Peritonitis in Ruminants
Gilles Fecteau
Despite the frequency with which peritonitis is suspected, it remains a frustrating disease for all food animal clinicians. A presumptive diagnosis is often based on clinical signs and history and rarely confirmed by ancillary tests.
If response to therapy is satisfactory, the clinician may never confirm the diagnosis or the precise cause.Review of the Peritoneal Cavity
HISTOLOGY. The peritoneal cavity is lined by a serous membrane composed of two layers called the peritoneum. The deeper layer (subserosa) is composed of loose connective tissue containing collagen, fat and, reticular cells, and macrophages. Covering that layer is a single-surface layer of mesothelial squamous cells (serosa). On the surface of the diaphragm, special lymphatic collecting vessels are located under the mesothelial basement membrane. Small stomata are found between mesothelial cells. They act as channels for lymphatic drainage from the peritoneal cavity to the thoracic duct.
NORMAL PERITONEAL FLUID. The peritoneum acts as a bidirectional semipermeable barrier to the diffusion of water and low-molecular-weight solutes between the blood and the peritoneal fluid. Peritoneal dialysis is based on this principle. Normal peritoneal fluid provides lubrication for the movement of abdominal organs and apposed peritoneal surfaces. It is formed and resorbed constantly. Normal fluid movement is achieved by movement of the viscera and contraction of the diaphragm during respiration. A normal animal has no more than 1 mL of peritoneal fluid per kilogram of body weight.1 In acute severe peritonitis, the inflammatory process may induce a net flow of liters of proteinaceous fluid (80 mL/kg/day in humans), which leads to hypoproteinemia, hypovolemic shock, or both.2
Several authors have described normal peritoneal fluid values.3-10 Each study should be appraised for its strengths and weaknesses and conclusions drawn accordingly.
Later, in the diagnostic section, the author shares his personal experience with interpretation of peritoneal fluid in cattle.Pathophysiologic Mechanism of Diseases in the Peritoneal Cavity in Response to Injury
HEALING. Peritoneal regeneration and healing can occur by reperitonealization or creation of an adhesion with an adjacent nearby mesothelial surface. This adherent type of healing occurs more frequently if the inflammation is severe, with presence of bacteria, foreign material, or both.
HOST DEFENSES AGAINST PERITONEAL INFECTION. The first mechanism of defense is physical removal of the bacteria. The second mechanism relates to the response to noxious stimuli. This intense acute inflammatory response includes degranulation of peritoneal mast cells with release of vasoactive substances. This creates a net influx of fluid rich in complement and serum opsonins that can bind to the bacteria. Third, the omentum contributes to the defense mechanism by adhering to an area that is infected or damaged, or both, to wall off the problem site. Finally, the rapid movement of neutrophils and later, of macrophages is also an important mechanism of control of infection.
ADHESIONS. Adhesions are fibrinous or fibrous bands that create an abnormal attachment of two or more surfaces that should be moving freely against each other. Formation of adhesions is part of the healing process and should be interpreted as an effort to control an injury. The omentum is often involved in adhesions and acts as a natural sealing device to control the acute phase of inflammation. Whole blood potentiates adhesion formation by providing more fibrinogen. Adhesion may or may not be reversible, depending on the amount of organization that takes place in the process. Adhesions that are cut or broken usually rapidly re-form. As the fibrin deposition process is replaced by capillaries and fibroblasts, the adhesion becomes solid fibrous tissue. The three major elements responsible for dissolution of the fibrinous adhesions are (1) adequate oxygen and nutrient supply for the mesothelium, (2) liberation of plasminogen-activating substance by mesothelial and submesothelial cells, and (3) control of the inflammatory process.2 Mechanical obstruction to the normal flow of ingesta and subsequent development of bowel obstruction are major undesirable side effects of adhesions.
■ Peritonitis
Definition and Etiology
Peritonitis is an inflammatory process involving the peritoneal cavity and its serosal surface, the peritoneum. Peritonitis is not truly synonymous with intraabdominal infection because the latter is defined as an inflammatory response of the peritoneum to microorganisms and their toxins that results in purulent exudates in the abdominal cavity. Peritonitis should be considered as the localized equivalent of SIRS, whereas intraabdominal infection is the localized equivalent of sepsis. Intraabdominal abscess is an intraabdominal infection confined within the abdominal cavity. Because most often in farm animals peritonitis is caused by bacteria, the two terms are often used as synonyms. The peritoneal inflammation may result from trauma, surgery, or vascular damage associated with an intestinal obstruction or an accident or from gastrointestinal ulceration (Box 32.7). Peritonitis is a serious and complex process that is often accompanied by various degrees of abdominal pain, changes in gastrointestinal motility, progressive signs of hypovolemia and septicemia, and endotoxemia.
■ Classification Peritonitis may be classified according to the clinical presentation, the cause, or both. Clinically relevant classifications include acute versus chronic, septic versus chemical, localized versus generalized, and primary versus secondary. Although classifying types of peritonitis is useful, it is imperative to recognize that it is a dynamic process. An apparently localized nonseptic peritonitis can evolve into a more diffuse septic process if the primary cause is not resolved.
■ Pathophysiology After peritoneal injury or contamination, mesothelial cells initiate an inflammatory response, modifying the permeability of the peritoneum and its vascular supply. Then several blood constituents move into the peritoneal cavity. Macrophages and polymorphonuclear cells, humoral opsonins, natural antibodies, serum complement, and a proteinrich fluid are the most important.
The inflamed peritoneum also becomes more permeable to toxins, allowing them to be absorbed into the bloodstream. Although this initial response is beneficial to the organism, it induces several systemic abnormalities that the clinician must recognize and treat adequately.Hypovolemia, hypoproteinemia, bacteremia or septicemia, and toxemia are commonly observed in acute diffuse septic
■ BOX 32.7
Causes and Examples of Peritonitis in Approximate Order of Frequency
Traumatic Perforation
Traumatic reticuloperitonitis Septic abdominal surgery Vaginal perforation during coitus Penetrating wound
Visceral Rupture
Perforation of abomasal ulcer
Perforation of ulcer in other part of gastrointestinal tract (oak toxicity of other cause)
Abomasal rupture after torsion
Small intestinal rupture after volvulus, strangulated hernia, or intussusception
Bladder rupture secondary to urolithiasis Spontaneous uterine rupture during gestation or dystocia
Abscess Formation and Possible Intraabdominal Rupture
Reticuloperitonitis, localized
Liver
Umbilicus
Perimetritis
Pyelonephritis
Iatrogenic
Intraperitoneal injection of irritant solution or contaminated solution
Uterine rupture during dystocia Perforation of the uterine wall with a pipette Rectal tear secondary to palpation
Miscellaneous
Hematogenous with systemic infection: tuberculosis, septicemia Fat necrosis
peritonitis. The major adverse effects of peritoneal contamination are (1) rapid clearance of bacteria, which leads to the development of endotoxemia, bacteremia, or both; (2) rapid influx of fluid rich in protein, which leads to hypovolemia and hypoproteinemia; (3) deposition of fibrin, which occludes lymphatic drainage and thus contributes to abdominal distention and enhances the chance of abscess formation; (4) ileus; and (5) adhesion formation, which may lead to obstruction.
■ Clinical Signs and Diagnosis Clinical signs are often nonspecific but suggestive of gastrointestinal dysfunction.
Severity of clinical signs ranges from mild recurrent discomfort caused by a localized abscess to an acute severe onset of toxemia and hypovolemia that lead rapidly to death after the sudden rupture of a viscus. Cattle suffering from acute peritonitis tend to show more characteristic signs. As the condition becomes less acute, the ability of the bovine to seal the infection will attenuate the clinical signs. Chronic but active peritonitis remains to this day a very difficult diagnosis to make without ancillary tests. Abdominal rigidity and tenderness, abdominal distention, scleral injection, fever, anorexia, and sudden reduction in milk production are classic findings but not pathognomonic of acute peritonitis. In the acute stage, abdominal pain and the release of catecholamines often lead to a complete gastrointestinal stasis and ileus. The rumen is then completely atonic. Feces are abnormal in quantity and quality. In the acute stage, feces are present in small amounts and often dry. In more chronic cases, feces are present with a tendency to be diarrheic.Pain, decreased plasma volume, and endotoxemia often result in persistent tachycardia. Anterior abdominal pain, evaluated by the withers pinch test, may be difficult to interpret. The withers pinch test is based on the normal reflex of the bovine to drop its back when the withers and back are pinched (ventroflexion). Cattle with anterior abdominal pain may be reluctant to ventroflex on withers pinch. The sensitivity of this test can be increased by simultaneous auscultation of the trachea during the manipulation. Production of an expiratory grunt during ventroflexion is considered a sign of pain. Cranial ventral pressure with the fist, knee, or some other external force (transverse pole under the abdomen) just behind the xyphoid process can help identify the presence of pain (expiratory grunt) and even localize it in some cases. The author believes that one of the most reliable clinical signs of abdominal discomfort in cattle is reluctance to move.
Scleral injection, fever, tachycardia, gastrointestinal stasis, and distention are the clinical signs that should be monitored to evaluate peritonitis.■ Ancillary Tests Hematologic findings associated with peritonitis range from completely normal hemogram results to severe leukopenia with degenerative left shift and presence of toxic neutrophils, depending on the severity of the peritoneal contamination. In severe cases, variations observed reflect the degree of sepsis and toxemia. PCV tends to increase as plasma/ proteins decrease. In less severe cases, neutrophilic leukocytosis and hyperfibrinogenemia are often present. Hematologic analysis has been a useful tool for monitoring response to therapy. Plasma fibrinogen concentration is also evaluated to monitor the progress of a particular case.
The blood chemistry profile is rarely altered by peritonitis in a way that is diagnostically useful. Chronic inflammation causes a marked increase in serum proteins, particularly the globulin portion. In acute severe cases, secondary findings may include increased serum urea nitrogen and creatinine levels, mildly increased liver enzyme levels, reduction in total CO2, and strong ion difference and reduction in serum albumin level. Ileus and upper gastrointestinal stasis may result in marked hypochloremia and alkalosis.
In the author's experience, abdominocentesis followed by cytologic examination of the peritoneal fluid is a useful aid in making a definitive diagnosis of peritonitis. The technique is simple and safe. The right side just cranial to the udder is the preferred site (to avoid stomach and omentum; Fig. 32.130). A needle, a blunt teat canula, or a bitch catheter and scalpel blade may be used with success (Fig. 32.131). Because of bulls' heavy fascia, a needle is preferable. Failure to secure fluid is common and should be interpreted with caution (because fibrinous peritonitis with fluid loculation is common). More than one site should be attempted if no fluid is secured on the first attempt.
Interpretation of values and what is considered normal appears difficult when the entire literature is searched.3-5,11 Some authors have tried to establish better reference values for cattle.10 Unfortunately, the range seems extremely wide even in the normal cattle population. The authors have been using certain criteria over the years on the basis of some older literature and personal experience: Normal fluid is clear and often in small quantity. Ease in collecting a large amount of fluid should arouse suspicion. A sanguineous fluid leads to suspicion of a compromised bowel problem (e.g., intussusception). A cloudy fluid is more indicative of peritonitis. Any foul smell is enough to conclude that septic peritonitis is occurring. Cytologically, the total number of cells is not as important as the differential. More than 50% neutrophils is suggestive of a septic process. The protein concentration should be less than 30 g/L (publications have moved the cutoff value higher than this number). No bacteria should be visualized. After exploratory
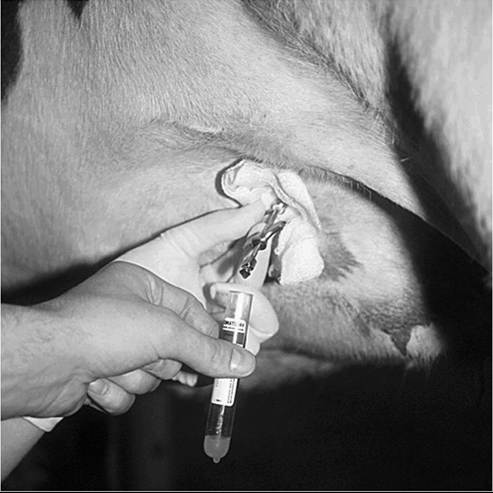
FIG. 32.130 Site of caudal abdominocentesis.
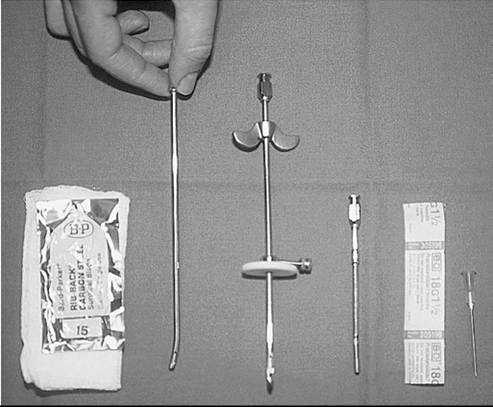
FIG. 32.131 Material used to perform abdominocentesis of bovines.
celiotomy and omentopexy on normal cattle, peritoneal fluid has increased specific gravity, total protein, and WBCs for at least 6 days, even without any peritonitis.12 Because of the bovine's ability to deposit fibrin and seal areas of the peritoneal cavity, the interpretation of peritoneal fluid analysis applies only to the immediate area that was sampled. Results of a caudal tap can mislead the clinician into concluding that a nonseptic process is occurring, when in fact a septic process has already been sealed by the fibrin deposition in the cranial abdomen.
Abdominal radiographs obtained with a high-power unit are extremely useful in cases in which TRP is suspected. They have limited value in other causes of peritonitis. Ultrasound examination is useful for assessing the size and anatomic relationships of lesions, particularly when considering drainage, aspiration, or surgical exploration of a mass surrounding vital structures (see Ultrasonography of the Ruminant Abdomen section). Knowledge of the underlying anatomy is important to prevent misinterpretation. Recognition of free abdominal fluid is easily accomplished by ultrasound examination, and it is also useful for guiding a peritoneal tap. Areas that should be scanned include the caudal lower flank area (right and left), right perirenal area, liver, abomasum and pylorus, and right paramedian area. During exploratory surgery, ultrasonography can be used to image an internal mass or a viscera that appears abnormal. Intraoperative ultrasonography is performed by placing the probe in a sterile sleeve filled with ultrasound gel.
Surgical exploration is often used to confirm or rule out an intraabdominal problem. Information obtained from physical examination and laboratory data is often indicative of a diagnosis but does not provide a specific cause. Cattle are particularly amenable to exploratory surgery, as the procedure is performed when they are standing and is not often associated with complications. Advances in minimally invasive surgical technique in cattle are promising. Laparoscopy can be used to diagnose acute and chronic peritonitis, which is otherwise difficult to identify with ultrasonography or abdominocentesis. It is easier to evaluate the extent of the lesions with the organs in situ.
■ Treatment The basic elements of therapy are support, antibiotics, and surgery.
SUPPORTIVE THERAPY. Depending on the severity of the process, the patient may be in shock. Large volumes of isotonic intravenous fluids and correction of any acid-base deficit are indicated. Electrolyte abnormalities (hypokalemia and hypocalcemia) should be identified and corrected. If the animal is hypoproteinemic, plasma or whole blood transfusions may be beneficial. NSAIDs or steroidal antiinflammatory drugs, or both, may be of importance to prevent the synthesis of more inflammatory mediators. Pain control is also important. Transfaunation with normal rumen fluid may be beneficial in cases of prolonged anorexia.
ANTIBIOTIC THERAPY. Systemic antibiotic therapy should be instituted as soon as a decision to treat is made. Until results of culture and antimicrobial susceptibility become available, a broad-spectrum antibiotic should be used. The choice should take into consideration the following: cost of treatment, permitted use and withdrawal periods in food animals, spectrum of activity, and treatment regimen (frequency and route). Tetracycline or a β-lactam antibiotic (third-generation cephalosporin or a synthetic penicillin) appears to be a good choice. Diffusion into the peritoneal cavity is not a major limiting factor because the permeability of the peritoneum is always increased in peritonitis. However, when fibrin becomes organized and forms multiple small pockets of infected peritoneal fluid, diffusion becomes more problematic. Duration of therapy is empirical in bovines. The author and colleagues normally recommend at least 1 week of intravenous therapy, followed by another week of intramuscular therapy. Some clients elect to have their animals undergo the 2 weeks of therapy in the author's hospital, and the animals are maintained on intravenous antimicrobials.
SURGICAL THERAPY. Surgical control of peritonitis includes peritoneal debridement, irrigation, and drainage. With ultrasound guidance, it is possible to safely establish drainage from the abdominal cavity. A thoracic chest trocar can be used temporarily until all fluid has been removed.
The concept of abdominal lavage during surgery was adopted by human surgeons at the beginning of the twentieth century, and it has been accepted as a part of the treatment of peritonitis since then with fluctuating support.13 Although the principle of removal of any gross contamination is not in question, the level of aggression with which clinicians should institute abdominal lavage during surgery is still open to debate in human and veterinary literature. There is evidence of a negative effect of lavage on the mesothelial cells, the peritoneal defense mechanisms, and the risk of spreading the infection.13 The solution used to irrigate is also under debate. There is no significant advantage to adding antibiotics to the lavage solution, and controversy exists regarding the possible advantages of adding an antiseptic.13 In bovines, large amounts of fibrin may be deposited in a short period of time; in combination with the omentum, this makes drains plug and become rapidly ineffective.
■ Prognosis The ultimate outcome of a bacterial peritonitis episode is determined by many factors, some of which are controlled by the clinician. The early decision on treatment (medical and surgical), correct choice of antimicrobials, and adequate supportive therapy contribute to the success or failure of a therapy. The owner's delay in seeking therapy, the primary cause of peritonitis, and the patient's age are important factors beyond the clinician's control. When aggressive therapy is economically possible, survival rates are good, but long-term sequelae may compromise a complete recovery.
MISCELLANEOUS PERITONEAL CONDITIONS
Ascites. Ascites is a collection of serous fluid in the peritoneal cavity. It must be considered a secondary sign rather than a primary diagnosis. In that regard the primary cause must be identified in order to treat the patient adequately. Common causes of ascites in ruminants include severe liver disease and congestive right-sided heart failure. Young cattle with mesothelioma have remarkable ascites. Ascites remains an uncommon condition that needs to be differentiated from septic causes of peritonitis and from urine accumulation with ruptured bladder.
Pneumoperitoneum. Pneumoperitoneum is commonly observed postsurgically in the bovine. Presence of air in the abdomen can be recognized by simultaneous percussion and auscultation. A low-pitch resonance can be auscultated in the upper flank on both sides of the abdomen. Presence of pneumoperitoneum normally resolves in the week after surgery. No clinical signs seem associated with the presence of pneumoperitoneum, although some clinicians describe abdominal pain associated with no cause other than the presence of air in the peritoneal cavity. Pneumoperitoneum not associated with surgery is indicative of bacterial peritonitis and the presence of gas-producing bacteria (see Box 32.7).
Retroperitoneal Abscess. Retroperitoneal abscess is a particular condition occurring in cattle after a flank laparotomy. It develops in many affected animals several days after surgery. They are mildly febrile, not performing adequately, and showing clinical signs compatible with peritonitis. The skin wound is often unremarkable, but some pain may be elicited while the flank area is palpated. A substantial mass may be palpated rectally, localized in the upper quadrant of the side of the previous surgical approach. The mass is firm, smooth, unmovable, and close to the previous flank incision and may have adhesions attached to it. Transabdominal or rectal ultrasound examination reveals a large amount of fluid located between the peritoneum and the rectus abdominis or the internal oblique of the abdomen. More superficial abscesses can also occur. A needle aspiration allows visual inspection of a thick, opaque, foul-smelling fluid. Treatment is aimed at establishing drainage and systemic antimicrobial therapy. A large volume of purulent and fibrinous material (up to 40 L) can be removed from the abscess. Rapid decompression may provoke hypovolemic shock, and intravenous fluids should be administered before a large abscess is drained. Prognosis is good, but the recovery phase is extremely long because of the large cavity left after drainage. Early closure of the drain is often observed, necessitating reopening. Some clinicians effectively use Penrose drains as they close a contaminated flank wound, to prevent serum accumulation in the wound, and stave off the development of an abscess.