Squamous Cell Carcinoma
Stephen D. White
Squamous cell carcinomas (SCCs) are tumors composed of squamous epithelial cells. They occur in all domestic species and are the most common bovine ocular tumor (see Chapter 39) and the second most common tumor recognized in the horse.
Although their gross appearance may vary, these tumors are usually slightly raised, broad based, and white to pink and have a cobbled or cauliflower-like surface (Color Plate 40.9). SCCs frequently occur on the penis and sheath of aged stallions and geldings (see Chapter 43). They also occur on the lips, nose, eyelids, eyes, and ears of horses. SCC often accompanies cutaneous papillomas of the udder and teats in Saanen milk goats, as well as female Angora goats in South Africa. The ears, base of the horns, perineal region, and prepuce may also be affected.2,3 SCC is reported as the most common cancer of the ear of sheep; an outbreak primarily affecting the eyelids in 15% to 18% of a sheep population has been reported. Diagnosis is by biopsy. There is increasing evidence that SCC in horses and sheep is associated with papillomavirus infection.5-8The treatment of choice is wide surgical excision.2,9,10 Solar elastosis (aggregates of thick, wavy, interwoven elastic fibers mixed with areas of degenerated collagen), when seen histologically with SCC, may lend a more favorable prognosis after complete surgical removal of lesions.11 Other treatment modalities reported as successful include cryosurgery, radiofrequency hyperthermia, and radiation therapy.2,12 Another study showed that topical application of 5-fluorouracil (5-FU) and intralesional cisplatin were effective in horses with SCC.13-16 Piroxicam was successful in the long-term control of SCC with metastases in one horse.17
Equine Sarcoid transmission studies of sarcoids have been unsuccessful.
Inoculation of sarcoid cell-free extract in cows does not induce warts, nor does it induce sarcoids in unaffected horses.3 Experimental cutaneous infection with BPV induces Abropapillomas that are clinically similar to sarcoids. The lesions, however, regress spontaneously with production of neutralizing antibodies to the virus and presence of viral DNA sequences in white blood cells.24,25 In contrast, histologically confirmed, naturally occurring sarcoids do not regress and are not associated with detectable serum antibody responses to BPV.26The infection in horses is considered nonproductive because BPV cannot replicate in horses nor be serially passaged from BPV-induced fibropapillomas.17,25 Full viral life cycle has never been demonstrated in Equidae, and viral particles have never been detected in lesions. Hence the disease is currently accepted as the result of an abortive cycle, dead-end infection where only early BPV gene sequences persist episomally27,28 or are integrated in host DNA.29
The mode of transmission of the disease is unknown and does not require contact with cows. Intradermal injection of primary sarcoid fibroblasts containing viral episomes,24 naked full-length BPV1 genome,24 or transforming genes (E5 and E7)30 does not induce sarcoids in horses and donkeys. Supporting evidence for an equine-to-equine infectious cycle that maintains BPV without the need for bovine host is missing. The finding that the majority of sarcoids collected in Austria, Switzerland, the United Kingdom, and Poland harbored equid-specific BPV1 variants, and that bovines lack these variants,31-35 further strengthens the theory that BPV is not transmitted from bovines. This is confirmed by a study where BPV DNA sequences were detected in healthy skin of horses not known to have ever been in contact with bovines.36
An epidemiologic BPV DNA analysis of a sarcoid outbreak in donkeys and mules in a rescue sanctuary revealed that donkeys were not the victims of an epidemic but had accidently developed sarcoids associated with different BPV variants and were assumed to have acquired infection before their rescue.37 In addition, evidence of a transmissible infectious cell line has not been found.38 Because only complete BPV virions can induce transformation, contamination cannot occur by casual contact with contaminated fomites or affected horses36 or by BPV-infected insect bites39 or blood samples.40 As a result, horses are considered to be nonpermissive hosts for BPV,41 and horizontal BPV transmission remains to be documented.
The presence of viral genetic material appears to be directly associated with tumor development. However, BPV DNA sequences have also been detected in healthy skin36 and in some cases of dermatitis.42 In addition, the presence of viral DNA sequences has also been reported in skin swabs of unaffected horses and in peripheral blood mononuclear cells of horses with unrelated skin lesions (abscess, carcinoma, and hoof canker).40,43 As a result, intracellular persistence of BPV transforming genes is not sufficient to produce the disease, and the role of BPV in the etiology of sarcoids continues to be questioned.22,23
■ Molecular Biology The mechanisms of cellular oncogenesis are similar to those of other transforming papillomaviruses. Cell transformation is associated with episomal or genomic integration and expression of the three transforming genes E5, E6, and E7. The gene products, E5, E6, and E7, are cell cycle regulators necessary for host cell proliferation and viral genome replication. In sarcoids, overexpression of these genes associated with persistent infection underlies cell transformation and progression into tumor cells. E5 is always found and expressed in sarcoids. E5 binds to and activates the platelet-derived growth factor beta receptor (PDGFβR),44 which triggers several downstream effectors pathways controlling cell proliferation, cell survival,44 and invasion.45 E6 and E7 proteins bind to cell cycle control gene products, blocking their activity. They specifically promote cell cycle progression and prevent apoptosis and therefore immortalize the transformed cells.33 E6 is a transcriptional activator that inactivates the apoptotic and cell cycle arrest functions of the tumor suppressor gene p53. Loss of functional activity of tumor suppressor p53 has been confirmed in sarcoid cells in culture and in tumors.14,,,4'j, P53 loss of transactivation function without p53 mutation has been confirmed in sarcoids.48 E7 cooperates with E5 as well as with E6 in cell transformation.49 Although E7 lacks the binding domain of the tumor suppressor retinoblastoma protein (Rb),50 it still inhibits apoptosis in a Rb-independent pathway, which provides transformed cells with a survival advantage.51 The mechanisms by which E7 and its cellular targets contribute to cellular transformation in sarcoids are not fully understood.52
The presence of inflammatory cells of the innate and adaptive immune system that infiltrate sarcoids provide evidence of an antitumor immune response that could eliminate abnormal cells before they can become tumorous in BPV-positive unaffected horses.
Although there is evidence that the inflammatory and immune response may inhibit the development of cancer, BPV1- and BPV2-infected equids seem to lack an effective antiviral immune response to BPV and BPV-infected tumor cells. As a result, sarcoid lesions persist and progress despite the presence of cytotoxic T cells and T-helper cells in lesional and perilesional tissue.53 It is speculated that E5 and E7 downregulation of the immune response may contribute to successful viral infection and allow cells to evade immune surveillance. E5-dependent downregulation of the surface expression of major histocompatibility complex class I (MHC I), by reducing transcription of the MHC I heavy chain gene and blocking transport of the MHC I complex to the cell, has been shown to depress adaptive immune response and allow persistence of infected cells.54 In addition, BPV E7 along with E5 have been shown to block the innate immune antiviral response by downregulation of Toll-like receptor 4 (TLR4) expression.55 Further evaluation of the defective host antitumor response ruled out a recruitment of actively immunosuppressive inflammatory cells such as regulatory T cells (Tregs). Tregs' cell density was not different in sarcoids compared to normal skin.53Although the interplay between BPV E5, E6, and E7 and their downstream targets is critical to immortalize and transform cells as well as to conceal them from the immune system, epidemiologic and experimental data indicate that persistence and overexpression of viral transforming genes are not a sufficient cause to induce sarcoid. The initiation of sarcoid appears to be due to a viral-induced inhibition of apoptosis rather than uncontrolled cell proliferation, as the markers of cell proliferation, such as cyclins and their respective kinases, are not different from those of normal skin19,56 Additional genetic events are required for tumor cells to acquire the traits that enable them to become malignant.
These events are sustained by several mechanisms, including loss of function of tumor suppressor genes, and driven by the host genomic instability that expedites additional mutations leading to malignancy.Genomic instability is a hallmark of cancer progression57 and plays a central role in sarcoid development. Increased genomic instability in sarcoids has been demonstrated by an abnormally high number of genomic aberrations found in tumor cells compared with normal unaltered skin tissue samples.58 Similar genomic instability has been found in cultured sarcoid- derived fibroblasts, suggesting that BPV may directly stimulate genomic instability through DNA replication stress due to loss of p53 function or through oxidative stress due to shifts in energy metabolism to support rapid proliferation.59
Genomic instability in sarcoids has been shown to allow accumulation of mutations of genes engaged in biological pathways common to other cancers. Growth factor signal transduction pathways, including PI3-AKT (phosphoinositide 3-kinase v-akt murine thymoma viral oncogene homolog 1)44 and p38 mitogen-activated protein kinase (MAPK),45 have already been identified. Whole genome scan has been used to identify genetic variants associated with sarcoids.58 The study confirmed an increased genomic instability already detected in tissue culture.59,60 Aberrations of genes involved in immune response (cytokines), generation of metabolites and energy, intracellular signal transduction (PI3-AKT and MAPK pathways), and cell proliferation were identified. In addition, aberrations of common cancer genes, including VEGF, Kit, and Ras, were detected.59
There is good evidence that genomic instability driving progression to malignancy could be promoted by inflammation, viral integration, and epigenetic modifications. The presence of leukocytes within sarcoids provides evidence of a link with inflammation.17 If inflammation can retard or eliminate the tumor, it can also contribute to tumor growth and survival by supplying factors that sustain proliferation and limit cell death and enzymes that facilitate invasion.57 BPV is commonly found in inflamed equine skin conditions.61 Although skin trauma, wound healing, and chronic irritations have been suggested as important mechanisms to allow BPV access to the dermal fibroblasts,43 they are not required, and inflammation alone may be sufficient to allow BPV access to the dermal fibroblasts.61 The inflammation itself may be partly a result of BPV infection, and the inability of some horses to resolve the inflammation in these areas may promote sarcoid formation.61 The inflammatory response may play a role in providing survival and proliferative signals to initiated cells, thereby leading to tumor promotion.
One effector mechanism by which the host fights microbial infection is the production of reactive free radicals that leads to oxidative damage of all cell components and induces host DNA damage actively mutagenic for nearby cancer cells, accelerating their genetic evolution toward states of heightened malignancy, which promotes genomic instability.57-60Epigenetic events are emerging as an important additional mechanism whereby the BPV transforming genes promote development of sarcoids. Epigenetic events are those that can alter phenotype without changing the genotype. Epigenetic mechanisms of silencing or activating expression of nonmutated genes involving DNA methylation and regulatory noncoding ribonucleic acids (RNAs) have been identified in sarcoids. BPV-induced aberrant DNA methylation has been associated both in vitro and in vivo with genomic instability, activation of cell proliferation genes, and silencing of genes involved with immune function.60,62 Further, microRNA deregulation in equine sarcoid tissues resulting in abnormal expression of messenger RNA (mRNA) at the posttranscriptional level has been shown to be engaged in cancer-related pathways, including regulation of cell proliferation, apoptotic pathway, and genomic instability.63
The role played by BPV in the development of sarcoids may be conceptually similar to the role of a genetic predisposing mutation that favors the appearance of the tumor in affected cells. Therefore in the pathogenesis of sarcoids one can identify at least two factors. The first one is related to the effects of transforming genes' proteins, which lead to an environment of genomic instability and local immune suppression. The second factor is the accumulation of cellular genetic damages not related to BPV, needed for tumor development. In humans, viral DNA integration is another factor that plays a critical role in the deregulation of key cellular genes by insertional mutagenesis. Although integration of human papillomavirus (HPV) DNA into the host genome has been shown to positively correlate with the severity of the tumors in humans, there has been no investigation of the role of viral integration in sarcoids.
■ Biological Behavior Sarcoids represent a wide spectrum of fibroblastic tumors ranging from indolent, apparently benign lesions to aggressive and invasive tumors. Clinically, many sarcoids behave initially as benign lesions because they are slow growing, giving the false impression that the lesion is inactive. In addition, sarcoids are frequently classified as biologically benign tumors because they do not metastasize to distant organs and regional lymphatic metastasis is rare and usually associated with multiple unsuccessful treatments.64 However, the equine sarcoid is not a benign tumor because it is a progressive disease that invades and destroys surrounding normal tissue, does not regress spontaneously, and recurs predictably after surgical mass removal.3,33,65 Early lesions are restricted to the dermis and epidermis, but advanced lesions commonly invade the subcutis and may extend through fascia into deeper muscular structures. Considering sarcoids as benign tumors leads to inappropriate management early in the course of the disease and thus to multiple recurrences and also results in unsatisfactory cosmetic and functional outcomes as well as unnecessary expenses to control the disease.
Molecular understanding of the different pathways leading to sarcoids may explain why some lesions remain quiescent for many years and eventually undergo progressive transformation to the aggressive fibroblastic type, whereas other lesions arise de novo as aggressive fibroblastic tumors.3,6,66 The variable presence, type, and location (episomal vs. integrated) of BPV DNA and expression of BPV transforming genes in tumor cells47 as well as the status of the host immune response, may explain the variable appearance, location, and behavior (growth rate, local invasion) of sarcoids. However, clinical manifestation of the disease is not in a simple linear correlation with BPV activity, and the correlation between viral load and disease 46
severity remains controversial.46
Sarcoids share common features with soft tissue sarcomas, particularly the propensity for local invasion of surrounding tissues and infiltration of tissue planes. Tumor invasion of surrounding normal structures is believed to require matrix proteases and metalloproteases (MMPs) to allow cell migration and invasion. It has been shown that the overexpression and activation of MMPs is induced by BPV transforming proteins in equine sarcoid fibroblasts, and recently MMP overexpression by epidermal and dermal cells has also been confirmed in vivo.47,67,68 Identifying signaling cascade controlling invasiveness may provide therapeutic targets against the most aggressive sarcoids.44,45
■ Diagnosis Sarcoids are recognized as having different multiple clinical manifestations, including occult, verrucous, and nodular clinical types (Fig. 40.14).3 In addition, approximately one third of affected horses have multiple sarcoids at different clinical stages at the time of diagnosis.2 The different clinical aspects represent stages of tumor progression and reflect the relative predominance of the dermal or epidermal component. Lesions with a predominant epidermal component include occult and verrucous sarcoids. Occult sarcoids appear as an almost circular area of alopecia with a gray, scaly surface. Verrucous sarcoids may be sessile (flat variety) or pedunculated (warty variety); the skin is thickened with a dry, rough surface, with partial or total alopecia. Nodular sarcoids, also called fibroblastic sarcoids, range in appearance from a dermal or subcutaneous nodule to a large exophytic mass with a skin surface that eventually ulcerates. The nodular type is locally invasive, destroying adjacent tissues, and ultimately may infiltrate lymphatic vessels and nerve sheaths and disseminate to form regional metastases.64 Mixed forms represent a transition from one type to another. The multiplicity of recognized clinical forms confirms the equivocal and progressive nature of the disease.
The polymorphic appearance of sarcoids and the diverse list of differentials make the clinical diagnosis of sarcoids unreliable. The diagnosis and treatment of sarcoids require a biopsy because they are often overdiagnosed clinically. In a review of 681 horses referred to the Equine Oncology Clinic at the University of California, Davis Veterinary Medical Teaching Hospital
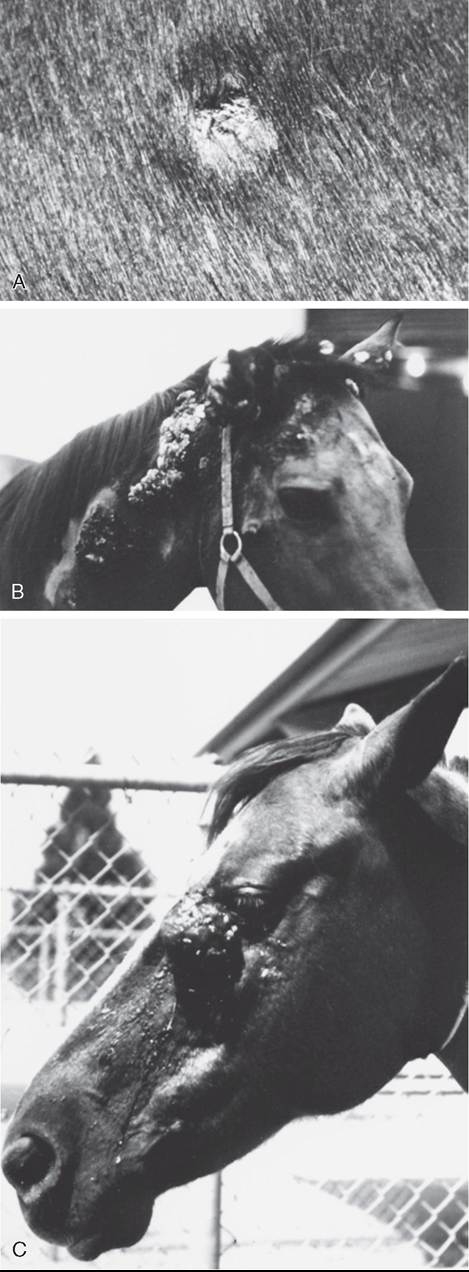
FIG. 40.14 Equine sarcoids. A, Small occult sarcoid. B, Multiple verrucous sarcoids. C, Fibroblastic sarcoid.
for evaluation and treatment of clinically diagnosed sarcoids, 31% of lesions were found to be nonneoplastic dermatologic conditions.69 After ruling out a nonneoplastic skin condition, any clinically suspicious lesion should be biopsied.70 As with any tumor, early recognition and treatment of a small lesion is always associated with a better prognosis. It is important to keep in mind that any large and invasive sarcoid associated with a poor prognosis was, earlier in its evolution, an apparently inactive small lesion that was not recognized or was neglected. There is no contraindication for a biopsy of a suspicious skin lesion as long as definitive and effective treatment is instituted immediately after the diagnosis is made. There should be no fear about performing a biopsy of a suspected sarcoid because very effective treatments are available. However, a biopsy, like any trauma, can increase proliferation of a previously slow-growing tumor and may accelerate tumor progression. As a result, a biopsy should not be recommended if the owner is not willing to pursue treatment, if needed, because the process of biopsy without subsequent treatment has the same effect on overall prognosis as an unsuccessful attempt at treatment.
■ Treatment Sarcoids are low-grade fibrosarcomas and share common features of soft tissue sarcomas. They are locally invasive and tend to infiltrate into surrounding normal tissues through and along fascial planes 2 to 4 cm from the palpable tumor mass. Treatments that are used can be broadly grouped into ablative (surgery, laser vaporization, cryotherapy, hyperthermia, caustic ointments), cytotoxic (radiation therapy, chemotherapy) and biologic (immunotherapy) modalities. The overall treatment goals are (1) to destroy all tumor cells in the gross tumor and also in the normal-appearing surrounding tissues and (2) to minimize damage to healthy tissues. These goals are difficult to achieve with ablative treatment methods because they are not selective against tumor cells. A cuff of surrounding normal tissue containing microscopic disease must be ablated to remove all tumor cells. Early complete surgical resection has a central role in the treatment of sarcoid. Alternate ablative modalities have no oncologic benefits over a well- planned conventional surgery and do not allow histopathologic evaluation of surgical margins to assess the quality of the procedure. Topical applications of escharotics with zinc chloride-based caustic ointments,t,t or 5-FU cream* are used empirically for treatment of sarcoids. Unfortunately, to date, no evidence-based data have been published documenting treatment efficacy against histologically confirmed sarcoids. As a result, no evidence-based information on treatment protocol, efficacy, prognosis, and toxicity is available.
Because tumor size and previous unsuccessful treatment attempts are the most important prognostic factors,65,75 early and histologically complete surgical resection is the mainstay of treatment of sarcoids.70 Failure to eliminate the disease results in regrowth of a tumor that is histologically and biologically more aggressive and requires wider excision than the primary lesion. As a result, it is critical to submit the resected tissue specimen for histopathologic examination to determine the status of the surgical margins. As a rule, grossly or histologically incomplete resection (i.e., positive or close pathologic margins [≤5 mm]) must be followed by a re-resection if possible or by effective adjuvant treatment. For noninvasive sarcoids resected with a pathologic margin greater than 5 mm and for invasive sarcoids resected with a pathologic margin greater than 1 cm, the risk of recurrence is low and no further treatment
other than observation at regular intervals for at least 1 year is recommended. For invasive sarcoids resected with surgical margins between 5 and 10 mm, the risk of recurrence is high and adjuvant treatment may be recommended, particularly when tumor recurrence may be difficult to manage because of unfavorable anatomic location. Access to molecular techniques (PCR and RT-qPCR) designed to detect BPV E5 or E6 in pathologic margins will help assess the risk of recurrence and determine the need for adjuvant treatment.76,77
Among the nonsurgical treatments, radiation therapy and intratumoral chemotherapy with a viscous-fluid, slow-release formulation of cisplatin have well-documented efficacy against biopsy-confirmed sarcoids of all clinical types and in any location.75,78,79 The selective effects of these treatments have the advantage of controlling the disease while avoiding disruption of anatomic structure and preserving function. When compared to radiation therapy, intratumoral chemotherapy with cisplatin is as effective but does not have long-term side effects and does not require any special license. The overall cure rate (all stages and clinical types combined) after treatment with intratumoral cisplatin therapy used alone or as adjuvant to surgery has been reported to be as high as 96%.75 Treatment includes a series of four intratumoral administrations of cisplatin (approximately 1 mg/cm of tissue) given at 2-week intervals. Widely available and inexpensive compounded crystal is formulated in a water and sesame seed oil emulsion stabilized with sorbitan monooleate (Span 80).75 Treatments are done on an outpatient basis under sedation, and the methods of administration and safety precautions have been described.80 Although other antineoplastic drugs81-83 and drug formulations65,80,82,84 for intratumoral chemotherapy have been evaluated, cisplatin in sesame seed oil emulsion remains the most effective drug.75 In an effort to increase duration of tumor exposure to cisplatin, cisplatin-containing biodegradable beads implanted intraoperatively84a have been used but have not shown any therapeutic benefit when compared to conventional intralesional cisplatin administration.75 Attempts to increase cisplatin uptake in tumor cells by applied electroporation85 called electrochemotherapy also failed to show any therapeutic benefit when compared to conventional intralesional cisplatin administration.75 Further, electrochemotherapy requires general anesthesia for each treatment due to painful pulses of electric current as well as expensive equipment and complex procedures.
Systemic chemotherapy with doxorubicin* has shown preliminary evidence of efficacy for fast-growing fibroblastic sarcoids but not for indolent verrucous sarcoids.87
BPV-associated equine sarcoids are distinct from other equine tumors in that they express viral foreign antigens necessary to maintain the cancerous phenotype that could be targeted by the host's immune system. Because sarcoid tumor cells have the potential to be highly immunogenic, immunotherapy has been evaluated for treatment of sarcoids. Nonspecific cell-mediated immunotherapy has been used for sarcoids with inconsistent results. Treatment involves the use of immune stimulatory agents that act nonspecifically to elicit both innate and adaptive immunity and results in the induction of proinflam- matory cytokines, chemokines, and other immune mediators. This in turn leads to the generation of a type 1 helper cell (Th1)-biased cell-mediated immune response and a concomitant generation of cytotoxic effector cells against antigens in the tumor. Bacillus Calmette-Guerin (BCG) cell wall derivatives5 and imiquimod5 are two nonspecific immunostimulants that have been reported for treatment of sarcoids. BCG cell wall derivatives5 administered intralesionally90 have been shown to be effective only for periocular sarcoids.65,91,92 The number of treatments depends on the rate of tumor regression, and the treatment schedule depends on normal tissue toxicity; most sarcoids require two to nine treatments over several weeks.65 Encouraging results have been reported with a biological response modifier used topically (5% imiquimod cream89). The ointment is recommended for the treatment of viral warts and basal cell carcinomas in humans. It was applied as a thin layer to the surface of sarcoids three times a week on nonconsecutive days for up to 32 weeks until resolution.93 However, in our experience, imiquimod treatment was effective only for treatment of persistent cutaneous papillomas in adult horses that have an appearance similar to verrucous sarcoids and a small percentage of occult sarcoids. Treatment did not prevent progression of verrucous or fibroblastic sarcoids. In all cases treatment was associated with severe and painful inflammation of the treated area.
The continued expression of the E5, E6, and E7 proteins by equine sarcoid tumor cells makes them excellent targets for specific immunotherapy.17,18 Therapeutic humoral immunization has not been found effective for treatment of affected horses. Immunization against BPV1 virus-like particles in sarcoid-bearing horses30 and donkeys94 resulted in BPV1 neutralizing antibodies but was not therapeutically effective. Cell-mediated immunity is critical for the control of papilloma- associated tumors.95 Therapeutic vaccines aim to control tumors by activating the patient's own cellular immune response to recognize and kill cancer cells. In humans, trials with therapeutic vaccines that target the E6 and/or E7 proteins using peptide or protein-based vaccines, live vector vaccines, cell-based vaccines, and DNA vaccines have been disappointing for treatment of HPV-associated tumors.95 Although E5 is uniformly expressed by sarcoid tumor cells, no attempt at targeting the E5 protein has been made in veterinary medicine. The renewed interest in E5 protein as a target for therapeutic vaccine in human medicine96 may provide a biological rational for targeting E5-expressing sarcoid cells. Dendritic cells are the central players in the initiation of the adaptive immune response and play a key role in the antitumor T-cell responses. A preliminary study with autologous monocyte-derived dendritic cells (MoDCs) isolated from horses with sarcoids and loaded with tumor lysates showed that the treatment was safe and prevented tumor recurrence after surgery in 13 of the 21 treated horses.97 Although the data are preliminary and need to be confirmed in a larger study, they underscore the need for an increased understanding of dendritic cell biology, which will lead to further development of innovative strategies to optimize vaccine-elicited T-cell antitumor immune responses.
Although therapeutic vaccines aim to develop a strong cellular immune response to BPV antigens that are expressed in transformed cells, prophylactic vaccines aim to prevent a putative BPV infection by inducing a neutralizing antibody response. In humans, prophylactic HPV vaccines act by inducing neutralizing antibodies against the late capsid protein L1 of HPV16 and HPV18. This has led to attempts to establish a vaccine for protection against BPV1- or BPV2-associated sarcoids. Although natural or experimental infection of the skin by wild-type BPV1- or BPV2-associated sarcoid does not induce a measurable antibody response,24 intramuscular immunization of horses with BPV1 L1 virus-like particles has been shown to elicit high titers of BPV1-neutralizing serum antibodies.98 Virus-like particle late protein vaccine proved highly effective in protecting horses from BPV1-induced pseudosarcoid formation (short-lived papules) but not from BPV2 challenge.99 This provides a rationale for developing a preventive vaccine that would benefit naive horses exposed to BPV1 and BPV2. However, immunization of previously exposed latent BPV1- and BPV2-carrier horses would require a vaccine that could stimulate cell-mediated immune responses to specifically target and kill the infected cells. Because it would be impossible to test horses for prior exposure to BPV prior to vaccination and horses need to be protected against both BPV1 and BPV2, the ideal vaccine would have to generate both humoral and cell-mediated immune response to BPV1 and BPV2.