Skin Disorders of Unknown or Genetic Origin
Stephen D. White
Equine Seborrhea
Several possibly related equine skin diseases characterized by scaling and crust formation are referred to as seborrhea. Contrary to claims in the older literature, there is little evidence that seborrhea is related to excess sebum production by the sebaceous glands.
Most types of seborrhea are probably diseases of abnormal cornification (development of the stratum corneum). Further, most cases reported as “generalized seborrhea” in the horse were probably pemphigus foliaceus, equine sarcoidosis (chronic granulomatous disease), or some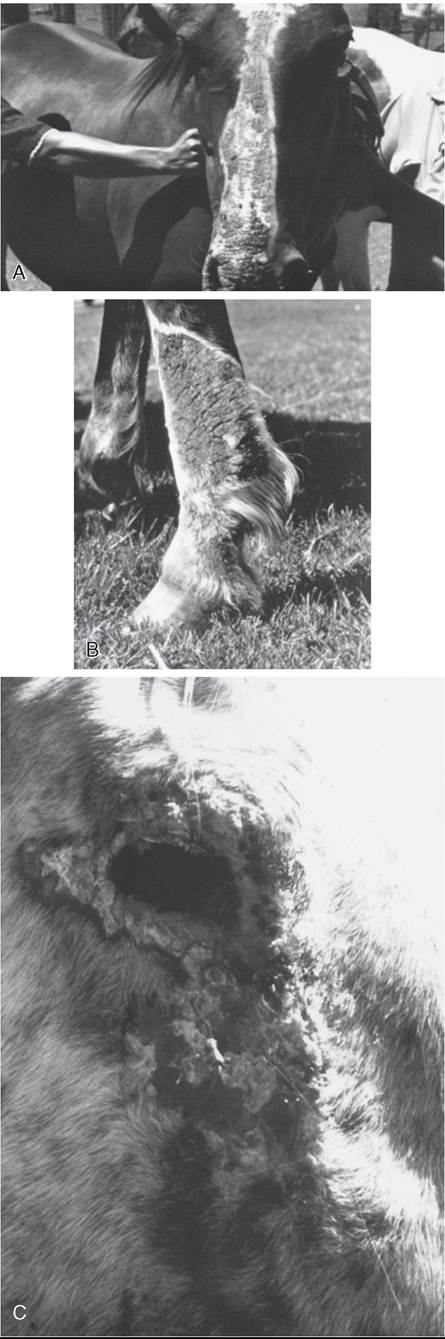
FIG. 40.15 Photosensitization. A, White blaze of a horse is selectively affected. B, White stocking of a horse is selectively affected. C, Area around eye where hair is less dense is most severely affected.
other immune-mediated or autoimmune disease. Mane and tail seborrhea is typified by moderate to heavy scaling, with minimal or no pruritus. Some horses have considerable alopecia of the tail.
Cannon keratosis is a common equine skin condition. It involves the cranial surface of the rear cannon bone region and rarely the forelimbs. The lesions consist of areas of scaling and crusting with varying degrees of alopecia. There is no pruritus or other signs of inflammation. Cannon keratosis occurs in both males and mares, so there is no basis for the theory that the condition is caused by urine splatter (“stud crud”).1 In one recent report, the response to treatment with four topical preparations was evaluated in an 11-year-old Morgan horse mare with histologically confirmed quadrilateral cannon hyperkeratosis. Each limb was treated for 30 days, and response to treatment was evaluated both histologically and visually. A water-based emollient and 0.1% tacrolimus ointment produced encouraging clinical responses.2
Linear Keratosis and Linear Alopecia
Linear keratosis and linear alopecia are rare equine dermatoses of unknown cause.
There is one report in a cow.3 Lesions do not follow blood or lymphatic vessels, nerves, or dermatomes. Because these conditions coexist in some horses, it has been suggested that they are variations of the same abnormality, and we have seen one case where both histologic presentations were simultaneously present in the same clinical lesion. Both conditions have been seen in a wide variety of breeds, but Quarter Horses appear to be predisposed. Most horses develop lesions between 6 months and 5 years of age.Linear alopecia is characterized by gradual development of annular areas of alopecia, usually in a linear, vertically oriented configuration. One or more linear areas may be present. The lesions are usually 2 to 10 mm wide by a few centimeters to more than 1 m in length and occur on the neck, shoulder, and lateral thorax. Mild surface scale and crust may be present. Lesions are neither painful nor pruritic. Affected horses are typically otherwise healthy.
Linear keratosis is characterized by the gradual asymptomatic occurrence of one or more unilateral, linear, vertically oriented bands of hyperkeratotic papules that progress to marked hyperkeratosis and alopecia. We have seen one case where the lesions were confined unilaterally to the jugular furrow (Color Plate 40.10). Lesions vary from 0.25 to 3.5 cm in width by 5 to 70 cm in length and occur most often over the neck, shoulder, and lateral thorax. Lesions have also been reported to involve the legs, hip, and pectoral region. Again, affected horses are typically otherwise healthy.
These disorders are visually distinctive. Histopathologic findings in linear alopecia include early lymphocytic, infiltrative mural folliculitis and later granulomatous, infiltrative mural folliculitis. The mural infiltrate is often directed at the middle area (isthmus) of the follicle. Sebaceous glands may be involved in some cases, and complete follicular destruction and permanent alopecia are seen in severe chronic lesions.
Histopathologic findings in linear keratosis include irregular to papillated epidermal hyperplasia and marked compact orthokeratotic hyperkeratosis.4 We have seen one horse with lesions grossly diagnosed as linear keratosis, whereas the histopathology had features of both conditions.Neither condition is known to undergo spontaneous resolution. Owners should be advised of the potential hereditary nature of these disorders. Linear alopecia has been anecdotally reported to respond to topical or systemic glucocorticoids, but recurrence is likely. Response to therapy is more likely to be seen in early lesions, when complete destruction of hair follicles has not occurred. Linear keratosis responds poorly to treatment. Topical keratolytic and keratoplastic agents, such as sulfur/
salicylic acid-containing shampoos or 50% propylene glycol, can reduce the hyperkeratosis but must be continued for life. There has been some success using tacrolimus (Protopic 0.1% ointment [Astellas Pharma US, Northbrook, Ill.]), a drug similar to cyclosporine but better absorbed through the skin, once or twice daily. Because neither condition is symptomatic, observation without treatment may be an acceptable approach. Interestingly, a report exists of a familial incidence of linear epidermal nevi in Belgian horses.5
Albinism
Complete and partial albinism occurs in cattle, sheep, and horses. It is a genetic defect (probably autosomal recessive) in melanin synthesis, resulting in white skin, white hair, pink eyes, and photophobia. In horses, albinism must be distinguished from lethal white syndrome, which is primarily a problem in Paint horses (especially, but not exclusively, in overo breedings). The defective gene has also been found in American Miniature horses, half-Arabians, Thoroughbreds, and cropout Quarter Horses (foals born to registered Quarter Horses that have too much white to register with the American Quarter Horse Association [AQHA]).6 The Veterinary Genetics Laboratory at UCD offers a diagnostic test to determine carrier status (https://www.vgl.ucdavis.edu/services/horse.php).
The lethality of albinism in horses comes from the association with intestinal aganglionosis. The foals die shortly after birth. Because some white foals are not affected, euthanasia should be performed only after signs of intestinal malfunction occur. This disease is similar to Hirschsprung’s disease in humans and is linked to a mutation in the endothelin-B receptor gene.7
Juvenile Arabian Leukoderma (Arabian Fading Syndrome, Pinky Syndrome, Hereditary Vitiligo)
Loss of melanin in the skin (depigmentation) occurs in young Arabian horses 6 months to 2 years of age (Fig. 40.16, A). The areas most frequently affected are periocular tissues, muzzle, genitalia, anus, perineum, inguinal region, and undersurface of the base of the tail. Depigmentation may persist, repigment, or wax and wane. The condition is probably hereditary.1
Vitiligo
This condition is best defined as “idiopathic depigmentation.” Typically no trauma has occurred to produce the loss of pigment, and other skin structures are not affected (i.e., no scarring or alopecia) (Fig. 40.16, B,- Color Plate 40.11). There is no known treatment for vitiligo. The condition may be seen in any species but is perhaps best recognized in the horse.
Reticulated and Hyperesthetic Leukotrichia
Reticulated Ieukotrichia occurs mainly in Quarter Horses, usually as yearlings, and occasionally in other breeds. The lesions occur on the dorsal midline and consist initially of linear crusts arranged in a characteristic crosshatch pattern (Fig. 40.17). The crusts shed, alopecia occurs, and white hair grows in permanently. There is leukotrichia without leukoderma (depigmented skin). Histologically, these lesions may resemble an epidermal form of erythema multiforme, resulting in individual keratinocyte necrosis. Hyperesthetic Ieukotrichia is a similar disease clinically, except that the crusts are extremely painful to the touch. Within a few weeks, white hairs appear in the affected areas. The crusts resolve, and the pain subsides in 1 to 3 months, but the leukotrichia persists.
While anectodal cases have been linked to recent rhinopneumonitis vaccination, a recent report of a case series failed to find evidence of a link to any vaccine or medication and determined that the histology differed somewhat from erythema multiforme.8 These diseases may recur (sometimes on a seasonal basis), and there is no known effective treatment.Hereditary Equine Regional Dermal Asthenia (Hyperelastosis Cutis)
Hereditary equine regional dermal asthenia (HERDA) occurs early in life in horses. Most affected horses are Quarter Horses, but registered Paint horses and Appaloosas with Quarter Horse lineage have developed this disease.9,10 Many of the Quarter Horses are from high-quality cutting lines. Reported cases have been in North America, but the disease and its associated genetic defect have been reported in Europe and South America.11-14 The disease (or similar condition) has also been reported in a crossbred Arabian mare, a Thoroughbred gelding, a Hanoverian foal, and a Hafflinger horse.15-18 Rarely, a similar disease has been noted in cattle, termed dermatosporaxis; this is caused by mutations in the procollagen I N-proteinase gene.17,19-21
The working hypothesis for HERDA in horses is a defect in the structure or healing process of the collagen fibers in the middle to deep dermis. Affected horses have less cutaneous tensile strength than healthy horses.22 Typically these areas are over the back and sides of the neck (Fig. 40.18). The skin in these areas may be easily torn or stretched and often develops seromas and hematomas (“blisters” filled with either serum or blood). Healing is usually adequate but often leaves unsightly
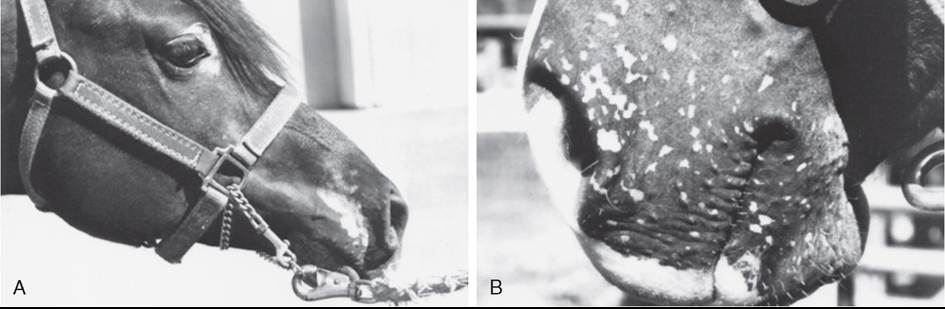
FIG. 40.16 A, Juvenile Arabian leukoderma. B, Vitiligo in a horse. (Courtesy Dr. Anthony Stannard.)
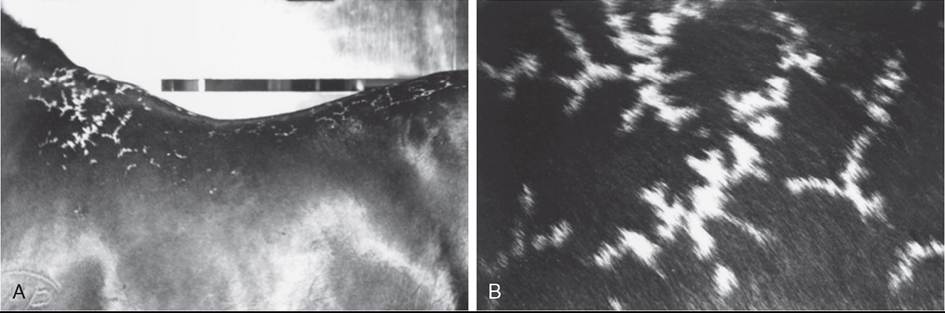
FIG.
40.17 Reticulated Ieukotrichia in a yearling Quarter Horse. A, Note reticulated pattern of white hairs over dorsum. B, Close up view of reticulated pattern of white hairs (leukotrichia). (Courtesy Dr. Anthony Stannard.)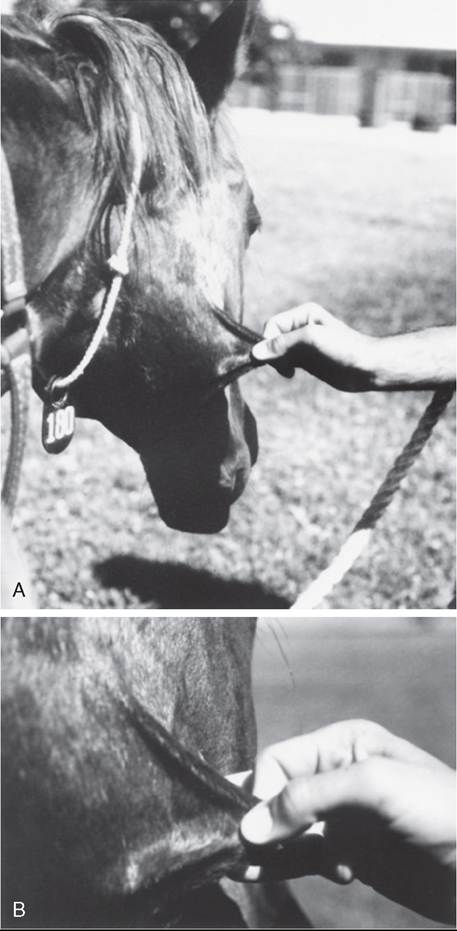
FIG. 40.18 A, Hereditary equine regional dermal asthenia (HERDA, hyperelastosis cutis) in a horse, showing hyperextensible skin. B, Close-up of A. (Courtesy Dr Anthony Stannard.)
scars. Despite the regional pattern of the cutaneous signs, skin with decreased thickness was not regionally distributed in the HERDA-affected horses in one report.23 Diagnosis is often based on the clinical signs alone; histologic findings are sometimes subtle, but “clumped” or poorly organized collagen fibers below the level of the hair follicles may be seen. A zone of middermal to deep dermal separation has been reported in two horses and is present in some biopsy samples.10,24 Poorly oriented collagen fibers are sometimes seen on electron microscopy. Interestingly, affected horses may have decreased corneal thickness, increased tear production, and increased incidence of corneal ulcers, as well as loss of heart valve tensile strength.25,26
This condition is almost certainly present at birth, but HERDA is often not noticed until about 2 years of age, when horses start being trained with tack and saddle, and the resulting friction and trauma induce the typical lesions.27 As with many genetic diseases, no effective treatment or cure exists; some of these horses have been maintained as “pasture pets.”
This disease follows an autosomal recessive mode of inheritance, so for the foal to be affected, both the sire and the dam must carry the gene, and if they were bred again, there would be about a 25% chance that the next foal would also be affected.28 Although histopathologic evaluation is informative, it is not conclusive for establishing the diagnosis. Samples of skin from the neck, croup, or back are useful for diagnosis of HERDA.23 However, the final diagnosis must be confirmed using molecular testing.23,29
Recently a genetic marker was determined for this disease.29 The marker relates to a missense mutation in equine cyclophilin B (PPIB), which in recent work has been shown to cause a functional defect in this protein, resulting in less effective catalysis of the rate-limiting step in collagen folding.30 The Veterinary Genetics Laboratory at UCD offers a diagnostic test to determine carrier or affected status (http://www.vgl.ucdavis.edu/services/horse.php). Both carriers and clinically affected horses with HERDA should be removed from breeding programs. There is no known treatment.
Epidermolysis Bullosa
Epidermolysis bullosa (EB) includes a number of diseases typified in humans and animals by the common finding of blister formation after minor trauma. Most forms are congenital and apparent soon after birth. In animals and humans, subsets of EB are classified by the histologic location of the blister or cleft. These subtypes (and respective cleft location) are termed EB simplex (basal cell layer of epidermis), junctional EB (intralamina lucida or basal cell layer), and dystrophic EB (sublamina densa).
Junctional EB has been reported in Belgian foals of both genders; in other breeds; and in a donkey, sheep, and cattle.31-38 Lesions are usually noted within 3 days of birth and include multiple asymmetric skin erosions and ulcers, often encrusted. Lesions may be especially prominent around the coronary bands (causing the hoof to crack and slough) and on the oral, anal, and genital mucosa. Histology and ultrastructural findings indicate a cleft in the intralamina lucida of the basement membrane zone. This is presumably caused by a defect in the anchoring filaments that connect the basement membrane to filaments in the superficial dermis.32 A laminin-5 (laminin 3A32) defect has been demonstrated in Belgians and in two French draft breeds, Trait Breton and Trait Comtois; the mutation is a cytosine insertion in exon 10 of the LAMC2 gene.39-41 Because of this knowledge, the Veterinary Genetics Laboratory at UCD offers a diagnostic test to determine carrier status in Belgian draft horses and related breeds (http://www.vgl.ucdavis.edu/services/horse.php). The defect in some ruminants has also been noted to be associated with the LAM gene.
Clinical presentation and the age of the foal are highly suggestive of EB diagnosis. Histology and, ideally, electron microscopy are required to confirm the diagnosis. There is no known treatment, and affected horses as well as the sires and dams of affected horses should not be bred; the mode of inheritance is autosomal recessive.
The disease previously known as Cpitheliogenesis imperfecta in Saddlebreds is now recognized as junctional epidermolysis bullosa. Lesions are most common on the limbs, head, and tongue. Hooves may slough in severe cases. Clinical presentation is usually diagnostic.42-45 In moderately to severely affected animals, the disease is fatal within a few days; the foals die of septicemia or other developmental abnormalities. Mildly affected areas may heal by scar formation.
Ruminants
Epidermolysis bullosa has been reported in cattle and sheep. The simplex form has been reported in Angus and Friesian- Jersey crossbred cattle (in the latter, a keratin 5 defect was noted), junctional EB in a Charolais calf (deficient expression of an epidermal integrin), and dystrophic EB in Brangus calves.46-49 In sheep, dystrophic EB in the white Alpine, Assaf, Suffolk, South Dorsett Down, and black face Scottish breeds has been shown or theorized to involve mutations in the gene encoding for collagen VII.50-53 Junctional EB has been described in German black-headed mutton sheep and churra sheep, with the defect in the former traced to the formation of laminin 332, similar to the defect in the Belgian horses.54,55 Junctional EB has also been described in Charolais, Belgian Blue, and Danish Hereford cattle; the defect in the latter two is also tied to the laminin gene.56-58 Clinical signs of EB in ruminants are similar to those seen in horses, with ulcers, especially around the coronary band and in the oral cavity.
Eosinophilic Granuloma (Nodular Necrobiosis, Collagenolytic Granuloma)
Eosinophilic granuloma is the most common equine nontumor nodular disease in our practice. In most cases the etiology is unknown, although a hypersensitivity reaction to insect bites has been suggested. There is no apparent age, breed, or gender predilection. The disease often begins in warmer months. Lesions up to 5 cm (2 inches) in diameter may be single or multiple and most often affect the neck, withers, and back (Fig. 40.19). Skin biopsy reveals multifocal areas of abnormal- staining collagen surrounded by granulomatous inflammation containing eosinophils, lymphocytes, and histiocytes.1 This is not thought to be caused by degeneration, but rather by

FIG. 40.19 Eosinophilic granuloma (nodular necrobiosis) with dermal nodules on a horse’s withers. (Courtesy Dr Anthony Stannard.)
degranulation of eosinophils and the coating of normal collagen fibers with the degranulated material.59
Development of equine eosinophilic granuloma has been noted in areas of previous injections using standard silicone- coated, stainless steel hypodermic needles.60 The reaction may occur at sites of IV and IM injections. Lesions consist of nonpainful cool, raised papules or nodules 0.25 to 1 cm in diameter at sites of previous injection. The nodule appears 24 to 48 hours after the injection, and the subsequent eosinophilic granuloma can persist for months to years. Affected horses do not develop a lesion at the site of injection if nondisposable, noncoated needles are used. The use of the noncoated needles is recommended for any horse that develops injection-site collagenolytic granulomas.
Horses with solitary or a few lesions may be treated by surgical excision (not in the saddle area) or glucocorticoid injections under the lesions. Triamcinolone acetonide (3 to 5 mg per lesion) is effective. It has been recommended that no more than 20 mg triamcinolone acetonide be administered at once to any horse because any more of this drug may cause laminitis.1 Horses with multiple lesions may be treated with oral prednisolone at 1 mg/kg once daily for 2 to 3 weeks. Multiple small (and disability of the limbs. Inevitably, it leads to the horse's premature death. In the Belgian draft horse, it has reduced the average life expectancy of a stallion from 20 to only 6 years.
The pathologic changes and clinical signs closely resemble a condition known in humans as chronic lymphedema or elephantiasis nostras verrucosa. The lower leg swelling is caused by abnormal functioning of the lymphatic system in the skin, which results in chronic lymphedema (swelling), fibrosis, a compromised immune system, and subsequent secondary infections of the skin. Based on preliminary research, it appears that a similar pathogenic mechanism is involved in the disease that affects these specific draft horse breeds.
The clinical signs of this disease are highly variable. The earliest lesions are characterized by skin thickening and crusting; both are often visible only after clipping the long feathering. Secondary infections develop very easily in these horses' legs and usually consist of either chorioptic mange or bacterial infections. Both dark skin and white skin on the lower legs are equally affected. These lesions are consistent with pastern dermatitis, certainly seen in other breeds. In horses with CPL, however, these lesions do not respond well to therapy.
As the disease progresses, one or two thick skin folds and sometimes multiple small, well-demarcated ulcerations develop, predominantly in the rear of the pastern region. The ulcerations are covered with adherent crusts. Manual removal of the crusts or even movement during exercise results in bleeding. These small sores may seem to respond initially to various topical medications but often reverse course, only to progress in severity and multiply in number. Small lesions tend to coalesce into larger and more intractable (resistant to treatment) areas of skin ulceration. Over time, the lesions extend up the leg, often affecting the skin as high as the knees or hocks. These lesions are, at the very least, irritating to the horses and at times can be quite painful. Severely affected individuals often exhibit generalized swelling in all four legs.
This condition is therefore primarily a lymph system disease, and the pastern dermatitis in these draft horses is secondary to the body's inability to supply fluids properly and oxygenate the skin of the lower leg. The lymphatics break down over time, and the protein-rich fluid leaks into the tissues of the lower leg, which results in fibrosis of the tissues under the skin and thickening of the skin itself. The tissue fibrosis leads to even more blockage of fluid within the legs, inhibiting circulatory flow. This results in neovascularization, a process by which the body develops new blood vessels in a futile attempt to provide oxygen to its tissues.
Researchers suspect that a deficiency or abnormality in the connective tissue component known as elastin is the underlying factor and perhaps the cause of the lymphatic degeneration in these horses.74,75 In affected animals, the lymph vessels and deep tissues of the skin do not have sufficient amounts or the proper configuration of elastin. The lack of this critical tissue element apparently instigates the progression of disease and the chronic progression of clinical signs. One report documents high levels of antielastin antibodies in affected horses.76 A more recent report found that affected horses had increased amounts of dermal elastin in both the distal limb and the neck, whereas unaffected horses of a susceptible breed had decreased amounts. These findings support an earlier hypothesis that CPL of horses is a generalized disease. Reduced efficiency of the elastic network in supporting the dermal lymphatics may explain the development of CPL.77
As the condition becomes more chronic, the lower leg enlargement becomes permanent, and the swelling is firm on palpation. More of the thick skin folds and large, poorly defined, firm nodules develop. The nodules may become quite large and often are described as golf ball or even baseball sized. Both skin folds and nodules first develop in the back of the pastern area. With progression, they may extend and encircle the entire lower leg. The nodules become a mechanical problem because they interfere with free movement and are frequently injured during exercise. This disease often progresses to include massive secondary infections that produce copious amounts of foul-smelling exudates, generalized illness, debilitation, and even death.75,76
In one report of possibly the same condition in several draft breeds, the authors found a perivascular dermatitis dominated by T lymphocytes with an increase in major histocompatibility complex (MHC) class !!-positive, dendritic-like cells. Immunohistochemical labeling for cytokeratins CK5∕6(4), CK10, and CK14 indicated a change in their expression pattern. This correlated with the degree of epidermal hyperplasia, indicating abnormal differentiation of keratinocytes. There was a statistically significant correlation between the severity of skin lesions and several other factors, including increasing age, increasing cannon circumference, prominence of anatomic structures (e.g., fetlock tufts of hairs, ergots, chestnuts), and bulges in the fetlock region.78 Another more recent report, again looking at various draft breeds (Rhenish German, Schleswig, Saxon-Thuringian, and South German), identified a quantitative trait loci for CPL.79
Zinc Responsive Dermatitis
In Holstein-Friesian cattle, zinc responsive dermatitis is a hereditary autosomal recessive defect in GI zinc absorption, also known as lethal trait A 46, and is characterized by diarrhea, skin lesions, poliosis (gray hairs), and a decreased suckle reflex. Skin lesions involve inflammation and crusts around the eyes, base of ears, coronary bands, and muzzle; these may become generalized. Plasma zinc concentrations of calves are normal at birth. The histology of skin lesions shows parakeratosis.80
Oral administration of zinc reverses signs in 1 to 3 weeks.
Recently a similar disease, albeit one associated with a different mutation, was described in Fleckvieh cattle. Treatment is uncertain, as the mutation does not appear to involve a problem with intestinal transport of the zinc.81
In goats and sheep this may be caused by ingestion of alfalfa (which is high in calcium and therefore blocks zinc uptake) or overliming the soil with calcium salts, creating a zinc-deficient soil. Crusts, bilateral symmetrical alopecia, rough hair coat, abnormal claw growth with weight loss, stunted growth, abnormal (kyphotic) gait, and anorexia may all be seen.82 Histopathology of skin shows parakeratosis and hyperkeratosis; this may be hereditary in some dairy goats.83