Failure of Passive Transfer of Maternal Immunity
M. Julia B. Felippe • Debra C. Sellon
■ Definition and Etiology Normal foals are immunocompetent at birth and capable of mounting an immune response. However, they are immunologically naive: they have had no exposure to foreign antigens and have not yet mounted any type of protective immune response or accumulated significant levels of immunoglobulins.
Although the equine fetus is capable of producing antibodies, newborn foals are essentially devoid of Ig at birth, with the exception of small amounts of IgM normally produced in utero. Without being able to rely on their acquired immunity in the first encounter with pathogens, foals are indeed more susceptible to infectious diseases during the neonatal period. Foals begin mounting immune responses and producing their own Igs immediately on exposure to antigens after birth, and Igs produced by the foal are detectable within 1 to 2 weeks of life and reach significant levels by 2 to 3 months of age.Immunologic protection of the newborn foal therefore relies on the transfer of maternal immunity through the colostrum. Under normal circumstances, temporary protection against infection in the first 1 to 2 months of life is provided to the foal in the form of passively transferred antibodies, cytokines, immune mediators, and a small number of mononuclear cells from the dam (Fig. 53.3; Table 53.6). Because of the diffuse epitheliochorial nature of the equine placenta, no transplacental transfer of Igs occurs in horses. Instead, ingestion and absorption of Ig-rich colostrum within the first day after birth are the sole means of passive transfer of immunity in foals. Serum IgG concentration in healthy foals after ingestion of colostrum under natural conditions varies between 500 and 6000 mg/dL.1-3 In a properly functioning system, maternal antibodies wane as levels of endogenous antibodies increase, and thus the foal should be protected during this transition period (Fig.
53.4; Table 53.7).Failure of the foal to ingest or absorb sufficient quantities of colostrum to provide adequate absorption of IgG is called failure of passive transfer (FPT). Complete FPT is defined as a foal with a serum IgG concentration of less than 400 mg/dL at 24 hours of age. Partial FPT is defined as a foal with a serum IgG concentration of 400 to 800 mg/dL at 24 hours of age. The reported incidence of complete or partial FPT in
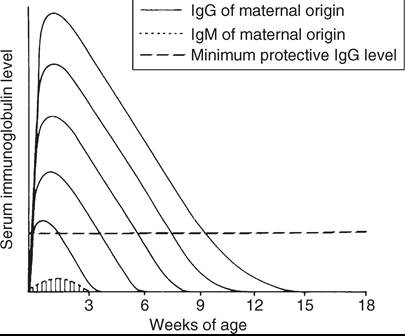
FIG. 53.3 The duration of protection provided by colostral immunoglobulins (Igs) in the foal varies with the isotype of immunoglobulin (e.g., IgG, IgM) and the quantity absorbed during the first 24 hours of age.
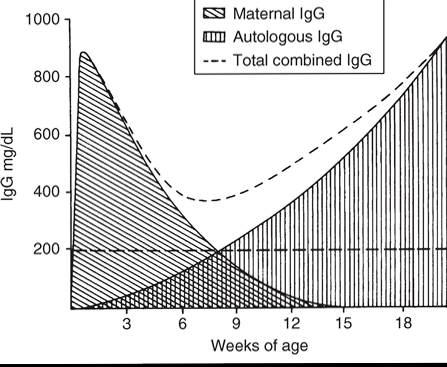
FIG. 53.4 Maternal immunoglobulin (Ig) wanes, whereas the production of autologous immunoglobulin increases during the first several months of life. The combined total amount of immunoglobulin ideally remains above the level considered the minimum for maintenance of good health.
■ TABLE 53.6
Immunoglobulin Concentration (mg/dL) in Equine Colostrum, Milk, and Normal Seruma
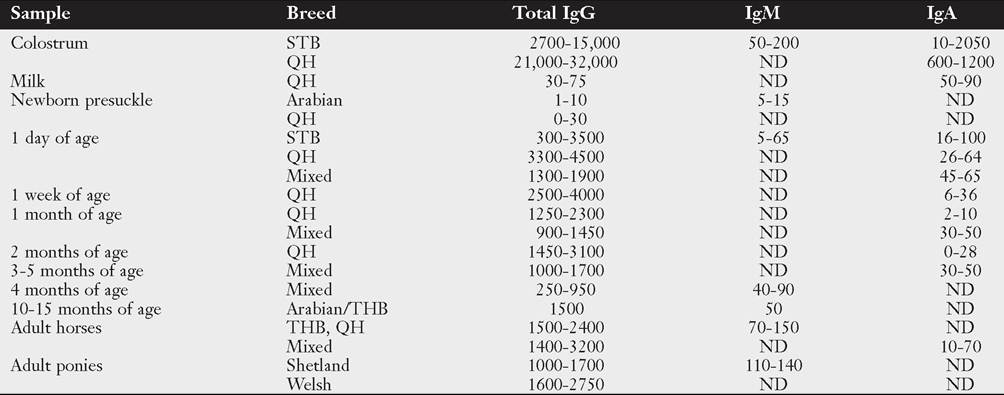
aLow and high values were calculated from mean and standard deviation reported (see references in text). Ig, Immunoglobulin; ND, not determined; QH, Quarter Horse; STB, Standardbred; THB, Thoroughbred.
■ TABLE 53.7
Approximate Half-Life (in Days) of Immunoglobulin Classes in Large Animals
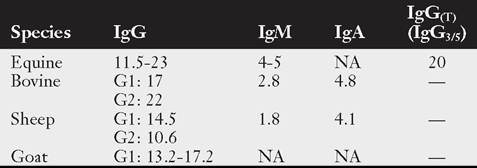
Ig, Immunoglobulin; NA, not available.
From Perryman L: Personal communication, Department of Veterinary Microbiology and Pathology, Washington State University, Pullman, Wash., 1988.
foals varies from 3% to 37.8%.4-11 Risk factors for FPT include month of foaling, adverse health events for mare or foal in the periparturient period, age of the dam, and colostral immunoglobulin content.
Low total Ig content in colostrum is associated with breed (e.g., Standardbred), age of dam (e.g., older mares), and low total solar radiation (i.e., shorter days).5,10,12Immunoglobulins are selectively concentrated from the mare's sera into colostrum in response to hormonal changes that occur in the last 2 weeks of pregnancy; local production in the mammary gland is also possible. The predominant Ig isotype in equine colostrum is IgG, followed by IgA and smaller quantities of IgM.13 The reported amount of total IgG in equine colostrum is variable among different studies (see Table 53.6), but overall a good-quality colostrum should contain 2500 to 5000 mg/dL. The reported amounts of IgA often range between 500 and 1500 mg/dL, whereas IgM generally ranges between 100 and 350 mg/dL. At birth the neonate has specialized enterocytes in the GI tract that can absorb large molecules such as immunoglobulins intact by pinocytosis.14 Absorbed proteins pass through the intercellular spaces and lacteals into the systemic circulation via the lymph. The window of gut absorptive capacity for Igs is narrow, lasting from birth until about 18 to 24 hours of age. Maximal absorptive efficiency occurs immediately after birth, declining to only 22% efficiency at 3 hours after birth and then to less than 1% by 20 hours.15,16 The decline in Ig absorption is accompanied by transient proteinuria that peaks at 6 to 12 hours of age and declines by 24 to 36 hours of age. This proteinuria most likely reflects absorption and excretion of low-molecular-weight milk proteins.16
Diminished Ig absorption over the first 12 to 24 hours of life is the result of shedding of specialized enterocytes capable of pinocytosis and replacement by more mature cells that are incapable of absorbing immunoglobulins.15,17 It has been hypothesized that delayed ingestion of macromolecules may prolong the duration of intestinal permeability to Igs. In one study, however, the type of fluid administered to foals before the ingestion of colostrum did not influence subsequent IgG absorption, suggesting that the process of gut closure is not mediated by a finite capacity for the uptake of macromolecules.18
The half-life for maternal IgG in the foal's circulation varies between 20 and 30 days.19-21 Concentrations decline as a result of normal protein catabolism, gradual dilution associated with an increasing plasma volume as the foal grows, and transfer of functional antibody into the mucosa.
Most maternal antibodies are present in only negligible concentrations by 6 months of age, although antibodies to some infectious agents have been detected for up to 12 months after birth. As passive antibody concentrations decline, endogenous antibody production increases. There is a nadir in serum Ig concentrations in colostrum-fed foals at approximately 1 to 2 months of age, followed by gradually increasing concentrations until adult levels are reached at 5 to 10 months.22,23 Serum Ig concentrations are similar in colostrum-fed and colostrum-deprived foals by 3 to 4 months of age.In addition to antibody, other colostral factors may be important for optimal immune protection of foals. For example, colostrum influences cell-mediated immunity and activates granulocytes. Colostrum contains many constituents of innate immunity and immunomodulating agents, such as cytokines, growth factors, hormones, enzymes, CD4 and CD8 T lymphocytes, macrophages, neutrophils, and epithelial cells.24-26 The cellular components of colostrum are likely to play an especially important role in local GI immunity in the neonatal foal. Maternal cells are found in a variety of blood and tissues in the neonate after absorption of colostrum, suggesting that these cells may also play a role in systemic immunity.24
In foals, FPT may occur because of ingestion of poor-quality colostrum with a low Ig content, failure to ingest a sufficient quantity of colostrum, or failure to absorb colostral Igs from the GI tract.27 Colostrum may have an insufficient quantity of Ig because of prelactation (lactation before parturition), premature foaling, a defect in the mare's ability to concentrate Ig in the colostrum, ingestion of endophyte-contaminated fescue grass or hay, or other factors. Premature lactation is most commonly associated with twin pregnancies, placentitis, and premature placental separation but occasionally occurs without any concurrent uterine, placental, or fetal pathology.
Mares most likely to produce colostrum with low Ig content are those older than 15 years of age, those that foal early in the year, and Standardbred mares.5,10,11 Insufficient colostral Ig concentration has also been associated with ingestion of endophyte-contaminated fescue grass or hay.28,29Foals that are orphaned or rejected at birth, too weak to stand, or unable or lack the desire to suckle are unlikely to ingest sufficient colostrum to prevent FPT. Malabsorption is occasionally incriminated as a cause of FPT in foals that are observed to suckle adequate quantities of good-quality colostrum. This most often happens in premature or dysmature foals, possibly as a result of immature GI function but may also occur in otherwise healthy and vigorous full-term foals.30 Glucocorticoids enhance the maturation of small-intestinal epithelial cells and thus their loss of absorptive capacity, leading to speculation that endogenous corticosteroids released second- 3132 ary to stress at parturition may impair Ig absorption in Ioals.31, However, administration of adrenocorticotropic hormone (ACTH) failed to affect absorption in experimental foals, and stress has not been a consistent historical finding in foals with FPT caused by presumptive impaired Ig absorption.8,33
■ Clinical Signs and Differential Diagnoses The association between FPT and infection has been investigated in numerous studies.4,5,7,10,11 Although the results have varied somewhat, FPT is generally considered a risk factor for infectious disease. By itself, FPT produces no clinical signs of disease and cannot be detected by physical examination. Clinical presentations that strongly suggest an underlying problem with FPT include onset of bacterial infections within the first 2 weeks of life, particularly septicemia, septic arthritis, pneumonia, and enteritis. Other immunodeficiencies or simply exposure to potent pathogens cannot be ruled out solely based on the time of onset; however, even with other forms of immunodeficiency, clinical signs of infection usually do not show up for several weeks if passive transfer is adequate.
■ Clinical Pathology FPT is diagnosed by the demonstration of low serum concentrations of IgG in the foal as early as 6 to 12 hours after birth, typically between 12 and 24 hours after birth, and probably for as long as several weeks after birth (see Table 53.6). The level of IgG considered adequate for protection against infectious disease is poorly defined and probably varies considerably with the environment. A serum IgG concentration greater than 800 mg/dL is considered to provide adequate protection for most foals in their first few weeks of life. In contrast, an IgG concentration of 400 to 800 mg/dL in a foal at high risk for sepsis because of its environment or other factors indicates the need for Ig replacement. Importantly, these figures only address total Ig content and not pathogen-specific antibody titers, which also play a critical role in determining risk for certain infectious diseases.
In healthy foals that nurse within 2 hours of birth, serum IgG concentrations become detectable at approximately 6 hours of age and peak at approximately 18 hours. Routine determination of serum IgG concentrations in apparently healthy foals is usually recommended between 12 to 24 hours of age. Foals considered to be at high risk for FPT and sepsis may be assessed as early as 6 to 12 hours of age.34,35
Importantly, since endogenous production of Igs in the foal takes an average of 2 to 4 months to reach protective levels, and colostrum-derived IgG concentrations decrease at a half-life of about 20 to 30 days, it is critical to ensure that minimum levels of transfer (>800 mg/dL or perhaps 1000 mg/dL serum IgG concentration) are measured after ingestion of colostrum in the foal's blood; this minimum amount of colostrum-derived IgG is expected to protect the foal beyond the first week of life, bridging this transition period in the first few months of life (see Fig. 53.3).
Described methods for IgG quantitation include turbidimetric immunoassay, radial immunodiffusion (RID), enzyme-linked immunosorbent assay, zinc sulfate turbidity, latex agglutination, and glutaraldehyde coagulation.34,36-41 Selection of an appropriate screening test for a specific farm or foaling environment should be made after considering overall accuracy based on sensitivity and specificity, time necessary to perform the test, simplicity of the testing procedure, technical skills and knowledge of the attending personnel, and cost. Turbidimetric immunoassay and RID are the most accurate quantitative (actual value) diagnostic tests; turbidimetric tests provide immediate results, whereas RID turnaround is 24 hours, which may be impractical when an at-risk foal needs rapid diagnosis and treatment. Total serum protein is not a reliable indicator of FPT in foals (unlike calves) because of the wide variation in total serum protein in cases of adequate transfer; serum globulin values correlate better with IgG values when using appropriate cutoff points.41-45 Many veterinarians prefer to use semiquantitative commercial kits based on enzyme-linked immunosorbent assay or glutaraldehyde coagulation technology for stall-side screening of foals.40-43 Both types of tests have high sensitivity and negative predictive value. False-negative and false-positive results tend to be more common when attempting to accurately identify foals with partial FPT of IgG concentrations between 400 and 800 mg/dL. These tests do not provide actual values above 800 mg/dL, which prevents predicting humoral protection throughout the first few months of life, given the half-life of colostrum-derived IgG (see Fig. 53.3).
No consistent changes in the blood work are seen in foals with FPT; however, a range of abnormalities related to secondary infection (e.g., neutrophilia, neutropenia), hyperfibrinogenemia, and hypoglycemia may be present. The presence and severity of these changes depend on the organisms and systems involved.
■ Necropsy Findings No specific necropsy findings are indicative of FPT. Necropsy findings reflect the site and severity of secondary infectious problems that have developed. Lymphoid tissue is normally developed, unless secondary infections have caused lymphoid necrosis or atrophy.
■ Treatment and Prognosis Treatment of FPT depends on the degree of FPT, the environment in which the foal is exposed, the foal's age at diagnosis, and the presence of secondary infectious problems. Treatment is aimed at minimizing exposure to pathogens, supplying immunoglobulins, and managing secondary infections, if present.
If FPT can be anticipated within hours of birth because of premature lactation, low-specific-gravity colostrum, or a weak or orphaned foal, treatment can include the provision of an alternative source of colostrum or antibody orally. Foals with complete colostrum deprivation require approximately 1.5 g IgG/kg body weight to achieve a peak serum IgG concentration of more than 800 mg/dL. In a 45-kg foal, administration of 1 to 3 L of colostrum with a specific gravity greater than 1.060, divided into multiple hourly feedings over the first 6 to 8 hours of life, is desirable. Mares that donate colostrum for feeding should be healthy, checked for blood type, negative for anti-RBC alloantibodies (especially anti-A and anti-Q), and appropriately vaccinated during the last 4 to 6 weeks of gestation.
If equine donor colostrum is not available, bovine colostrum, a commercial colostrum substitute, or equine plasma may be administered orally to the foal.46-53 Because bovine colostrum is often more readily available than equine colostrum, it may be substituted in emergency situations when equine colostrum is not available. Bovine colostrum is relatively well absorbed in the foal, but bovine immunoglobulins have a much shorter half-life in foals and do not contain antibodies specifically directed against equine pathogens. It is certainly better than no colostrum and, on the basis of a small experimental study, may be used without creating adverse reactions.4’’’ Approximately 2 to 4 L should be administered orally, and many foals develop transient mild diarrhea; increased colostrum-derived gamma-glutamyl transferase (GGT) values will be measured in the foal's blood for a few weeks.
Concentrated equine serum products such as Seramune Oral (Sera, Inc., Shawnee Mission, Kan.) are available for use in foals with FPT.54 In one study, however, it failed to increase serum IgG concentrations in colostrum-deprived foals to adequate levels, probably because of the relatively low total IgG dose administered.53 If the product contains 25 to 30 g of IgG/300-mL bottle, approximately three bottles may be required to increase the serum IgG concentration of a 45-kg colostrum-deprived foal to greater than 400 mg/dL.53
If no other sources of immunoglobulin are available for a foal, oral administration of equine plasma or serum may be considered. This is an expensive source of oral Ig, however, and approximately 2 to 4 L are required to treat a colostrum- deprived 45-kg foal.
If the foal is older than 6 hours of age, the absorption of colostral antibody is significantly decreased, although a locally protective effect of the colostrum may still be present in the intestinal tract. If the foal is older than 12 hours of age, it is unlikely that sufficient colostrum will be absorbed; therefore Ig levels should be rechecked at 24 hours and intravenous (IV) plasma transfusion given, if indicated by persistently low serum Ig levels.
Some animals with FPT, particularly partial FPT, do well without treatment if they are systemically healthy, are not heavily exposed to pathogens, and have no preexisting infections. FPT itself is not necessarily fatal. If plasma transfusions are not administered, owners should be made aware of the risks, and these foals should be maintained in an environment with minimal exposure to potential pathogens. Foals with other risk factors for septicemia (e.g., prematurity, dysmaturity, placentitis) should receive IV plasma transfusions if they have blood IgG concentrations of less than 800 mg/dL at 12 to 24 hours of age. Importantly, foals with FPT may develop recurrent infections around 1 to 2 months of age when blood IgG concentrations are below protective levels or until endogenous IgG production reaches protective values. Therefore checking serum IgG concentrations should also be a practice in foals with recurrent infections during this transition time.
If the decision is made to supplement plasma parenterally, equine plasma for transfusions can be collected and processed locally or obtained commercially. Available sources of commercial equine plasma include Plasmune (formerly Foalimmune) and HiGamm-Equi (Lake Immunogenics, Inc., Ontario, N.Y.); Equi-Plas and Polymune (Plasvacc USA, Inc., Templeton, Calif.); and Immuno-Glo Normal Equine Plasma (Mg Biologics, Inc., Ames, Iowa).55 Commercial sources are convenient, save time, have been screened for anti-RBC antibody, contain minimal amounts of RBCs, are free of diseases such as equine infectious anemia, and originate from animals with known Ig levels. The major disadvantage is that plasma may not contain antibodies specific for the pathogens from the particular environment to which the foal is exposed.
Use of a local donor has the potential benefit of providing antibodies specific to the environmental pathogens to which the foal has been exposed. If a local donor is to be selected, several criteria should be met. First, the horse should be healthy, and results of agar gel immunodiffusion for equine infectious anemia should be negative. Second, no anti-RBC antibody should be detectable in the horse's serum. The donor's plasma should be screened for lysins and agglutinins by a blood-typing laboratory against a panel of cells representing all known blood groups. If plasma evaluated in this way is not available, the presence of anti-RBC antibody in donor plasma can be crudely evaluated with a minor crossmatch for agglutination using donor plasma and recipient blood cells. Lytic antibodies require an external source of complement for activity in vitro and may not be detected using this test.
Ideally, a third criterion is selection of a horse that is negative for blood group factors Aa and Qa. Even though there are dozens of blood group factors, Aa and Qa have been associated with the great majority of cases of neonatal isoerythrolysis (NI).56-58 If plasma is collected and separated by sedimentation, it is inevitable that some RBC contamination be present. If Aa-positive (Aa+) RBCs are given to an animal that is Aa negative (Aa-) or if Qa+ RBCs are given to an animal that is Qa-, the recipients could become sensitized to these antigens. This sensitization probably would not have any immediate consequences for the recipient foal because the foal's cells would not be affected by the antibodies, but it has potentially sensitized any Aa- and Qa- females for production of a foal with NI later (see the Diseases Caused by Allogeneic Incompatibilities [Horses and Ruminants] section later in this chapter). To avoid these potential complications, the ideal donor should be Aa- and Qa- and possess no anti-RBC antibody in its serum. It is desirable to have identified this type of donor to avoid the need for immediate crossmatching in every case of plasma transfusion.
The volume of plasma needed to correct the measured IgG deficit in a foal can theoretically be calculated on the basis of the blood volume of the foal and the concentration of IgG in the foal's serum and in the donor plasma; however, these calculations do not reliably predict the actual levels of IgG achieved after transfusion.34,59 A 20-mL volume of plasma per kilogram of body weight administered intravenously in general raises serum IgG levels 200 to 300 mg/dL, and often two to three times this amount is necessary to bring serum IgG levels into the range considered the minimum for protection (e.g., 800 mg/ dL).34,60 If the foal is already clinically ill, additional plasma often will be required to raise IgG levels an equivalent amount.34,40 In a newborn foal (estimated at 50 kg) with complete FPT, between 2 and 4 L of plasma is frequently necessary.
Plasma should be administered through an IV catheter placed aseptically in one jugular vein. Frozen plasma is thawed and warmed slowly to room temperature in a lukewarm water bath. Microwave thawing or thawing with high temperatures is not recommended because this may denature important plasma proteins. An appropriate in-line blood filter should be used for IV administration of any blood product to remove fibrin clumps and other debris. Initial infusion rates should be slow (0.5 mL/kg over 10 to 20 minutes) to monitor for adverse reactions. Muscle fasciculations, piloerection, increased heart or respiratory rate, fever, respiratory distress, abdominal pain, soft feces, blanching of mucous membranes, and collapse are indicative of transfusion reactions. One dose of flunixin meglumine has been used in cases of adverse reactions, and plasma transfusion may be attempted again at a slower rate. In the absence of these or other adverse effects, the remainder of the transfusion may be administered in 30 to 40 minutes. Slower infusion rates are recommended for foals that are systemically ill. If other IV fluid therapy is being administered concurrently, slower infusion rates are also indicated to diminish the likelihood of inadvertent fluid overload.
Serum IgG concentrations in the foal should be rechecked 24 hours after plasma transfusion to confirm that the desired increase has been achieved. The delay from transfusion to IgG assessment is necessary to allow for distribution of Ig into extravascular spaces. Healthy foals transfused with plasma at 1 day of age experienced a 30% decrease in serum IgG concentrations by 7 days of age.59 This decline may be even more marked in septic foals with increased vascular permeability, increased catabolism, and increased demand for use in immune responses.
Although several equine serum-derived products are marketed for IV administration in the treatment of foals with FPT, these products have been associated with significant adverse reactions in some foals. Administration of high-quality equine plasma is preferred for treatment of foals with FPT.
■ Prevention and Control Evaluation of colostral Ig content has proved to be valuable in predicting the occurrence of FPT and assessing the neonate's risk for FPT.34,61 Colostrum with high Ig concentration tends to be sticky, yellow, and thick, but these subjective criteria are unreliable in assessing colostral quality. The quantity of Ig in colostrum may be more accurately estimated by single RID, refractometry, glutaraldehyde coagulation, or specific gravity.62 Because 24 hours are required to read the results of RID, it is more practical in a field situation to assess specific gravity with the other tests. A handheld Brix 0% to 50% sugar refractometer provides a simple and costefficient stall-side screening test for assessing colostral quality.63,64 A Brix reading of 20% to 30% correlates with adequate colostral quality; a reading greater than 30% indicates good-quality colostrum.65 A commercial kit based on glutaraldehyde coagulation of immunoglobulins is the Gamma-Check-C (Veterinary Dynamics, San Luis Obispo, Calif.). Colostral specific gravity using a colostrometer such as the Equine Colostrometer (Lane Manufacturing Company, Denver, Colo.) should be at a minimum of 1.060, corresponding to an IgG concentration greater than 3000 mg/dL; levels of 6000 mg/dL or higher are desirable. Approximately 75% of foals that ingest colostrum with a specific gravity less than 1.060 will have serum IgG concentrations less than 400 mg/dL; when colostral specific gravity is greater than 1.060, foals usually attain serum IgG concentrations above 500 mg/dL.62
Some of the causes of FPT can be alleviated or recognized for early intervention by careful management. These include identification of mares that drip colostrum before parturition, attendance at foaling to ensure that foals suckle within several hours of birth or are supplemented artificially with colostrum, and screening of high-risk foals with doubtful nursing histories. Routine screening of foals between 12 and 24 hours of age allows early identification of FPT and potentially allows for therapy before the onset of infections. Although signs of septicemia secondary to FPT are often first observed on days 3 to 4 of life, a bacteremia may already be present at 24 hours of age or earlier.62,65
A colostrum bank can be established by collecting small amounts of colostrum from lactating mares (e.g., 200 to 250 mL) within the first 2 hours after foaling. This is only about 10% of the total colostrum produced by the average mare in the first 24 hours after parturition and therefore does not adversely affect the foal suckling the donor mare. Although the volumes are quite variable, mares produce about 300 mL of colostrum per hour and about 5 L during the first 18 hours. Colostrum can be stored frozen for at least 1 year at standard freezer temperatures, approximately -20° C (-4° F). Although frozen immunoglobulins are stable for much longer, the overall quality of the colostrum may deteriorate. Ideally, banked colostrum should be screened for the presence of anti-RBC antibodies as advised for plasma. Colostrum typically has low titers of agglutinins, which are probably not of significance unless they present a dilution of one eighth or greater.
More on the topic Failure of Passive Transfer of Maternal Immunity:
- Failure of Passive Transfer of Maternal Immunity
- REFERENCES
- Neonatal Encephalopathy
- The Immunological Benefits of Colostrum
- REFERENCES
- History
- References
- Ovine and Caprine Vaccination Programs
- REFERENCES
- Overview of Immunologic Disorders in Horses