Traumatic Reticuloperitonitis (Hardware Disease, Traumatic Reticulitis)
David Francoz
Definition and Epidemiology
TRP, or hardware disease, is a frequent disease of cattle but it is rarely diagnosed in small ruminants. It is considered the most common cause of anterior abdominal pain in cattle.
The ingestive behavior of cattle allows sharp nonfood items to be prehended and swallowed. Ingestion of such items by sheep or goats is rare. The disease affects confined cattle where mechanical processing of forages or construction activities increases the chances that piece of wire or nails will be included in the feed.Few data available are on the frequency of TRP in cattle. In one study in Denmark, data were collected on 222,490 cows from 5979 herds. TRP was presumptively diagnosed by veterinarian in 1621 (0.7%) cows in the year before slaughter and in 1521 (0.7%) cows at slaughter. However, in only 48 of these 1521 cows had TRP been diagnosed by a veterinarian premortem.1 Grohn and Bruss2 reported a similar prevalence (0.6%) of TRP veterinary diagnosis in live dairy cattle in 1990. Data from England and Wales indicated that 141 of 2709 adult cattle carcasses submitted to the Veterinary Laboratories Agency from January 2004 to May 2008 had a diagnosis of TRP.3 In western Canada, TRP was the most frequent postmortem findings (8%) in beef cows and replacement heifers.4 Most cases are sporadic, but outbreaks have occurred when such things as multistranded cable have been chopped up by a forage harvester and ensiled or when cattle have chewed nails containing charcoal from burned buildings.
Etiology and Pathophysiology
The ingestive behavior of cattle predisposes them to the accidental swallowing of metal foreign objects. Ingestion of a foreign body may also be associated with diseases that cause pica, such as phosphorus deficiency.5 Foreign bodies of high specific gravity initially settle to the bottom of the ventral sac of the rumen.
Subsequent contraction cycles of the forestomach move those objects from the rumen into the reticulum. Subsequently, depending on the presence of a magnet, four things can happen to a sharp foreign body6: (1) It may attach to the magnet without any clinical disease; (2) it can penetrate the reticular wall only with intramural inflammation; (3) it can perforate the reticulum wall, penetrate into the peritoneal cavity, and create a localized septic peritonitis; or (4) it can migrate into the peritoneal and thoracic/pericardium cavities. The diaphragm, pericardium, and heart muscle are located just cranial to the reticulum, with the liver positioned medially and dorsally and the spleen laterally and dorsally. These organs are sometimes penetrated by foreign bodies and become involved in the inflammatory and infectious process. The pain and inflammation associated with the trauma and infection lead to decreased appetite and ruminal hypomotility or stasis. Agalactia is abrupt because of the acute anorexia and subsequent failure to absorb precursors for milk synthesis.Rehage and colleagues7 suggested that the motility disturbances of ingesta through the forestomachs and the abomasum in cows affected with TRP develop in three phases. The first one, characterized by poorly comminuted feces, occurs after reduce or arrest of the reticulum contractions caused by pain and inflammatory adhesions. With extension of the adhesions, additional impairment of reticulum motility develops. In this second phase, stratification of the food particles in the reticu- lorumen is lost, volume of these two forestomachs is increased, and ruminal outflow is reduced. In the third phase, the consistency of ruminal contents is changed and becomes pasty with high viscosity. Increase in viscosity of ruminal content leads to inhibition of the transpyloric outflow. Abomasal volume increases and internal vomiting occurs.
Clinical Signs and Differential Diagnosis
TRP in the most severe, acute form is characterized by fever, anorexia, decrease in or absence of ruminal contractions, and evidence of cranial abdominal pain.
Pinching of the withers or upward pressure on the xyphoid region may elicit a grunt on expiration. Affected cattle may stand with an arched back and resist ventral flexion of the back when pinched over the withers (normal cattle flex ventrally). Some cattle grunt spontaneously when forced to move or when defecating or urinating. Lactating cows show a sudden decrease in milk production. Some cows regurgitate ruminal fluid, especially if the oropharynx is mechanically stimulated. Tachycardia, reluctance to move or lie down, mild bloat, constipation, or abducted elbows may also be observed. These typical signs often abate within the first day or two, making diagnosis more difficult as the disease progress. Sudden death has occurred as a result of the laceration of a coronary blood vessel or puncture of the heart by the foreign body.Less severe or more long-standing cases show clinical signs that are more subtle and less specific. Cows in early lactation may have ketosis; however, a distinguishing feature of TRP is the abrupt onset of anorexia and hypogalactia. Fever may be absent or very mild. Weight loss, rough hair coat, diarrhea, or generalized lameness, along with cranial abdominal pain that is difficult to localize, may be the only clinical signs.
If the pericardial sac has been seeded with bacteria, pericarditis usually develops. Clinical signs of pericarditis are discussed in detail in Chapter 30. In addition to the clinical signs previously described for TRP (decreased appetite, fever, tachycardia, pain), muffled heart sounds, jugular vein distention, and edema of the submandibular region, brisket, and ventral abdomen are typically observed.8
The foreign body may penetrate the liver or spleen, which leads to abscess formation. These abscesses, as well as reticular adhesions, may be responsible for reticuloomasal outflow problems and may lead to chronic indigestion.7 TRP is a leading cause of chronic indigestion, more specifically of type 2 chronic indigestion (i.e., failure of omasal transport).
Agreement between premortem and postmortem diagnosis of TRP has been reported to be low, which can be explained by the low specificity of the clinical signs associated with TRP.1 TRP must be differentiated from other causes of cranial abdominal pain. They include localized peritonitis associated with abomasal ulcers or liver abscesses, pleuritis, and pericarditis. In one study, cows with a premortem diagnosis of TRP not confirmed during postmortem examination were more likely to have one of the previously listed diseases detected post mortem.1 More information regarding the differential diagnosis of abdominal pain is presented in the section on acute abdomen in cattle. When thoracic structures are involved, TRP must be differentiated from pneumonia or pleuritis, diaphragmatic hernia, and heart diseases such as endocarditis, lymphosarcoma of the heart, and cor pulmonale. Finally, TRP must be differentiated from others causes of ruminal distention and chronic indigestion.
Ancillary Tests
COMPLETE BLOOD CELL COUNT. The WBC count and differential may indicate an acute or chronic inflammatory process depending on the stage of the TRP. Neutropenia and a left shift are expected in acute cases. However, in more chronic cases, changes are less pronounced, and both the WBC count and differential may return to normal,6 but modification associated with chronic inflammatory diseases such as eryth- rocytopenia, thrombocytopenia, and hypohemoglobinemia may also be noted.9,10 Gokce and colleagues9 also reported longer activated partial thromboplastin time, prothrombin time, and thrombin time in cattle affected by TRP than in a control group of healthy cattle.
PLASMA PROTEINS AND ACUTE-PHASE PROTEINS. High total plasma proteins, primarily reflecting high globulin levels, are expected in chronic cases of TRP.9,11 Higher concentrations of total plasma proteins has been observed in cases of TRP than in other abdominal disorders.12,13 Plasma proteins concentration of 87 g/L12 and 100 g/L13 have been proposed for the differentiation between TRP and other abdominal disorders.
Elevated fibrinogen concentration may be observed in acute (2 to 3 days after the beginning of the disease) and chronic cases. A significant increase in fibrinogen concentration has been reported in comparison to healthy control cows.14 In addition, studies in referral centers have demonstrated highest plasma fibrinogen concentration compared with other abdominal disorders.12,13,15 Cutoff points have also been reported in these studies for the differentiation between TRP and other abdominal disorders. Jafarzadeh and colleagues13 proposed a value of 6.91 g/L (with a sensitivity and specificity of 81% and 72%, respectively), whereas Nazifi and colleagues15 suggested a value of 5.7 g/L (with a sensitivity and specificity of 32% and 100%, respectively).
Serum amyloid A and haptoglobin concentrations have also been reported to be elevated in case of TRP.12,14"16 Cutoff points for the differentiation between TRP and other gastrointestinal disorders of 0.67 g/L12 and 0.74 g/L15 for haptoglobin and 68 μgZmL15 for serum amyloid A have been reported. These two parameters seem to be more accurate than plasma fibrinogen or protein concentrations for the differentiation between TRP and other gastrointestinal disorders.12,15 However, in one study, a nonsignificant increase of serum amyloid A was observed in cases of TRP in comparison to healthy control cows.14 Of importance is that other inflammatory disorders can induce the same modifications, and absence of these abnormalities does not rule out TRP. Other diagnostic tests thus must be performed to confirm the diagnosis
SERUM BIOCHEMISTRY PROFILES AND BLOOD GAS ANALYSIS. Serum biochemistry profiles and findings of blood gas analysis are usually within normal range but may reflect anomalies associated with ileus and chronic indigestion, such as hypochloremic metabolic alkalosis, hypokalemia, and hypocalcemia.10,11 Other abnormalities reported include increases in specific and nonspecific indicators of liver damage (such as aspartate aminotransferase, ALP, lactate dehydrogenase, and bilirubin),6,9,10 and increases in specific and nonspecific indicators of skeletal or cardiac muscles (such as CK [CK-MB], lactate dehydrogenase, aspartate aminotransferase, and cardiac troponin).9-11
DIAGNOSTIC IMAGING.
Ultrasonography and radiography are complementary methods that provide different and useful information for the diagnosis and management of TRP. Radiography of the reticulum is available only in centers where powerful equipment is available. Different techniques have been described for radiography of the reticulum. They can be performed on recumbent or standing animals; lateral radiographic views of the reticulum on standing animals are the recommended methods. Radiographs allow the detection of a metallic foreign body and the determination of its location in or outside the reticulum. They can also be useful in order to assess the success of magnet administration. Different parameters criteria may be evaluated on radiographs for the diagnosis of TPR. They include presence or absence of a foreign body, position of the foreign body, presence of focal gas shadows or gas-fluid interface near the reticulum, and the shape, size, and location of the reticulum (Fig. 32.132).17-19 Of these parameters, location of the foreign body is the most reliable indicator for the diagnosis of TRP.12,14Ultrasonography of the reticulum is presented elsewhere in the Diagnositic Imaging subsection of the Acute Abdomen section in this chapter. Ultrasonography provides information about the localization and extension of peritoneal effusion, the presence of perireticular abcesses, and the contraction of the reticulum.20 Ultrasonography is also the most useful complementary examination for the diagnosis of pericardial effusion.7
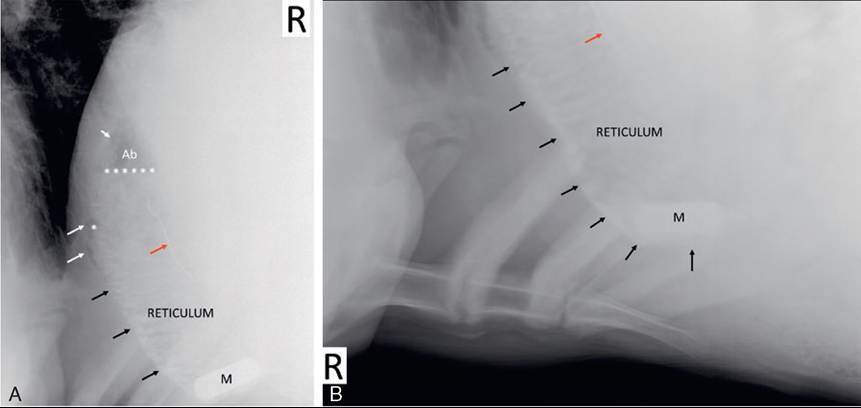
FIG. 32.132 Radiographs of the reticulum of a cow with traumatic reticuloperitonitis. Two lateral views were obtained: a craniodorsal view (A) and a caudoventral view (B). The reticulum is displaced dorsally and cranially. Its contour (black arrows) is irregular. Multiple gas bubbles (white arrows) are observed, and fluid lines (white asterisks) are also visible. Those observations are compatible with septic peritonitis and possible abscesses formation (Ab, large abscess). A linear foreign body (red arrow) is visible in the two views but most easily evaluated on the craniodorsal view. This foreign body is not attached to the magnet (M). (Courtesy Centre Hospitalier Universitaire Veterinaire de !Universite de Montreal.)
AbdominocentESIS. Abdominocentesis and pericardiocentesis may be performed blindly or with ultrasound guidance. Abdominal fluid analysis and its limitations in cattle are discussed in the Peritonitis in Ruminants section. Pericardiocentesis may be performed at the level of the point of the elbow in the left fifth intercostal space. Aseptic preparation of the skin and local anesthesia of the region to be punctured are required; pulling the left forelimb forward may be helpful. A 5- to 10-cm spinal needle or intravenous catheter can be used; the length required depends on the size of the animal and the amount of subcutaneous fat. Previous ultrasonographic examination is helpful for the choice of the needle. Caution is advised for advancing the needle to prevent laceration of the myocardium or of a coronary vessel. Ultrasonographic guidance helps prevent trauma to the myocardium. Visual inspection of the fluid obtained is usually adequate to confirm the diagnosis of pericarditis; in case of septic traumatic pericarditis it is cloudy and foul smelling. The fluid may be examined bacteriologically and cytologically.
Treatment
Conservative medical treatment is generally attempted first. It is based on the administration of a magnet for attachment of the foreign body, parenteral antibiotic therapy for the control of infection, administration of NSAIDs for the control of pain and inflammation, and the correction of dehydration and electrolytes imbalances when present. Different drugs have been used to enhance the chance of the magnet to enter the reticulum cavity. The effects of premedication with atropine, scopolamine, or xylazine and the practice of standing the cow with its forelimbs 30 cm lower than its hindlimbs on successful administration of a magnet (i.e., adequately located in the reticulum cavity) have been evaluated in healthy cows.21 Adequate location of the magnet was controlled radiographically 1.5 hours after the administration of the magnet. None of the procedures increased the chance of the magnet's being successfully located in the reticulum. In all groups (treatment groups and control groups), only 57% of the magnets were adequately located in the reticulum.21 In one study, Braun and coworkers evaluated radiographically the efficacy of magnet administration for the treatment of TRP.22 They demonstrated that foreign bodies that have already penetrated the reticulum wall or that have clearly perforated the reticulum before magnet administration had approximately a 54% and 32% chance, respectively, of becoming attached to the magnet.
Treatment of peritonitis requires systemic antibiotic therapy and possibly drainage of the affected area; surgical correction of the inciting cause is discussed in the Peritonitis section in this chapter. Forestomach bacteria are involved the in acute phases, and T.pyogenes and anaerobic bacteria in chronic cases when perireticular abscesses are present. NSAIDs are the drugs of choice for the control of inflammation and pain. However, the risks associated with their side effects, abomasal ulcerations and renal toxicity, should be evaluated in case of anorexic and dehydrated animals. Multimodal approaches such as the combination of NSAIDs and opioids or continuous infusion of analgesics should also be considered for pain management.23 Institution of fluid therapy is necessary in cases of diffuse peritonitis and associated hypovolemic shock, as well as for the correction of electrolytes imbalances associated with ileus or indigestion. Physiologic salines (0.9%) containing potassium and calcium are the solutions of choice.
Many cattle recover after such a course of medical therapy with resumption of forestomach motility and appetite within 1 to 3 days. Appetite and rumination activity monitoring is also useful for an objective assessment of the response to treatment. These parameters have been reported to normalize within 3 to 5 days after the initiation of medical treatment or rumenotomy.24 Animals that have not significantly improved by the third day may require a rumenotomy to remove the foreign object. Ideally, radiography combined with ultrasonography is recommended at this time to verify the diagnosis and objectively assess the response to treatment,22 but ultrasonography is more feasible in most practices. During rumenotomy, abscesses that adhere tightly to the reticulum may be drained into the lumen of the reticulum. In some instances, reticular abscesses may also be drained through an ultrasonography-guided transcutaneous incision,25 ultrasonography-guided insertion of a chest trocar, or insertion of a trocar during ventral laparotomy.6
Prognosis
The prognosis of TRP depends mainly on the location of the foreign body and the other organs affected. The prognosis is fair to good when TRP is associated with localized peritonitis and when only the spleen or the liver is also affected. The prognosis is poor to guarded in TRP associated with pericarditis, pleuritis, or diffuse inflammatory adhesions in the abdomen.6,7,26 In most cases, as inflammation diminishes, the reticular function can return to normal.26 In a multicenter retrospective study on rumenotomy and rumenostomy, data on long-term outcome (5 months to 5 years after the procedure) were available for 23 bovines that underwent rumenotomy for TRP: Six bovines (26%) were still in the herd and productive, 9 (39%) were removed from the herd, and 8 (35%) died or were euthanized.27
Necropsy Findings
Cattle that die peracutely may have a lacerated myocardium with resulting hemorrhage or cardiac tamponade. Diffuse peritonitis characterized by copious, foul-smelling peritoneal fluid with an obvious reticular defect may be present in acute cases. More chronically affected animals may have extensive pericardial effusion with a thick epicardial layer of fibrin if the pericardium was penetrated. Localized peritonitis with adhesions alone is unlikely to kill the animal. The penetrating foreign body generally is still present in the wall of the reticulum or pericardium.
Prevention and control
Eliminating sources of sharp foreign objects in the feed supply prevents TRP. Installation of large magnets on feed handling equipment and prophylactic administration of forestomach magnets to all animals at 15 to 16 months of age prevent almost all cases caused by magnetizable objects.
Abomasal Displacement and Volvulus
GiUes Fecteau • Charles L. Guard
■ Etiology Although the precise cause of displacement of the abomasum remains unknown, general agreement exists in veterinary literature that it is a multifactorial syndrome and that abomasal hypomotility is an absolute prerequisite. Abomasal motility can be decreased in many ways. Numerous common disorders of postpartum dairy cattle have been incriminated as possible triggering events to abomasal dilation and displacement. Among the most important, ketosis, low serum calcium levels, hyperinsulinemia, and reduced insulin sensitivity have been studied.
■ Prevalence and Incidence Abomasal displacement occurs either to the right or to the left side of the abdomen when gas accumulates within this viscus. Left-displaced abomasum (LDA) is the more common, accounting for most of the cases. The incidence is highest by far in adult dairy

FIG. 32.134 Schematic view of a right-dilated abomasum. (Courtesy Andre Desrochers, from Surgery of the abomasum in cattle, Version 2.0, Universite de Montreal.)

FIG. 32.133 Schematic view of a left-displaced abomasum. (Courtesy Andre Desrochers, from Surgery of the abomasum in cattle, Version 2.0, Universite de Montreal.)
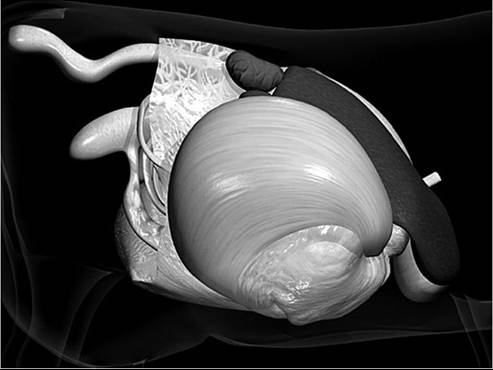
FIG. 32.135 Schematic view of an abomasal volvulus (AV). (Courtesy Andre Desrochers, from Surgery of the abomasum in cattle, Version 2.0, Universite de Montreal.)
cattle in the early postpartum period, but cases have been seen in all other classes of cattle. LDA is probably a worldwide problem. The prevalence among dairy herds is variable, depending on multiple factors such as geographic location, climate, management practices (confinement versus pasture), and feeding practices.
■ Pathophysiology After abomasal atony, distention with gas produced by microbial fermentation occurs and probably precipitates the displacement. It has been hypothesized that the displacement is oriented (left or right) according to the size of the rumen. If the rumen is small and empty (as in the early postpartum period), the abomasum can move to the left, and LDA can occur (Fig. 32.133). If the rumen is large and filled, the left displacement is less likely, and the abomasum dilates and in some cases twists to the right (Figs. 32.134 and 32.135).
■ Surgical Therapy Numerous surgical techniques exist with advantages and disadvantages.7 All techniques have a common objective to create a permanent attachment, usually by suturing either the abomasum or the greater omentum to the abdominal wall. This prevents recurrence. The techniques may be classified into three different broad categories: blind technique, surgical (open) technique, and laparoscopic technique. Another way to consider the different options is to classify the techniques as performed on an animal standing or in recumbency. Multiple factors influence the technique used or recommended for a particular case. Cost and preference of the surgeon are very important. Laparoscopic technique has also been described and studied.8-11
All techniques have been successful when performed adequately. The less invasive techniques have been studied to evaluate the possible advantages over the more invasive open techniques. The advantages are time to perform the surgery, less frequent use of antimicrobials, a shorter interval from calving to first service, and a faster abomasal emptying.12-15 Understanding the limitations of each technique allows the clinician to best serve the patient and client in all situations. Success rates and possible economic advantages of having the procedure performed by herd personnel have been discussed in the literature.16,17
■ Left Displacement of the Abomasum Clinical Signs and Differential Diagnosis
Cattle with simple LDA have a reduced appetite (complete anorexia, reduced consumption of concentrates, or alternating periods of normal appetite and anorexia). Milk production is reduced. Ketosis is usually present, either as a predisposing factor or as a consequence. Feces are often normal to softer than normal but reduced in volume. Rectal temperature is normal, unless a concurrent infectious problem is present (metritis, mastitis). Pulse and respiration rates are normal or slightly above normal, unless a concurrent or secondary problem is present. Ruminal contractions are decreased to absent and difficult to hear because the abomasum interferes with transmission of the sound. It is not unusual to observe the animal ruminating despite the displaced abomasum. The last one or two ribs on the left are sprung, but the abdomen is sunken in the paralumbar fossa. Gurgling or tinkling rather than normal scratching sounds may be heard on auscultation in the left paralumbar fossa. Simultaneous auscultation and percussion reveal a ping over the gas-filled portion of the abomasum. With LDA the area of ping may be anywhere from the lower third of the abdomen in the eighth intercostal space to the paralumbar fossa (see Chapter 1, Physical Examination section). Attention should also be given to the cranial and lower aspect of the flank because in some cases the ping will be audible only in this area. On rare occasions, during rectal examination the clinician may be able to palpate the abomasum to the left of the caudodorsal blind sac of the rumen or at least perceive that the rumen is displaced medially.
Ruminal tympany, pneumoperitoneum, and collapsed rumen may all produce pings on the left side of the cow. Physometra (air in the uterus) and dilation and displacement of the cecum to the left of the rumen (which is rare) may also produce left-sided pings. Having an assistant blow on the stomach tube passed into the rumen while auscultating over the left side helps the clinician differentiate the rumen from other structures. Percutaneous needle aspiration of fluid or gas from the suspected abomasum aids in correct identification. A pH of less than 4.5 as determined with wide-range pH paper or the odor of abomasal gas (slightly acrid or of burned almonds) confirms the presence of LDA. Ultrasound examination could also be helpful in determining the position of the pylorus and to compare the position with the actual normal variation.18
■ Clinical Pathology The most important abnormalities detected by clinical chemical evaluation usually involve the serum electrolyte levels, acid-base levels, and liver metabolism and integrity. Sequestration of the hydrochloric acid secreted into the abomasum or by means of reflux in the ruminoreticulum may occur and lead to metabolic alkalosis. The blood pH and bicarbonate concentration are slightly elevated, with a concomitant small decrease in the blood chloride concentration. Ketosis is common, and liver enzyme levels are often elevated, reflecting a degree of hepatic lipidosis.6,19,20 The serum calcium level may be below normal as a result of decreased intake and absorption. Hypokalemia may develop as a consequence of both the metabolic alkalosis and reduced intake and absorption. Cattle with LDA tend to be hypophosphatemic.21
CBC analysis may reveal a mild dehydration and a stress leukogram. If LDA is combined with bleeding abomasal ulcers, it may produce severe anemia. The presence of a concurrent disease may lead to specific changes (e.g., left shift with acute coliform mastitis). The peritoneal fluid of cows with abomasal displacement reveals changes compatible with ischemia and
22
inflammation.22
■ Epidemiology Cows in early lactation (particularly the first month) are at greatest risk of developing LDA. The overall incidence is highly variable among herds and related to nutrition program and associated problems. Retained placenta, metritis, and increased serum concentration of β-hydroxybutyrate were associated with a greater risk for LDA.3 Cows identified with subclinical ketosis early in lactation (3 to 5 days in milk) were 6.1 times more likely to develop an abomasal displacement than were cows affected later in lactation.1 A serum β-hydroxybutyrate concentration above 1200 pmol/L in the first week after calving were associated with an increased risks of subsequent abomasal displacement (odds ratio, 2.6).2 On a herd basis, in one study in Sweden, large herd size, high maximum daily milk yield, keeping dry cows in one group, and not cleaning the feeding platform daily appear to be risk factors associated with a high incidence of abomasal displacement or clinical ketosis.23 The same research group also demonstrated that high-incidence herds have a lower metabolic index and a higher incidence of ketosis than do low-incidence herds.5 The metabolic index used was the revised Quantitative Insulin Sensitivity Check Index (RQUICKI). Genetic factors may also play a role in the predisposition to LDA. Fox suggested that body depth had increased in dairy cattle since 1945 and that this may provide more room for the relatively empty abdominal viscera to move more freely at parturition.24 More recently, cows selected for large body size had significantly greater health costs, related mostly to the greater incidence of LDA.25 Also, the depth of the abdomen and the vertical distance between the ventral abdomen and the descending duodenum were greater in cows with a previous history of LDA than in the controls.26 Some evidence exists to support a genetic basis for predisposition to LDA, and perhaps this is mediated through body size or conformation.
■ Treatment and Prognosis Treatment of LDA involves returning the abomasum to its normal anatomic location and preventing recurrence (abomasopexy); treating the electrolyte and acid-base abnormalities and the energy metabolism problems (ketosis and hepatic lipidosis); and providing therapy for concurrent diseases. The prognosis for animals with LDA is good but is influenced by the severity of the concurrent disease. Cattle with severe hepatic lipidosis and LDA should be given a guarded prognosis because their recovery is often slow and incomplete. Also, some cattle develop LDA as a consequence of gastrointestinal malfunction. As an example, LDA could be diagnosed in an animal suffering chronic indigestion. The prognosis of this group of cattle is poor because the primary disease is often more serious than the LDA per se.
■ Prevention and Control The incidence of LDA has been reduced in problem herds by dietary manipulation that reduces the likelihood of forestomach and abomasal atony caused by high-concentrate rations. This includes slow introduction of concentrates after calving, prepartum introduction of ensiled and concentrate feeds, and increase in the particle size of the forage. Maintaining serum calcium concentration at the time of parturition and reducing subclinical ketosis early in lactation are of particular importance. Dietary cation-anion difference is a reliable guideline for controlling hypocalcemia in dairy cows (see Chapter 41).
Right Displacement of the Abomasum
Simple right displacement of the abomasum (RDA) occurs at approximately 10% to 15% the frequency of LDA.
■ Clinical Signs and Differential Diagnosis The general systemic state of cows with a simple RDA is the same as that of cows with LDA. On the other hand, as simple RDA evolves toward the volvulus, the systemic changes observed in cattle with abomasal volvulus progressively appear. An area of tympanitic resonance is heard on the right side with simultaneous auscultation and percussion. The ping usually is confined to an area under the last five ribs in the upper half of the abdomen. The condition must be differentiated from other causes of right-sided pings, such as cecal distention (with or without volvulus), gas in the spiral colon, pneumorectum after rectal examination, pneumoperitoneum, physometra (gas in the uterus), signoid flexure volvulus, and abomasal volvulus. Cecal and rectal pings usually are detectable in a linear pattern just below the transverse processes of the lumbar vertebrae extending to the tuber coxae (see Chapter 1, Physical Examination section). Rectal examination identifies the gas-filled structure. Pings heard with gas in the spiral colon typically have a variable pitch, depending on the location over the cranial paralumbar fossa and last three or four ribs. In general, the spiral colon may be palpated rectally as a laterally flattened, mildly distended viscus adjacent to the right body wall. Gas in the uterus can be detected on rectal palpation. Pneumoperitoneum creates a ping that is distributed all along the dorsal portion of the abdominal cavity and is usually heard on both sides.
Abomasal volvulus is the condition most difficult to differentiate from RDA. Determination of the difference by physical diagnosis in an early case of abomasal volvulus is probably impossible. With time affected cows become progressively more dehydrated and more severely ill with volvulus than is usual with RDA. Rapid heart rate (>100 beats/min), total absence of ruminal motility, and almost no fecal output are clinical signs in favor of a diagnosis of abomasal volvulus. Advanced cases of volvulus also produce a ping that reflects an arched dorsal border and a horizontal ventral border caused by the fluid level in the abomasum. This fluid is auscultable on succussion of the abomasum. Even with ultrasonography in one study to determine positions of the liver, omasum, and small and large intestines, the two conditions could not be
27
distinguished from one another.
■ Treatment and Prognosis Surgical treatment is necessary to correct RDA. Because of the difficulty of differentiating RDA from early volvulus, intervention should be as prompt as possible. The prognosis for a successful recovery after surgery is comparable with that for LDA if no other concurrent disease is present.
Abomasal Volvulus
Abomasal volvulus, or right torsion of the abomasum, leads to complete obstruction of the flow of ingesta into the duodenum and is therefore a surgical emergency. The condition occurs in all classes of cattle. Although RDA is thought to precede its development, unknown factors lead to abomasal volvulus.
■ Clinical Signs and Differential Diagnosis The systemic effects of the gastrointestinal obstruction that results from abomasal volvulus progress to a much more severe degree than in LDA or RDA. Sunken eyes and loss of skin turgor accompany the dehydration that develops. The heart rate increases above 100 beats/min, and the pulse is weak and thready. Abdominal distention is marked bilaterally. Complete ruminal stasis develops, which leads to bloat, and the abomasum greatly enlarges on the right. Despite the severe degree of gastric distention, colic rarely develops in cattle with abomasal volvulus; it is much more likely to occur with cecal distention. The skin is cool to the touch. Feces are absent or watery but scant. A large area of tympanitic resonance with uniform pitch throughout is detectable on the right, extending from the eighth rib to the middle of the paralumbar fossa. The ventral border of the ping is a horizontal line reflecting the fluid level in the greatly distended abomasum. Borborygmi is absent. Splashing fluid sounds can be heard when the abomasum is ballotted (succussed) behind the last rib.
Other causes of proximal intestinal obstruction and torsion of the intestinal mass around the root of the mesentery must be differentiated from abomasal volvulus. On rectal examination the abomasum can usually be palpated with abomasal volvulus. With intestinal obstruction or intestinal volvulus, distended loops of small intestine can be palpated. Pings caused by gas in the intestines have a variable pitch over the areas involved. Cecal distention with rotation can produce a similar degree of abdominal distention high on the right, but the abdomen usually is less filled cranioventrally on the right. A ping extends to the tuber coxae, and the cecum can be palpated rectally. Diffuse peritonitis leads to complete atony of the gastrointestinal tract, and the abdomen may become distended with gas in all parts of the tract; there is no discrete ping extending over a large area of the right side. As abomasal volvulus progresses, cattle become recumbent and depressed. Death occurs within hours in this stage, which occurs 1 to 3 days after the development of the volvulus.
■ Clinical Pathology The serum biochemistry profile shows much more dramatic changes with abomasal volvulus than with RDA or LDA. Clinicopathologic consequences include hypovolemia, dehydration, hemoconcentration, metabolic alkalosis, hypochloremia, hypokalemia, and paradoxic aciduria. Hyperglycemia, hypocalcemia, and hyponatremia may also be observed. Later in the condition a superimposed metabolic acidosis is also present. Anion gap gradually increases with the severity of the disease. Systemic shock eventually causes fatality. Reduced fluid intake and sequestration of large quantities of chloride-rich fluid in the stomachs (third space problem) leads to dehydration and hypovolemia. Hyperphosphatemia was also observed, possibly as a consequence of decreased renal blood flow.21
Under the influence of carbonic anhydrase, hydrogen ions are normally pumped into the abomasal lumen. A chloride ion follows into the lumen, whereas bicarbonate and sodium remain in the blood. Under normal circumstances, the hydrochloric acid leaves the pylorus, where the hydrogen ions are neutralized by pancreatic and intestinal secretions and the chloride is resorbed. When abomasal volvulus occurs, the hydrochloric acid is sequestered in the abomasum and regurgitated into the omasum and rumen (internal vomiting). Ruminal chlorides increase. The animal becomes alkalotic and hypochloremic. Because of shifts between intracellular and extracellular compartments, potassium moves intracellularly as hydrogen ions move extracellularly in response to the metabolic alkalosis. This, plus the total anorexia, leads to severe hypokalemia. The hallmarks of abomasal volvulus are metabolic alkalosis, hypochloremia, and hypokalemia.
Paradoxic aciduria occurs in the presence of metabolic alkalosis, when a cow should be retaining hydrogen ions. The overwhelming renal physiologic drive appears to be sodium retention. Dehydration and reduced cardiac output result in falling blood pressure. The animal must respond by volume expansion; thus sodium is resorbed in the renal tubules. Chloride is also resorbed. Because there is hypochloremia, the electrical gradient that must be corrected is high; if 140 mEq/L of sodium is resorbed and only 60 mEq/L of chloride is available, there is a net of 80 mEq/L (140 - 60) of cations that must be secreted back into the tubules. This is normally accomplished by secretion of potassium. Because hypokalemia is severe, hydrogen ions are paradoxically secreted to retain electrical neutrality so that blood pressure can be maintained by means of maximum sodium resorption.
Peritoneal fluid of cattle with abomasal volvulus has been studied.22 In comparison with cows with a diagnosis of LDA, cows suffering from abomasal volvulus had significant changes in their peritoneal fluid parameters. Total protein, albumin, L-lactate, CPK, ALP, lactate dehydrogenase, and D-dimer levels were increased, whereas fibrinogen level was decreased. Also, a higher percentage of apoptotic and necrotic neutrophils was detected despite the fact that total leukocyte count was not significantly different. At least in one study, evidence of abnormal coagulation profile reflecting possible disseminated intravascular coagulation was present in a small proportion of cattle studied (3 of 10). Hemostatic dysfunction could be present in advanced stages of the disease.28
■ Pathophysiology At least some of the factors predisposing to LDA or RDA probably contribute to the development of abomasal volvulus. Whether true RDA precedes abomasal volvulus is not known. Dissection of naturally occurring cases of abomasal volvulus demonstrated that the structures involved in rotation can vary from the reticulum to the omasum at the orad end. The rotation probably occurs most frequently at the reticuloomasal junction. The duodenum is looped around the omasum, regardless of the degree of volvulus. The ensuing displacement leads to a counterclockwise rotation of the abomasum and omasum as viewed from the right side and the rear. The duodenum is pulled medial to the body of the omasum and wraps around the neck of the omasum in the final configuration. The continued hydrochloric acid secretion of the abomasum and the gas produced in the omasum and abomasum further stretch and occlude the duodenum. The abomasal blood vessels and the ventral vagal trunk are compromised near the site at which the duodenum wraps around the omasum in long-standing cases. Thrombosis of vessels may occur.
The acid-base and electrolyte abnormalities of early abomasal volvulus are the same as those of LDA. In cases of severe distention of the abomasum and omasum with vascular compromise, systemic cardiovascular insufficiency develops. Reduced perfusion of peripheral tissues may lead to metabolic acidosis terminally. Hemoconcentration develops, although bleeding into the abomasum may occur from devitalized mucosa, which lowers the hematocrit. These changes are compounded by the developing necrosis of the abomasum. The abomasum may physically leak contents through a weakened, overstretched wall. Endogenous inflammatory mediators and bacterial toxins may diffuse from the abomasum to viable surrounding tissues, where absorption occurs. In either case, the viability of the abomasum is lost, and death follows shortly. At least in a sheep model of abomasal volvulus, ischemia and reperfusion injury occur.29
■ Treatment Immediate surgical intervention usually is necessary to save the animal's life. At the same time, fluid, electrolyte, and acid-base abnormalities must be corrected. For early cases of hypokalemic, hypochloremic alkalosis and dehydration, intravenous fluids consisting of 20 to 80 L of 0.9% sodium chloride with 25 to 100 mEq/L potassium chloride added are administered. Intravenous potassium should not be given at a rate greater than 1 mEq/kg/h to prevent cardiotoxicity. If the serum potassium level is unknown, it is best to stay with an IV rate of less than 0.5 mEq/kg/h. For advanced cases with metabolic acidosis, balanced electrolyte solutions such as Ringer's solution are indicated. Broad-spectrum antibiotics are appropriate if the integrity of the abomasal mucosa is questionable. NSAIDs are indicated to control pain, inflammation, and shock. Both standing right-sided and recumbent right paramedian approaches have been successful for correcting abomasal volvulus. There may be less cardiopulmonary compromise if the animal remains standing, especially if reperfusion injury is suspected.
■ Prognosis Establishing an accurate prognosis before surgery would be optimal because at that time salvage remains a possibility and little expense has been incurred. It is not a simple task. A second critical time is shortly after surgery in cows suspected of not fully recovering. The decision will be whether to continue to treat (cost) or salvage, if that still is an option.
Preoperative assessment is difficult. In the author's experience, assessment cannot be based on a single clinical observation or serum biochemistry value. In the best published studies, investigators examined two different classifications of outcome: death versus survival and productivity versus nonproductivity. A logistic regression model of heart rate, base excess, and serum chloride level was developed as a preoperative predictor of death or survival.30 Constable and colleagues found that four presurgical variables (hydration, heart rate, duration of inappetence, and pelvic alignment level) could be used to best predict cattle as productive or nonproductive after surgery.31
Assessment of outcome after surgery has been investigated. The overall success rate of surgery varies between 61.5% and 86.3%.32-35 The number of forestomachs involved in the twist has been found to adversely affect survival and productivity. Wallace found only 20% success in cattle with reticuloomasal- abomasal volvulus.35 Another study demonstrated success in 55% of cattle with omasal-abomasal volvulus and 87% success in cattle with only an abomasal volvulus.31 Edema of the abomasum carries a guarded to poor prognosis.35-37 Edema around the proximal duodenum was associated with a poor outcome in Pearson's study, but Fubini and coworkers found no association with outcome.36,38 Purple discoloration of the abomasal serosa tends to bode poorly for long-term outcome, as does severe distention of this organ, abomasal necrosis, and thrombosis of the gastric veins.30,35 The measurement of intraluminal pressures of greater than 16 cm Hg also carries a poor prognosis because of mucosal damage.31 A logistic regression model of some of the surgical findings did not predict outcome any better than did the preoperative model.30
After surgical correction, cattle with abomasal volvulus often have diarrhea for 24 hours. Feces then firm up to normal consistency. Postoperative clinical signs associated with a poor prognosis include melena, anorexia, persistent tachycardia, and dehydration.33,37,39 In the author's experience, even if appetite and general attitude are initially good (24 to 48 hours after surgery), persistence of a loose low-volume stool 72 hours after surgery may indicate complications.40 Among animals in which clinical signs compatible with chronic indigestion develop, the survival rate is only 11. 5% to 20%.35,41 Prolonged treatment seems irrelevant. Prokinetics and their possible benefit in postoperative care have been studied and reviewed.42,43 Erythromycin (10 mg/kg) IM given preoperatively improves abomasal motility in cattle suffering from abomasal volvulus.
■ Necropsy Findings Cattle that die of abomasal volvulus are grossly dehydrated, and the abomasum is severly distended or ruptured. The omasum often is also distended when torsion occurs at the reticuloomasal junction. Affected cattle that die or are euthanized after developing postoperative complications have one or more of the following postmortem lesions: gastric compartment dilation, peritonitis, abomasal wall necrosis or ulcer, vascular thrombosis, or vagal nerve lesions.40
■ Prevention and Control Because factors predisposing to atony of the forestomach and abomasum probably are important in the genesis of abomasal volvulus, prevention should be similar to that outlined for LDA.
Abomasal Ulcers
■ TABLE 32.20
Abomasal Ulcers
| Type | Lesions | Clinical Signs | |
| 1. | Nonperforating | la. Erosion with minimal mucosal defects sometimes distinguished from the surrounding tissue by mucosal discoloration (often reddish-violet or green-brown) lb. Deeper erosions with focal mucosal hemorrhage, sharply demarcated with a depression in its center lc. Craters with coating of detritus or fibrin, depression in its center, and bulging margins ld. Radial wrinkles with a central point, affecting gastric folds only | Partial anorexia; decreased ruminal motility; positive fecal occult blood |
| 2. | Nonperforating with severe blood loss (bleeding) | Penetration of mucosa and submucosal blood vessel; hemorrhage into abomasum | Partial anorexia; decreased ruminal motility; anemia; pale mucous membranes; melena; tachycardia; cool extremities |
| 3. | Perforating with local peritonitis | Penetration from mucosa to serosa; leakage of abomasal contents; localized peritoneal reaction with adhesion formation | Total anorexia; low-grade fever; ruminal motility decreased or absent; localized abdominal pain; very similar to traumatic reticuloperitonitis |
| 4. | Perforating with diffuse peritonitis | Penetration from mucosa to serosa; widespread contamination of the peritoneal cavity with abomasal contents; significant exudate in peritoneal cavity; fibrin deposition of all serosal surfaces | Total anorexia; fever early, then hypothermia; ileus of entire gastrointestinal tract; tachycardia; shock; terminal recumbency with grunt on respiration |
hemorrhage.7 Of these, half had lymphosarcoma and, for the most part, were older than 6 years of age. The age of the cattle with nontumor-associated bleeding ulcers was generally younger. In the remaining two-thirds of the cattle, ulcers had perforated, with approximately half having diffused and half having localized peritonitis.8 Most adult cattle with abomasal ulcer are in the first month of lactation after calving and have a concurrent disease. Several cows have been discovered to suffer of an abomasal ulcer during surgery to correct displaced abomasum. Metritis, mastitis, and ketosis are the other diseases commonly seen with abomasal ulcers.
Few data are available in small ruminants. However, the prevalence of abomasal ulcers at slaughter has been reported to be 61% among goats in one old slaughter study from Iran.9 The incidence of abomasal ulcers was reported to be highest in goats severely affected with nematodes.9 In two slaughter studies from the Middle East, the prevalence of abomasal ulcers in healthy sheep ranged from 18%10 to 75%11; almost all of these abomasal ulcers were type 1 ulcers.
■ Etiology and Pathophysiology The specific events leading to erosion and ulceration of the abomasal mucosal epithelium are unknown. Cytoprotective mechanisms include a mucous barrier, cloudy mucus containing bicarbonate ions to neutralize back-diffusing hydrogen ions, and high submucosal rates of blood flow to remove back-diffusing hydrogen ions. When these mechanisms are disturbed, gastric (abomasal) ulcers may occur.
The exact cause of abomasal ulcers is still obscure and may be multifactorial. Hund and Wittek12 reviewed the different suspected causes of abomasal ulcers in cattle and small ruminants. In calves, development of abomasal ulcers was proposed to be associated with mineral deficiencies (mainly copper), stressful management practices, feeding practices (type of milk and frequence of feeding), concomitant diseases, proliferation of microorganisms (C. perfringens type A or D, Escherichia coli, Sarcina-Xike spp., fungi, or others), and abrasion of the abomasal mucosa by roughage, geosediments, or trichobezoars. However, all explored hypotheses have failed to demonstrate involvement of any of these alone in the development of abomasal ulcers. In adult cattle, the disease is associated with stressful events such as recent parturition, peak milk production, presence of concurrent diseases (mainly those of the peripartum period), feeding practices such as diets high in starch, and presence of lymphosarcoma. Finally, abomasal ulcers are an adverse effect of antiinflammatory drug administration.
■ Clinical Signs and Differential Diagnosis Loss of gastric epithelium may range from no clinical signs to hemorrhage and subsequent melena, to peritonitis if the erosive processes penetrate all layers of the abomasum (see Table 32.20).
The mildest form (type 1) is caused by nonperforating ulcers that do not result in extensive hemorrhage. Affected animals may have mild or no clinical sign. Mild abdominal pain, shown by partial anorexia, decreased ruminal motility, and mild ruminal tympany are the possible clinical signs if present. There is usually no fever. Feces may be normal or reduced in amount and stale because of prolonged transit. In some cases, abdominal pain may be evident on manual pressure on the right ventral abdomen. TRP or indigestion may be suspected. In one study, approximately two-thirds of affected cows produced a positive result of a fecal occult blood test measured with the use of an ortholidine-based tablet.13
In cattle with ulcers that erode into major gastric blood vessels (type 2), blood loss can be sufficient to cause signs of anemia and hemorrhagic shock. These animals have dark blood clots in their feces or tarry, black feces with the characteristic smell of partly digested blood. The mucous membranes may be pale, tachycardia and a pounding heart may be pronounced. Respiratory rate may be elevated. Total anorexia and rumen stasis usually are present. The rumen may have a fluid consistency, and if the animal is able to stand, abdominal pain sometimes is evident. There are other possible sources of proximal gastrointestinal hemorrhage in cattle, but abomasal ulcers are by far the most common cause. Among them, bleeding abomasal ulcers must be differentiated from melena sometimes seen with intussusception or hemorrhagic bowel syndrome (hemorrhagic bowel syndrome; see Diseases Caused by Clostridium perfringens Toxins [Yellow Lamb Disease, Lamb Dysentery, Necrotic Enteritis, Enterotoxemia] section). In these cases, feces are usually more the color of blackberry or strawberry jam. The PCV usually is increased with intussusception,14 normal or increased in hemorrhagic bowel syndrome,15-17 and decreased with a bleeding ulcer.18
Abomasal ulcers that perforate the serosal surface may lead to localized peritonitis (type 3) from contamination with abomasal contents. If the lesion is small or the local inflammatory reaction sufficiently swift, localized peritonitis results. This condition mimics the presentation of TRP. The animal may have a moderate fever and partly or totally anorexic. Milk production may decrease acutely. There is evidence of abdominal pain, usually localized to the right ventral quadrant (positive withers pinch test). Ruminal motility is reduced, and mild bloat may be present. As with TRP, the signs usually abate over the course of a few days if the infection is successfully contained. In some cases the infection is confined to the omental bursa, where extensive contaminated fluid (pus) may accumulate. The course of omental bursitis is much more prolonged than that of simple localized peritonitis and usually results in a guarded prognosis.
Major leakage from a perforating ulcer leads to acute diffuse peritonitis (type 4). The course of the disease usually is rapid, with signs of septic shock developing within 24 hours of the onset. Total anorexia and ruminal stasis are accompanied by tachycardia with a weak, thready pulse and a heart rate of more than 100 beats/min. Pain may be evidenced by grinding of the teeth or groaning. The extremities are cool, and affected animals usually become recumbent. Abdominal enlargement may be evident as a result of both ruminal tympany and the accumulation of peritoneal fluid. Dehydration is detectable by skin pinch or by observation of the position of the eye in the orbit. Septic shock from other causes may be difficult to distinguish. Diffuse peritonitis from uterine, cecal, or intestinal ruptures have the same final course. Abomasal volvulus of more than a day's duration has similar characteristics but can be differentiated by the right-sided ping and fluid in the abomasum.
■ Ancillary Tests Antemortem diagnosis of abomasal ulcers may be challenging, particularly in cases of nonperforating and nonseverely bleeding ulcers.
COMPLETE BLOOD CELL COUNT. If peritonitis is present, leukocytosis usually is present, with neutrophilia predominating in many cases. The plasma fibrinogen is increased (>700 mg/ dL) in most cattle with peritonitis. The hematocrit is normal or elevated with peritonitis, but plasma protein levels may be decreased as a result of protein accumulation in the peritoneal cavity or increased if dehydration is severe. If blood loss is severe, the PCV is decreased.
SERUM BIOCHEMISTRY PROFILES AND BLOOD GAS ANALYSIS. Results of a serum biochemistry profile or blood gas analysis are nonspecific. In most cases, they reflect a digestive stasis (hypochloremic metabolic alkalosis), but in animals in shock a metabolic acidosis may be observed. BUN level may be increased. This can be a result of blood degradation in the intestine or hypovolemia and prerenal azotemia. The utility of BUN in the diagnosis of abomasal ulcers by identifying digestive hemorrhage remains to be determined.
OTHER BLOOD TESTS. Serum pepsinogen concentration has been reported to be increased in one study in cases of severe abomasal ulceration.19 Because serum pepsinogen concentration can also be elevated in other abomasal diseases such as nematode infection, this finding is not specific.19,20 Serum gastrin concentration has also been reported to be increased in cases of type 2 ulcers in comparison with healthy cows.21 However, the sensitivity and specificity of this test are not known.
Cattle older than 5 years of age with a bleeding abomasal ulcer should be tested for bovine leukosis virus.
AbdominocenTESIS. Abdominocentesis confirms diffuse peritonitis (a large quantity of abdominal fluid is obtainable); centesis fluid may contain leukocytes with phagocytosed or free bacteria and even feed particles. In localized peritonitis, the results of abdominocentesis may be normal (see Peritonitis in Ruminants section for more details).
FECAL OCCULT BLOOD TEST. Fecal occult blood tests may be helpful for detection of type 1 ulcers. The tests are inexpensive and can be performed during the physical examination. Testing multiple samples may increase its sensitivity.22 However, these test did not provide any information about which part of the gastrointestinal tract is involved in the bleeding. One study have reported a sensitivity of 77% and a specificity of 97% for ulcers confirmed at surgery or necropsy.13 However, the reagent used in this study is not commercially available anymore. Researchers have since evaluated a guaiac test and a urinary test strip for the diagnosis of type 1 ulcers. They reported low sensitivity, low specificity, or both and concluded that these tests are not suitable for the detection of type 1 ulcers.23
DIAGNOSTIC IMAGING. Because of forestomach anatomy, oral endoscopy of the abomasum is not possible in ruminants. Because ultrasonographic assessment of the abomasal mucosa integrity is difficult, ultrasonography is of limited value for the diagnosis of abomasal ulcers. However, images compatible with focal mucosal or omental edema and abdominal effusion associated with abomasal ulcers may be observed and lead to the suspicion of ulcers (Fig. 32.136). Ultrasonographic images of lymphomatous infiltration of the abomasal mucosa has been described in cows with lymphoma.24 Abdominal ultrasonography is also useful for the diagnosis and the evaluation of peritonitis associated with type 3 and 4 abomasal ulcers (see Normal and and Main Abnormal Ultrasonographic Aspects of Abdominal Organs in Calves and Cows section). Braun and colleagues reported that percutaneous ultrasonography-guided abomaso- centesis can be safely performed for the evaluation of abomasal fluid.25 According to the investigators, the presence of blood or hemoglobin is principally associated with abomasal ulcers.
EXPLORATORY LAPAROTOMY. Exploratory laparotomy may also be an alternative in the diagnosis abomasal ulcers by palpation of a thickening of the abomasal wall, roughing of the abomasum serosa, adhesion of the abomasum, or directly
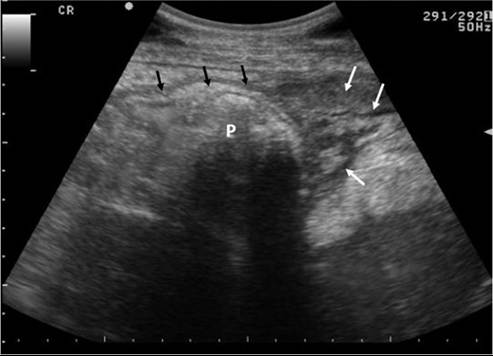
FIG. 32.136 Ultrasonography of the right cranial abdomen of a cow diagnosed with abomasal ulcers. The pylorus (P) is visualized (black arrows). The surrounding images are compatible with inflammatory changes (white arrows, indicating hypoechogenic pocket with structures of various echogenic appearance). (Courtesy Centre Hospitalier Universitaire Veterinaire de PUniversite de Montreal)
a perforation in the abomasal wall. However, potential aggravation after the exploratory procedures should be considered.
■ Treatment Treatment is aimed at correcting dietary problems, reducing stress, treating concurrent diseases, and initiating specific therapy to address the consequence of the ulcers.
SUPPORTIVE TREATMENTS. Removal of high-energy feedstuffs and replacement with good-quality hay combined to confinement in a stall are beneficial.26 The buffer effect of food is very important in controlling the abomasal pH. Consequently, recovering a normal appetite is the main goal of the treatment of abomasal ulcers.27
Blood transfusions may be necessary for cattle that have lost enough blood to lower the hematocrit to 14% or below. Usually 4 to 6 L given once is adequate, but repeated transfusions may be necessary. Crossmatching is usually not necessary in cattle unless repeat transfusions are performed over more than 3 days.
Broad-spectrum antibiotics are administered when peritonitis is suspected. Principles and details regarding the treatment of peritonitis are described in the Peritonitis in Ruminants section. Intravenous or oral fluids may be necessary to treat dehydration and metabolic or acid-base disturbances. Animals with diffuse peritonitis must be given intravenous fluids with caution because of the risk of pulmonary edema associated with the low plasma oncotic pressure.
DRUGS THAT INCREASE THE ABOMASAL PH: ANTIACIDS. Numerous studies have been performed to evaluate the effect of different therapeutic agents on abomasal pH of healthy calves. Results of these studies have been summarized by Constable and colleagues.27 The therapeutic agents studied in normal calves included oral administration of an antacid agent containing aluminum hydroxide and magnesium hydroxide (25 mL and 50 mL, tid), oral administration of specific H2 antagonists (cimetidine, 100 mg/kg and 50 mg/kg, tid; and ranitidine, 10 mg/kg and 50 mg/kg, tid), and oral administration of the proton pump inhibitor omeprazole (4 mg/kg q24h). All these extralabel treatment regimens induce an increase in the mean 24-hour abomasal luminal pH. Oral administrations of aluminum hydroxide agent induced a dose-dependent increase in luminal pH and were more efficacious when administered postprandially. Because some deleterious effects (diarrhea, hypomagnesemia, metabolic alkalosis) were observed when this antacid was administered at the dose of 50 mL tid, this should be considered the maximal dosage in calves. Frequent (every 8h) oral administration of 25 mL of aluminum hydroxide is reported to be the most effective treatment.27 Cimetidine (100 mg/kg tid) was the most effective. However, ranitidine (50 mg/kg tid) was the most cost-effective in these studies. Interestingly, the effect of omeprazole on abomasal pH decreased over time (reduced effect observed after five daily treatments).28 Results of these studies may or may not apply to ill calves. In adults, oral administration of these therapeutic agents is of doubtful benefit because of dilution in the rumen and slow release into the abomasum. Oral medications administered after stimuli that induce esophageal groove closure would be more likely to have the desired effect. Traditional stimuli have included copper sulfate solutions and 10% sodium bicarbonate solution. Vasopressin (0.25 IU/kg IV) was shown to induce reliable abomasal deposition of materials given by drench to adult goats.29
Intravenous administration of H2 antagonists at lower doses may be efficacious, but their use by this route is cost-prohibitive ($100 to $200 per day) or reserved for valuable animals. In the authors' clinic, ranitidine 1 to 1.5 mg/kg IV tid is used; the clinical impression is that this is effective. Intravenous administration of ranitidine (1 and 2 mg/kg) in healthy sheep has shown an increase in the abomasal pH for up to 150 min, and authors conclude that administration of ranitidine at a dosage of 1 mg/kg tid or 2 mg/kg bid IV could be the most effective treatment protocols.30 Intravenous administration of famotidine at 0.4 mg/kg once or tid has also been reported to increase abomasal outflow pH, but the effect decrease with time.31 Injectable proton pump inhibitors (omeprazole, pan- toprazole) are also available in some countries, but their efficacy in cattle and small ruminants is unknown.
SURGERY. Surgery may be an option in cases of perforated ulcers or when abomasal adhesion secondary to a localized peritonitis lead to abomasal dysfunction. Right paralumbar fossa, right paracostal, or right paramedian approaches can be used to access the abomasum (see abomasal impaction) and allow ulcer resection. However, prognosis associated with these surgeries is guard. In calves, 40% of 10 calves survived the corrected surgery in one study32 whereas none survived in another (8 calves, one of which had a nonperforated ulcer).33 In another study in cattle with concurrent abomasal displacement and perforating ulceration, the short- and long-term survival rates were 38% and 14%, respectively.34
■ Prognosis The prognosis is good for ulcers that are neither bleeding nor perforated. For animals that stop bleeding and those with localized peritonitis, survival and eventual return to normal function are possible. Many dairy cattle stop lactating during the acute course of the illness and do not return to milk until the next lactation. Because abomasal ulcers generally occur within the first month after calving, most of these animals are used for slaughter. Most cattle with diffuse peritonitis (type 4 ulcers) die despite aggressive specific therapy. Cattle with ulcers that occur secondary to lymphosarcoma should be euthanized.
■ Necropsy Findings Cattle with bleeding abomasal ulcers resulting in death are very pale and may have blood or bloody fluid throughout the distal gastrointestinal tract. The lesion in the abomasum is typically small and involves an abomasal blood vessel in the submucosa. Most bleeding and perforating ulcers were found in the fundic portion of the abomasum in the region of the proper gastric glands. The most ventral portion of the abomasum in its normal position is frequently affected.18 Most affected animals have a single bleeding ulcer, but approximately 60% have one or more additional ulcers or erosions.18 Cattle with diffuse peritonitis have many liters of foul-smelling fluid in the peritoneal cavity. Fibrin usually covers the serosal surface of all abdominal organs. The defect in the serosal surface of the abomasum is usually nearly round and 3 to 6 cm in diameter. Abomasal fluid freely enters the peritoneal cavity. Omental bursitis may be present, with the omental recess filled with purulent to fibrinous fluid. In these cases, the remainder of the abdomen may not be grossly affected. Asymptomatic abomasal ulcers (often 50 to 200) may be found coincidentally in cattle that die of septic metritis or mastitis. These ulcers generally produce no signs of hemorrhage and go undetected until necropsy.
■ Prevention and Control Because the exact cause of development of abomasal ulcers is unknown, prevention is difficult. Dietary management that reduces other abomasal diseases likewise reduces the incidence of abomasal ulcers. Avoiding abrupt changes in rations and including adequate fiber sources of sufficient particle size to facilitate normal ruminal function also promote normal abomasal function. Minimizing stress caused by overcrowding, excessive competition, and adverse environmental conditions and minimizing mastitis and metritis should also reduce problems with abomasal ulcers. Removal of animals infected with the bovine leukosis virus from the herd eliminates lymphosarcoma as a cause of abomasal ulcers. Judicious use of corticosteroids and NSAIDs is also important.