saanen does that have pale pink udders at the end of the housing season often have large black spots akin to freckles on the udder after a summer on pasture. This condition is not pathologic and requires no treatment.
Warts and Squamous Cell Carcinomas
Papillomas (warts) of the udder of white goats are a very serious problem, especially in areas with abundant sunshine (Moulton 1954; Ficken et al. 1983; Theilen et al. 1985).
Etiology and Epidemiology
Most attempts to demonstrate virus in these lesions have failed.
Recently, papillomavirus-like sequences have been detected in wart-like lesions by DNA hybridization, even though no virions were found by electron microscopy (Manni et al. 1998), and a novel papillomavirus was identified in teat lesions from another goat using PCR techniques (Dogan et al. 2018). An epidemiologic survey (Ficken et al. 1983) revealed that appearance of udder warts in the herd often begins three to six months after introduction of an affected goat. Exposure to sunlight appears to be involved.Pathogenesis and Clinical Signs
The warts are multiple and initially may be flat and scaly (Figure 14.7) or prolonged into cutaneous horns. Some flake off the teat or bleed during milking. In some animals the warts regress completely during the non-lactation period. In other goats, the warts partially or totally regress, but recur the next spring and summer (during lactation). The animals with persistent lesions may develop squamous cell carcinomas in subsequent years. The carcinomas have a flat base and often an ulcerated surface. They occasionally metastasize to the supramammary node. Much more serious is their propensity to eventually erode through the wall of the teat. This leads to mastitis and loss of the udder half, as may penetration of the streak canal by bacteria harbored in tumors located near the teat orifice. Myiasis may also occur.
Treatment and Prevention
No effective treatment is known. Neither have vaccines been of any value. The recently affected goat could be housed in the hopes that permanent regression will occur. Certain carcinomas may be surgically removed; cryosurgery has the advantage of minimizing hemorrhage. Prevention involves excluding affected goats from the herd and selecting for other breeds, or at least for pigmentation of the skin of the udder in white breeds. The prevalence of udder warts in Saanens in Queensland, Australia, has been greatly decreased by selecting for tan skin on the udder (Baxendell 1984a).
In South Africa, providing adequate
Figure 14.7 Udder warts on a Saanen doe. Source: Courtesy of Dr. M.C. Smith.
shade for milking Saanens has prevented the development of squamous cell carcinomas (Donkin and Boyazoglu 2004).
Teat Obstruction and Stenosis
A doe at kidding may have a temporary teat obstruction caused by a plug blocking the streak canal. This material can be manually expressed from the teat, and afterward the doe milks easily. When kids are allowed to suckle the doe, it is important to remove a squirt or two of colostrum from each half of the udder. Not only does this allow inspection of the secretion for evidence of clinical mastitis, but it avoids starvation of the kid that is too weak to suck out the teat seal on its own. Even a strong kid prefers to suckle the side that yields milk for less effort. The unmilked side then becomes distended and painful, and the doe no longer permits nursing on that teat. Stripping out milk from the enlarged gland as soon as the udder is noticed to be lopsided is necessary if both glands are to remain productive in the current lactation.
If difficulty in milking persists after removal of the initial teat plug, an experienced person should evaluate the teats of the goat in question. People who are just learning to hand-milk goats may have difficulties because of lack of proper technique. If a teat sphincter is too tight for milking, it is important to determine if scar tissue from a previous injury is responsible. Ultrasound examination of the teat will aid in this determination (see above under normal anatomy) or endoscopy could be used if available. If no scar tissue is detected, the doe and its offspring should not be kept for breeding purposes. In such an animal and in goats that previously milked normally, a stenotic teat opening sometimes can be corrected by removing a core of tissue with a disposable 18-gauge needle (Nigam and Tyagi 1973) after previous infusion or spraying of local anesthetic. Consideration should be given to antibiotic therapy after such manipulation because the protective keratin lining of the streak canal will undoubtedly be damaged. In large teats with scar tissue or an excessively tight sphincter, several cuts (on opposite sides, with care to avoid incising skin) with a teat bistoury may be tried; milk should drip from the teat end immediately after surgery, as some contraction is to be expected during healing.
If the udder of a multiparous doe appears to be distended but no milk reaches the teat cistern, the problem may be scar tissue at the base of the teat (Figure 14.8). This develops as the result of chewing behavior by hungry nursing kids when milk production is inadequate. The obstruction may not be recognized until the subsequent lactation. An important differential is hard udder, in which interstitial mastitis caused by the CAE virus (see below) prevents milk from reaching the teat end.

Figure 14.8 Scars on the caudal aspect of the teats of a Boer doe caused by aggressive nursing by hungry kids in the previous lactation. Source: Courtesy of Dr. M.C. Smith.
Milkstones, Iactoliths, or “peas,” small hard concretions floating in the teat cistern, may occasionally work as a ball valve and interfere with milking. An association with incomplete milkout has been proposed (Guss 1980), but the possibility that a staphylococcal infection provided the nidus for the lactolith should not be ignored, and milk culture is warranted. Stones that cannot be forcibly expressed from the teat or crushed with alligator forceps could be removed surgically (Plummer and Plummer 2012).
Udder and Teat Wounds
Udders with poor suspensory ligaments or long teats can be injured during grazing activities. Barbed wire, dog attacks, and horn punctures can also tear the skin of the teats or udder. Repair of the wound follows general surgical principles, but has been described in some detail by Anderson et al. (2002). After cleansing and debriding to bleeding tissue, the fascial layer of the udder or the inner teat lining (depending on the location of the wound) is closed with a fine (4-0) absorbable suture material. Non-absorbable sutures or wound clips can be placed in the skin. Others prefer a three-layer closer (Plummer and Plummer 2012). The goat is given systemic antibiotics (penicillin) and the gland is infused with a bovine intramammary antibiotic product. Tetanus prophylaxis must not be neglected. Aftercare involves frequent gentle hand-milking or, preferably, drainage with a sterile teat cannula to prevent back pressure, leakage, and formation of a permanent fistula.
In fiber-producing goats, teats are occasionally cut off accidentally during shearing. Does with only one teat remaining may not be able to raise a kid under range conditions.
Teat biting is an abnormal behavior that has been observed in dairy goats at the time of estrus if the group is being reserved for later breeding. The teat may be scratched or bruised or bitten completely off. Often the goat that is biting the teats of other animals is not identified, but sometimes it is a frustrated buck, sticking his head through a fence to a waiting doe. The use of a sexually active vasecto- mized buck has been recommended to prevent this problem (Coleshaw 2004). The does will not feel compelled to search out a buck and heat detection will also be possible without penning the does within reach of another buck.
Udder Edema
Periparturient udder edema, characterized by excessive accumulation of fluid in the interstitial spaces and pitting on digital pressure of the skin of the udder, has been reported in goats, but has received little scientific attention. The goat may be uncomfortable and difficult to milk. Does kidding for the first time are frequently affected. Differential diagnosis includes mastitis, hard udder caused by CAE, hematoma, and rupture of the prepubic tendon (Al-Ani and Vestweber 1983). Treatment with exercise, massage, and a diuretic (e.g., 50-100 mg furosemide, although a goat dosage has not been established) can be tried, but the edema often resolves within a few days after parturition without any treatment except milking. Vitamin D3 has been suggested to aid resolution of udder edema by counteracting hypocalcemic effects of hypomagnesemia (Mills 1983a, b). Some owners start milking a week before parturition as a means of controlling edema (Baxendell 1984b); the first milking colostrum should be heat treated and frozen for later feeding to the kids. Draining the fluid with one or more 3 cm incisions in the skin caudal to the teat has been reported to be effective and innocuous in goats (Rebesko et al. 1974), but is not presently recommended. Because the pathogenesis of udder edema remains unclear, even in cattle (Al-Ani and Vestweber 1986; Goff 2006), one can only speculate on how to prevent the condition in goats. Limiting salt before parturition is reasonable, but limiting grain, as commonly recommended, might cause pregnancy toxemia.