Transient Hypogammaglobulinemia
M. Julia B. Felippe
■ Definition and Etiology Transient hypogammaglobulinemia is a rare disorder characterized by the delayed onset of Ig synthesis in the foal.1-4 Foals normally produce some IgM and trace amounts of IgG in utero and begin to produce significant amounts of immunoglobulins after birth following exposure to environmental antigens (see Fig.
53.4). Assuming adequate passive transfer, maternal antibody fills the void from birth until the foal has produced sufficient autologous antibody for protection (e.g., first 2 months). For unknown reasons, in transient hypogammaglobulinemia, the onset of endogenous antibody production is delayed in the first 6 months of life, but in some cases, protective levels of IgG (i.e., >800 or 1000 mg/dL) may be reached only by 2 years of age. As maternal immunoglobulins wane, the amount of endogenous antibody is transiently insufficient to be protective, making the foal highly susceptible to infections; recurrent pneumonia is a common presentation.This disorder has been described in the literature in an Arabian foal and a Thoroughbred foal, but this author has diagnosed the condition in other foals. It is possible that this condition is underdiagnosed because testing serum IgG concentrations in older foals (i.e., beyond the first week of life) is not common practice in equine medicine. Therefore to make a diagnosis, serial samples may be required to document that autologous Ig is not increasing sufficiently as maternal Ig declines. Many cases that are not followed this closely probably occur.
■ Clinical Signs and Differential Diagnoses Clinical signs occur more often when passively acquired antibodies are catabolized to nonprotective levels, which may happen in the first month of life. As with other Ig deficiencies, signs consistent with the recurrent infections are seen in affected foals.
The differential diagnosis list should include FPT and, if the affected animal is male, agammaglobulinemia.■ Clinical Pathology The cardinal features are persistently low serum Ig concentrations and recurrent bacterial infections that require antibiotic therapy.1,2 Determining low levels or nonprotective levels of Ig in young foals is challenging because of variable amounts of passively transferred immunoglobulins, their catabolism, presence of infections in early age, environmental risks, and age-dependent developmental aspects of the immune system, among other factors. In the event of a robust passive transfer of antibodies at birth, colostrum-derived antibody concentrations are expected to wane by 3 to 4 months of age, and foals with normal immune system development will have produced measurable quantities of endogenous antibodies by then. Therefore serum IgG concentration of 500 mg/dL and serum IgM concentration of 50 mg/dL are commonly measured in affected and normal foals between 3 and 6 months of life; however, in foals with transient hypogammaglobulinemia, the concentrations of immunoglobulins, including IgG and IgM, do not increase with age at the same degree when compared with age-matched samples.
Affected foals have normal cell-mediated responses in vitro and in vivo and appear to be able to respond to immunization to some antigens. Normal numbers of B and T lymphocytes are present in blood and lymph nodes. However, some foals may present CD4 T-cell lymphopenia and low CD4/CD8 ratio distribution (adenoviral pneumonia are often found in SCID foals as compared with other foals. Differential diagnoses include other immunodeficiencies of foals.
SCID in Arabians and Arabian-cross horses has an autosomal recessive mode of inheritance. Thus foals of Arabian breeding that show clinical manifestations of SCID are homozygous for the defective SCID gene. Carriers of the gene are asymptomatic but can be detected by production of an affected offspring or genetic testing.20,21 A correlation between heterozygosity for the SCID allele and the development of sarcoids has been demonstrated, suggesting that the gene may play a role in tumor suppression.6
■ Clinical Pathology A consistent finding on the hemogram of affected foals is an absolute lymphopenia, which is less than 1000 lymphocytes∕μL and often much lower.22,23 Depending on the neutrophil response, the total white blood cell (WBC) count may be low, normal, or elevated, making it essential that the absolute number of lymphocytes be determined. Septic and other compromised foals, as well as some normal foals, may have low lymphocyte counts during the first few days of life; therefore persistent lymphopenia should be established before considering a diagnosis of SCID.24
Concentrations of autologous serum Ig are low in foals clinically affected with SCID.22,25-27 The presence of colostral antibody may mask these low levels of autologous Ig; therefore the degree of colostral transfer and the age of the foal should be considered when interpreting the serum Ig values (see Table 53.6).
In normal foals, IgM is produced in utero, and thus some IgM should be present in presuckle serum.28 Although not pathognomonic, the absence of IgM in presuckle serum is a feature of SCID. Also, due to the relatively low concentrations of IgM in colostrum and the short half-life of IgM (see Table 53.7), maternally derived IgM is generally absent from the circulation by about 3 weeks of age. Thus the absence of serum IgM after 3 weeks of age, although also not pathognomonic, is consistent with SCID.Foals affected with SCID do not respond to intradermal phytohemagglutinin (PHA) by increasing skin thickness as do normal foals, nor do they respond to DTH stimulators, such as dinitrochlorobenzene.29 In vitro tests such as blastogenesis are depressed with all mitogens.22,23,26 The definitive diagnosis of SCID in foals of Arabian breeding is based on genetic testing demonstrating that the foal is homozygous for the defective SCID gene.20,30 Pulled hair, whole blood in ethylenediaminetetraacetic acid (EDTA), or bristle-style cheek swabs may be submitted to VetGen (3728 Plaza Drive, Suite 1, Ann Arbor, Mich., 48108, vetgen@vetgen.com, www.vetgen.com) for DNA testing to determine if a horse is clear, heterozygous, or homozygous for the gene defect. Before the advent of genetic testing, the criteria required to confirm a diagnosis of SCID included (1) persistent lymphopenia (4 asymptomatic carriers of the SCID trait. Mating of a carrier and a normal horse (noncarrier) does not produce any affected foals, but half the offspring would be expected to be carriers.
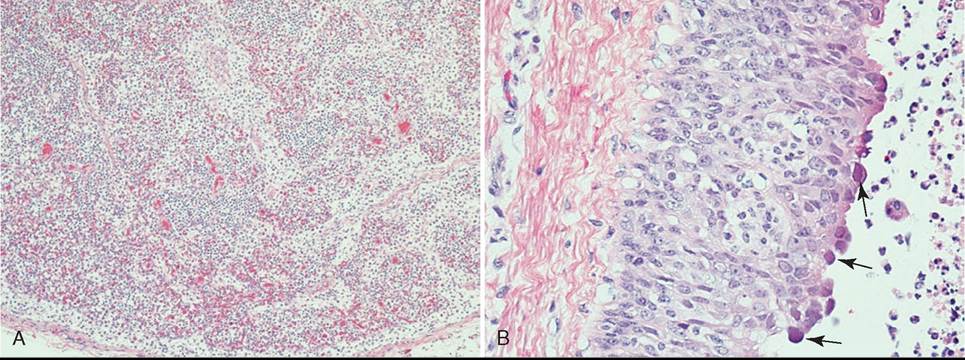
FIG. 53.5 Tissue from an Arabian foal with severe combined immunodeficiency (SCID). The foal presented at 1 month of age for evaluation of persistent pneumonia. A, 200? mediastinal lymph node with extensive lymphoid atrophy. The node is poorly populated with lymphocytes that fail to form lymphoid follicles, and active germinal centers are lacking.
The node is predominantly composed of loosely scattered mononuclear cells and edema. B, 400? tracheal epithelium with adenovirus inclusion (black arrows), epithelial hyperplasia, and suppurative tracheitis. (Photos courtesy Sushan Han.)The disease can be controlled in horses of Arabian breeding by avoiding the production of affected foals, which has been simplified now that carriers can be identified by genetic testing. Mares and stallions intended for breeding should be tested to determine whether they are free or heterozygous for the defective SCID gene. Under no circumstances should two heterozygotes be mated to each other. If an owner decides to continue breeding a heterozygote, the breeding partner should be confirmed homozygous normal. All foals from such matings should be tested to determine if they are clear of or heterozygous for the defective gene (50/50 probability). Only homozygous normal foals should be selected for future breeding purposes, whereas heterozygous foals should be used for nonreproductive purposes. The decreasing prevalence of SCID provides support for the positive effect of genetic screening.6,38,41