Urogenital System
As the foal begins to move after birth, it causes stretch and breakage of the umbilical cord, typically around 3 cm beneath the abdomen. This can also occur when the mare rises after foaling.61 Early separation of the cord has no detrimental effect, provided the cord is severed by stretch rather than sharp dissection.
The volume of placental blood available for transfer to the foal under normal circumstances is relatively small, typically well below 200 mL.62 Greater volumes may be lost if the cord is cut, preventing contraction of vascular smooth muscle. Hemorrhage should therefore be controlled with a commercial clamp or umbilical tape. Prolonged attachment of the cord is unlikely to be a significant problem, although blood flow between the placental membranes and the foal is partly gravity dependent, such that blood could flow preferentially from foal to membranes if the foal is above the level of the placenta. Manual breakage of the umbilical cord is recommended if it remains attached for more than 8 minutes. The preferred method for manual cord breakage is to grasp the placental side of the cord while holding the foal side of the cord with your other hand to prevent excessive traction on the abdominal wall. Gently twist and pull from the placental side such that the breakage will occur at the natural site of detachment. Intraabdominal umbilical arteries may continue to pulse for several days after delivery; this may result in a palpable pulse in the umbilical stump, but it is not associated with blood flow.62 The umbilical stump should be treated once or twice daily until it becomes dried and sealed. A 0.5% chlorhexidine solution is preferred; however, it may cause delayed drying of the stump. Iodine solutions can also be used, but the concentration should be limited to 2% to prevent tissue necrosis.Urine is one of the most important indicators of health in foals. As a consequence of a milk diet, normal neonatal foals produce a large volume of urine relative to their body weight, estimated at 148 mL/kg/day, or 7.4 L for a 50-kg foal. This value is approximately 5-fold to 10-fold greater than that of a healthy adult horse on a per-kg body weight basis.63 The first passage of urine after birth occurs around 12 hours of age in normal foals, with colts passing urine earlier than fillies. The first urination in normal foals is concentrated with a specific gravity greater than 1.030, which will gradually decrease with subsequent urinations. The urine will become light in color and be very low in specific gravity, typically 1.001 to 1.008. Any foal observed to pass thick, concentrated urine should be assessed closely. Disruption to the urinary tract occurs relatively commonly and can be difficult to diagnose early in the clinical course. Rupture of the urinary bladder during delivery occurs more commonly in colts than fillies, although postpartum disruption to the tract in sick or hospitalized foals has no gender bias.64,65 Signs often include prolonged straining, passage of small volumes of urine, progressive abdominal distention, lethargy, and weakness. Patency of the urachus is a common complication in sick newborn foals. Surgery is rarely required as most will close spontaneously by 2 weeks of age. Techniques to hasten closure generally involve chemical cautery, such as application of silver nitrate around the external opening. However, some believe that the resultant inflammation could predispose to infection or damage to internal structures and therefore limit their therapy to local disinfectants and systemic antibiotic therapy. Surgery would generally be recommended if the urachal leakage continued beyond 3 weeks of age.
In male foals the inguinal and scrotal region should be palpated for swelling and testicular descent. Inguinal and scrotal hernias occur relatively commonly but rarely result in clinical signs.
Preputial edema may be present. Most congenital hernias are indirect, unilateral, and easily reducible and spontaneously resolve by 3 to 4 months of age. Positioning the foal on its back facilitates manual reduction. A figure-8 support wrap can assist in keeping the hernia reduced. Surgical correction is recommended if spontaneous resolution is delayed, if the hernia increases in size, or if signs of colic develop. Certain breeds appear to be at increased risk for herniation, including Tennessee Walking Horses and Standardbreds. A rent in the parietal vaginal tunic can lead to subcutaneous dissection of intestinal loops; this requires surgical reduction, herniorrhaphy, and unilateral castration.66 Although extremely uncommon in foals, signs of colic can occur if herniated loops of intestine strangulate.At the time of birth most testes lie within the inguinal canal. The extraabdominal gubernaculum, which can be easily mistaken for a testicle, typically limits movement into the scrotum. Monorchidism has been reported in foals, and affected colts are usually mistaken as cryptorchids.67 Congenital abnormalities of the penis are rare. Failure to drop the penis during urination can occur as a consequence to preputial edema, a common complication in colts that are straining to defecate or urinate. The free part of the penis is normally fused to the internal lamina of the prepuce for up to 1 month of age. This can make exteriorization of the penis difficult. “Kinking” of the penis has been described, resulting in stranguria or pollakiuria.68 Correction was achieved through manual straightening of the penis.
Umbilical Hernias
Umbilical hernias occur commonly in foals. The condition is generally considered to be a congenital defect with a likely hereditary basis, although umbilical infection may be an important postnatal predisposing factor. In a study of Dutch Warmblood foals, 19 of 44 had a palpable abdominal wall defect between 2 and 6 cm at the time of birth.69 In all but one of these foals the defect had closed by 4 days of age; however, 28% of the foals developed a defect between 5 and 8 weeks of age.
These were considered to be true umbilical hernias in that a hernial sac with contents was palpable in addition to the abdominal wall defect. The group included both foals with or without a palpable abnormality at birth. In a study of hospitalized foals it was concluded that the defect was more likely to occur in fillies than males and that the condition was more common in Thoroughbreds than Stan- dardbreds.70 Most clinicians recommend delay in treatment, as some defects will close spontaneously. Several techniques have been described for repair and vary from external clamps to surgical herniorrhaphy. Rarely, complications associated with umbilical hernias or their repair occur. These include colic, enterocutaneous fistulae, umbilical abscessation, and intestinal incarceration.71Ultrasound Examination of Umbilical and Related Structures
The examination can be performed with the foal either standing or in lateral recumbency using a mid- to high-frequency linear transducer. The preferred probe is a high-frequency (10 to 14 MHz) linear transducer, although diagnostic scans can be performed with a 5- to 7.5-MHz linear rectal probe. Dorsal recumbency affords the best access, but care should be taken as this positioning has an adverse effect on ventilation. Clipping is helpful but not necessary, and most examinations are adequately performed using alcohol with or without coupling gel. Images are obtained in the transverse (short-axis) plane with the probe orientated perpendicular to the vertebral column and in a long-axis (sagittal) plane with the probe parallel to the spine. The external umbilical stump can be assessed for size and echodensity; there are no published normal dimensions for size of the stump (Fig. 16.5). The umbilical vein runs cranially from the umbilical stump to the liver. It is located 1 to 2 cm deep to the skin and is a thin-walled ovoid structure that is 5 to 10 mm in maximal diameter (Fig. 16.6).72 The paired umbilical arteries originate from the internal iliac arteries and run adjacent to the urinary bladder and urachus before emerging at the umbilical stump.
The arteries atrophy postpartum and become the round ligaments of the bladder. They appear as thick-walled hyperechoic structures, which should measure less than 13 mm in diameter (Fig. 16.7).72 Asymmetry in size is common, and there may be an echogenic core if filled with clot (Fig. 16.8). Pulsation may also be noted in very young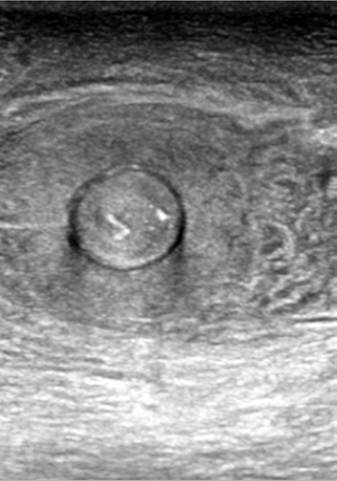
FIG. 16.5 An ultrasound image of an enlarged umbilical stump external to the body wall. The entire stump was 34 ? 43 mm. Note the central core surrounded by thickened tissue.
foals. The urachus connects the apex of the bladder to the umbilical stump. It can be difficult to image unless it is fluid filled, as would occur during patency. At the level of the bladder apex the combined diameter of the urachus and arteries in transverse view should be less than 25 mm. The bladder wall should be examined for defects because a full appearance to the bladder does not preclude a leak (Fig. 16.9).
Neurologic System
Differentiation of primary neurologic disease from systemic illness can be difficult as many critically ill foals are somnolent, recumbent, and unable to suck. Neurologic examination of the neonatal foal has several features that are unique to animals of that age.73 While a domed skull could be consistent with hydrocephalus, it is also a physical feature of immaturity. Furthermore, hydrocephalus and other congenital brain abnormalities may occur with a normal skull shape and size.
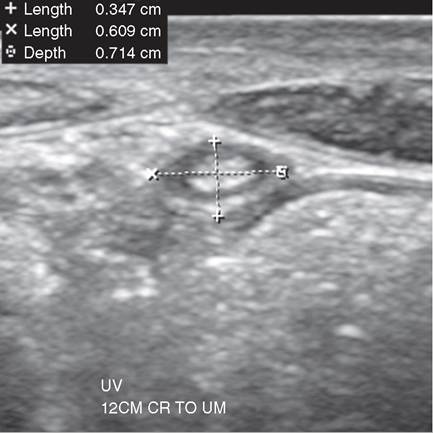
FIG. 16.6 A normal umbilical vein imaged transversely 12 cm cranial to the umbilicus.
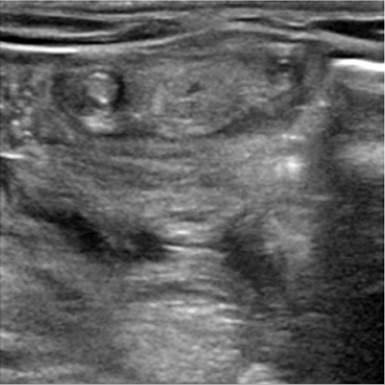
FIG. 16.8 A transverse image demonstrating asymmetry in size and echodensity between the two umbilical arteries. Both were considered normal, and the combined measurement was within normal limits.

FIG.
16.7 A transverse image taken 2 cm caudal to the umbilicus showing the normal paired umbilical arteries and the apex of the bladder. The arteries measured 4.2 and 4.7 mm in diameter.
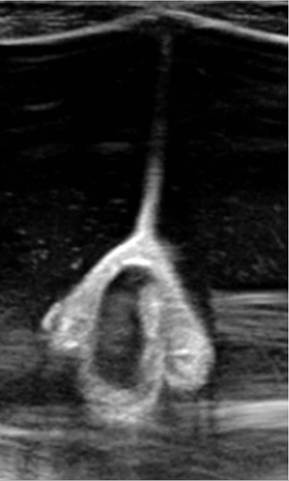
FIG. 16.9 A collapsed bladder attached to the body wall with a large-volume effusion consistent with uroperitoneum. The arteries give the collapsed bladder a classical shape.
Examination of the head should be done with the foal standing or in sternal recumbency. The eyes have a normal slight ventromedial rotation in young foals. As described earlier, pupillary light responses are present but sluggish and the menace response is typically absent in the first week of life, although the foal should withdraw its head in response to a threatening gesture. Further assessment of vision can be through observations of behavior and navigation through obstacles.
The ability to suck and swallow milk should be evaluated. The suckle reflex should be evaluated using a clean and preferably gloved finger. Dysphagia can be recognized by nasal regurgitation of milk or milk coming out of the mouth. Although a cleft in the palate should be an important rule-out, it occurs less commonly than pharyngeal/laryngeal weakness and incoordination due to neonatal encephalopathy or systemic weakness. Dysphagia commonly resolves spontaneously but may take days to weeks.74 Uncommon causes include persistent dorsal displacement of the soft palate, subepiglottic cyst, esophageal disease, or nutritional myodegeneration. Esophageal diseases are rare in the newborn foal. Reported conditions include congenital dilatation or ectasia, tubular or cystic esophageal duplication, megaesophagus, motor dysfunction, and stricture. Most descriptions are in foals outside of the neonatal period. Aspiration of milk into the airway may be difficult to identify due to immaturity of cough receptors; auscultation over the trachea after nursing may identify fluid sounds.
Limb reflexes can be evaluated with the foal loosely restrained in lateral recumbency. Spinal reflexes, such as the patellar, sciatic, and cranial tibial reflexes, are hyperactive in the newborn foal and therefore easily elicited. The neonatal foal can have strong thoracic and pelvic limb crossed extensor reflexes, where a stimulus to the distal limb causes flexion (withdrawal) of the affected limb and extension in the contralateral limb. This reflex is typically only seen in adults with severe or chronic upper motor neuron lesions.75 The painful stimulus should also be recognized centrally.
The gait should be evaluated for evidence of paresis or ataxia. The normal gait is hypermetric and bouncy but should be precise and symmetric and be free of circumduction and

FIG. 16.10 Collection of cerebrospinal fluid at the atlanto-occipital site using a hypodermic needle.
toe-dragging.73 Generalized hypotonia is seen with hypoxic- ischemic syndrome, sepsis, prematurity, botulism, white muscle disease, or heritable muscle disorders. A “bunny hopping” gait could be suggestive of a myelodysplasia, and examination of the anus, tail, and perineum is indicated. Peripheral nerve damage can occur with birthing trauma, particularly brachial plexus or radial nerve injury from forelimb traction. Affected limbs are weak, are hyporeflexic, and may have regions of anesthesia.
Seizures can vary from localized or partial to generalized. As described earlier, normal foals in REM sleep can be active, including galloping actions, neck extension, and vocalization. These can last for several minutes and be confused with seizures. Narcolepsy/cataplexy should be suspected in foals that collapse, remain laterally recumbent for several minutes in a sleep state, and then recover uneventfully. The condition has been reported in American Miniature Horses, Morgans, Shetlands, and Suffolks.73 It is possible to induce collapse and flaccidity by applying pressure to the thorax in normal newborn foals. The response is referred to as squeeze-induced somnolence.76 There is a decrease in respiratory and heart rate and activation of the hypothalamic-pituitary-adrenal axis. The response was originally thought to be a form of narcolepsy or cataplexy, but electroencephalogram data in a small number of foals was not consistent with REM sleep, a feature of true narcolepsy.76 An exaggerated head nod, a base wide stance with truncal sway, and dysmetric gait without weakness may indicate cerebellar dysfunction. The most common cause would be cerebellar abiotrophy, an inherited condition of Arabian horses and Gotland ponies.
Cerebrospinal Fluid Collection
Samples of cerebrospinal fluid (CSF) can be obtained from the atlanto-occipital (AO) or lumbosacral (LS) sites. The procedure is helpful in differentiating neonatal encephalopathy from bacterial meningitis. An AO CSF tap is a relatively straightforward procedure (Fig. 16.10). In comatose or profoundly somnolent foals, an AO tap can be performed using diazepam (0.05 to 0.2 mg/kg IV), local anesthesia, and adequate restraint. In more active foals general anesthesia should be used. In most neonatal foals the tap can be performed using a 3.8-cm, 18- to 20-ga hypodermic needle; in larger foals (>55 kg) a styletted spinal needle will be required. The needle is inserted at the intersection of a line drawn from the anterior wings of the atlas and midline. The poll is flexed tightly, and the needle is directed to the mandible. Alternatively, CSF can be collected from the lumbosacral (LS) site in the standing foal or in foals that are laterally recumbent without the need for general

FIG. 16.11 Bilateral carpal and fetlock contracture in a newborn foal.

anesthesia. The landmarks for LS are the cranial borders of the tuber sacrale. A 3.5-inch styletted needle is inserted on midline approximately 5 mm cranial to a line intersecting the borders of the tuber sacrale after local anesthesia and a stab incision with a No. 15 blade. The sample should be analyzed within 30 minutes because of rapid cell degeneration. Normal CSF has 1 to 5 cells^L with cells restricted to monocytes and lymphocytes. There should not be any neutrophils in normal foal CSF. Yellow discoloration (xanthochromia) and slight turbidity of the sample can be normal. Similarly, CSF protein concentration can be elevated in foals during the first 2 days of life.77
Musculoskeletal System
The hoof wall of the newborn foal is covered by soft horn, or perionychium, a protective layer that is rapidly worn away when the foal begins to ambulate.78 The coronary bands should be examined for hyperemia, an early indicator of systemic sepsis. Changes in hoof capsule temperature could also indicate regional or generalized perfusion problems. The limbs should be assessed for flexural laxity or contracture (Fig. 16.11). Mild to moderate limb contraction can make it difficult for the foal to stand and ambulate. In response to pain, foals with contracted tendons may have elevated heart and respiratory rates, as well as diffuse muscular tremor. In severe cases the foal may not be capable of standing. Treatment involves a combination of analgesia, splinting, and intravenous oxytetracycline. Repeated dosing of oxytetracycline is discouraged due to the risk of renal complications.79 Extensor tendon rupture is a complication of flexural contraction and is recognized by discrete soft fluctuant swelling on the lateral aspect of the carpus.80 The condition is often mistaken as septic synovitis. Foals usually respond well to conservative management. Fetlock laxity is common and can often be managed using heel extensions taped to the foot.
As part of the physical examination, all peripheral joints and physes should be palpated for swelling, heat, pain, and edema. Although trauma is often implicated as the source of any lameness, infection should always be considered as the most likely cause until proven otherwise. Other problems that may be identified in the neonate include rupture of the gastrocnemius muscle (Fig. 16.12) or associated muscle and patellar luxation. Foals are unable to bear weight when there is complete rupture of gastrocnemius muscle and cannot stand when bilateral rupture occurs.81
Premature or dysmature foals have joint laxity and delayed ossification. Joint laxity can predispose affected foals to angular limb deformities. These are managed through a combination

FIG. 16.12 Rupture of the gastrocnemius muscle has a guarded to poor prognosis in foals.
of hoof trimming, exercise restriction, and splinting. Delayed ossification is assessed using radiography, centering on the cuboidal bones of the tarsus and carpus. The management of delayed ossification is difficult, and collapse or crush of cuboidal bones can sometimes be unavoidable. Preventative strategies include restricted exercise and splinting.
Supplementation of foals with selenium is recommended for those born in known selenium-deficient regions where mares have not been supplemented during pregnancy. Severe rhabdomyolysis has been reported in newborn foals, usually associated with selenium deficiency.82 Glycogen branching enzymes deficiency is an inherited cause of mortality in Quarter Horse foals.83 Clinical signs are variable and include seizure, persistent recumbency, respiratory failure, and cardiovascular collapse. The generalized nature of the clinical signs would likely lead to a false diagnosis of other more common neonatal diseases.
Dermis
A short, silky hair coat is consistent with immaturity. Skin abrasions occur in foals with prolonged recumbency or as a consequence to seizures, colic, or frequent unsuccessful attempts to rise. Lesions are commonly seen on the elbows, around the eyes, or on other skeletal prominences. They usually begin as focal regions of moisture. A syndrome of ulcerative dermatitis with widespread crusting and erythema has been seen in foals with alloimmune thrombocytopenia.84 Edema can form on the ventrum, axilla, perineum, and periorbital region with fluid overload and renal dysfunction. Swelling under the axilla can also result from cellulitis, trauma, or fractured ribs. Ventral swelling over or around the umbilicus can occur with tearing of the urachus and urine leakage into tissues (Fig. 16.13).
Immunoglobulin G and Colostrum
There is an association between low serum immunoglobulin G (IgG) and morbidity and mortality, most commonly due to sepsis. Measurement of serum IgG should be made between 12 and 18 hours of age. A normal foal that has consumed adequate amounts of colostrum will have a serum IgG measurement substantially greater than 8 g/L (800 mg/dL). Failure of passive transfer is generally defined as a serum IgG less than 4 g/L (400 mg/dL); partial failure of passive transfer is used when the serum IgG is between 4 and 8 g/L. Foals that have been exposed to chronic in utero infection can be born with IgG concentrations greater than 8 g/L. Furthermore, septic foals may catabolize immunoglobulins, resulting in lower concentrations than originally assessed. Tetanus prophylaxis, in the form of antitoxin (1500 IU), should be administered to foals with untreated failure of passive transfer.
Good-quality colostrum is typically yellow and highly viscous, but physical properties alone do not result in significant differences in foal IgG levels at 24 hours of age.85 There is a strong linear correlation between colostral specific gravity and IgG concentration.86,87 A modified hydrometer, the Equine Colostrometer (Jorgensen Laboratories, Colo.) is used to estimate the specific gravity of equine colostrum. It is important to accurately add the recommended volume of colostrum to the chamber. The temperature of the distilled water will also influence the final reading, and corrective tables are available. Handheld refractometers that measure sugar or

FIG. 16.13 Swelling around the umbilicus caused by tearing of the urachus within the tissues of the body wall.
alcohol content are also suitable for assessing colostral quality. The test can be performed rapidly by placing a single drop of mixed colostrum onto the glass prism of the refractometer. Values greater than or equal to 16 on the alcohol scale, or 23% on the BRIX sugar scale, correspond to a colostral IgG content greater than or equal to 60 gm/L.85,88 The following guidelines have been recommended for evaluating BRIX readings:
(1) 0% to 15% BRIX, 0 to 28 gm/L IgG, poor quality;
(2) 15% to 20% BRIX, 28 to 50 gm/L IgG, borderline quality;
(3) 20% to 30% BRIX, 50 to 80 gm/L IgG, adequate quality; and (4) greater than 30% BRIX, greater than 80 gm/L IgG, very good quality.88
A minimum dose of 60 to 90 gm/L of IgG has been recommended in the first 6 hours after birth.89 This represents 1 to 1.5 L of good-quality colostrum, as defined by an IgG content of greater than 60 gm/L. Foals that received a minimum of 1.0 to 1.25 gm/L IgG/kg body weight within this time period should achieve a serum IgG above 8 gm/L.90 The total IgG content in mammary secretions is highly variable but was reported to be 183 ± 58 gm/L (range 112 to 336 gm/L), equating to a mean volume of colostrum of 2.3 ± 0.5 L.90 The specific gravity declines to below 1.040 by an average of 7 hours after parturition, reflecting a reduction in IgG concentration from a mean of 113 gm/L to 35 gm/L. Several factors influence colostral quality. Mares that are stressed or ill are less likely to produce good-quality colostrum, as are animals with adrenal hyperplasia secondary to pituitary dysfunction or those receiving exogenous glucocorticoids. Aged mares, particularly those older than 15 years of age, tend to produce colostrum with a lower IgG concentration.89
Laboratory Data
Hematology and biochemistry can provide a critical insight in identifying foals at risk of developing clinical disease, in assessing the magnitude of clinical problems, and in monitoring response to treatment. Normal hematology, biochemical, and electrolyte data are reported in Tables 16.3 and 16.4. Foals that have been exposed to an abnormal in utero environment will frequently have abnormalities on routine blood work that can predict future clinical problems. Several important variations
■ TABLE 16.3
Normal Hematology Reference Values for Neonatal Foals
Gestational Age (Premature Foals) Postnatal Age (Term Foals)
| Parameter | 300-309 Days Mean | 310-319 Days Mean | 320-334 Days Mean | 1 Day Mean ± SD | 2-7 Days Mean ± SD |
| RBC (?10⅜L) | 9.6 | 10.1 | 11.3 | 10.5 ± 1 | 9.26 ± 0.8 |
| Hb (g/dL) | 13.1 | 14.1 | 13.2 | 14.4 ± 1.1 | 13.2 ± 1.2 |
| PCV (%) | 41 | 42 | 43 | 42.0 ± 3.6 | 36.5 ± 3.1 |
| MCV (fl) | 42.7 | 42.2 | 38.6 | 40.2 ± 3.6 | 39.4 ± 2.3 |
| MCH (pg) | 14 | 14.4 | 11.8 | 13.6 ± 1.1 | 14.5 ± 1.1 |
| MCHC (%) | 32.4 | 33.8 | 30.5 | 33.8 ± 2 | 36.2 ± 1.1 |
| Icterus index (u) | 40.0 ± 15 | 30.3 ± 15 | |||
| Total plasma protein (g/dL) | 6.1 ± 0.8 | 6.4 ± 0.6 | |||
| Fibrinogen (mg/dL) | 243 ± 74 | 310 ± 90 | |||
| Total WBC/pL | 5000 | 6800 | 4900 | 8632 ± 2570 | 9075 ± 2200 |
| Neutrophils/μL | 1230 | 1540 | 1940 | 6381 ± 2225 | 6528 ± 2000 |
| BandsZμL | 2960 | 50 | |||
| LymphocytesZμL | 3720 | 5090 | 2021 ± 2225 | 2203 ± 575 | |
| MonocytesZμL | 222 ± 160 | 305 ± 145 | |||
| EosinophilsZμL | 0 | 22 | |||
| BasophilsZμL | 8 | 17 | |||
| Neutrophil-to-lymph ratio | 0.33 | 0.3 | 0.66 | 3.16 | 2.96 |
Hb, Hemoglobin; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; PCV, packed cell volume; RBC, red blood cell; SD, standard deviation; WBC, white blood cell.
■ TABLE 16.4
Normal Serum Biochemical Reference Values for Normal-Term Postnursing Foals
| Parameter | Age | |
| 1 Day Mean ± SD | 4-7 Days Mean ± SD | |
| Sodium (mEq/L) | 139.7 ± 6 | 139.5 ± 4.2 |
| Potassium (mEq/L) | 4.4 ± 0.9 | 4.5 ± 0.4 |
| Chloride (mEq/L) | 103.5 ± 3 | 101.3 ± 4 |
| Bicarbonate (mEq/L) | 22.9 ± 3.4 | 34.3 ± 2.1 |
| Calcium (mg/dL) | 11.7 ± 1.1 | 11.4 ± 0.8 |
| Inorganic phosphorus | 5 ± 0.85 | 6.4 ± 0.8 |
| (mg/dL) | ||
| Magnesium (mg/dL) | 2.2 ± 0.35 | 2.7 ± 0.15 |
| Glucose (mg/dL) | 136 ± 40 | 150 ± 30 |
| BUN (mg/dL) | 18.9 ± 4.3 | 13.6 ± 536 |
| Creatinine (mg/dL) | 2.3 ± 0.6 | 1.3 ± 0.3 |
| Total bilirubin (mg/dL) | 4.3 ± 2.2 | 4.4 ± 1.1 |
| Direct bilirubin (mg/dL) | 0.5 ± 0.2 | 0.8 ± 0.4 |
| Indirect bilirubin (mf/dL) | 3.8 ± 1.5 | 3.5 ± 1.1 |
| Alkaline phosphatase | 2282 ± 1100 | 1949 ± 1100 |
| (IU/L) | ||
| GGT (IU/L) | 29.6 ± 15 | 18.3 ± 7.3 |
| SDH (IU/L) | 2 ± 0.9 | 2 ± 0.9 |
| AST (SGOT) (IU/L) | 154 ± 55 | 225 ± 60 |
| LDH (IU/L) | 487 ± 100 | 490 ±100 |
AST, Aspartate aminotransferase (SGOT); BUN, blood urea nitrogen; GGT, γ-glutamyltransferase; LDH, lactate dehydrogenase; SD, standard deviation; SDH, sorbitol dehydrogenase.
to adult values must be considered when interpreting laboratory data. In addition, there are some differences between horse foals and donkey foals and readers are directed to an appropriate reference.91
White Blood Cell Count and Differential
The total white blood cell (WBC) count at birth is similar to that in adult horses, but the proportion of neutrophils and lymphocytes is more variable. An elevated count at birth reflects a fetal response to placental infection with or without infection of the foal. Premature or dysmature foals with incomplete adrenal maturation will have low total white cell and neutrophil counts and a neutrophil-to-lymphocyte ratio that is characteristically less than 1:1.92 It is important to determine if sepsis is present as neutropenia is also a common feature of this condition. Evidence of shifting toward immature cell types, and neutrophil toxicity should indicate primary sepsis or prematurity/ dysmaturity complicated by sepsis. Premature foals that fail to improve their total white blood cell and neutrophil counts over the initial 24 to 48 hours of treatment have an even poorer prognosis for survival. Persistent decreases in lymphocyte counts (Enzymes, and Bile Acids
Relative to adult horses, newborn foals have increased total bilirubin concentrations that are attributable to the unconjugated component. The basis of the discrepancy is not known but could relate to accelerated breakdown of fetal and neonatal red blood cells or decreased uptake and conjugation of bilirubin. Concentrations peak shortly after birth before declining to adult levels by 2 weeks of age.106 Increases in bilirubin above normal are seen with hemolytic conditions, such as neonatal isoerythrolysis, primary liver disease (including equine herpesvirus-1 infection, Tyzzer's disease, and cholangiohepatitis), sepsis, meconium impaction, and after internal hemorrhage or blood transfusion. Large increases in bilirubin can lead to the neurologic complication of kernicterus.
Gamma glutamyl transferase is normal at birth but increases between 5 and 14 days of age before decreasing to adult levels by 4 weeks of age. The increase is thought to be due to hepatic enzyme induction associated with normal maturation. The hepatocellular enzyme, sorbitol dehydrogenase, is not affected by age. Glutamate dehydrogenase concentration has not been well described in healthy newborn foals. These enzymes are increased in a range of conditions, particularly sepsis.107
The concentration of aspartate aminotransferase increases slightly after 7 days of age; an increase attributed to enhanced muscle activity rather than hepatobiliary changes. Serum alkaline phosphatase (ALP) concentrations are substantially increased over adult levels in the first few days of life, remaining elevated through the first week. The initial increases are attributed to intestinal activity, including the pinocytosis of maternal immunoglobulin, and to the osteoblastic activity in growing and adapting bones. Premature or dysmature foals with incomplete ossification will have ALP concentrations that are higher and persist for longer than levels in term foals.40
Serum bile acid concentrations are also greater in foals during the first 6 weeks and are 6 to 7 times greater than adults during the first 2 days of life.108 Increased concentrations of bilirubin or triglycerides or hemolysis may interfere with serum bile acid measurement under certain methodologies. Serum cholesterol is also elevated during the first 2 weeks of life.
Trigylcerides
Triglycerides increase from birth to the first day of life, peaking early in the first week, and then gradually declining to adult levels by 3 months of age.106,109 Increases in lipids, reflected through serum hypertriglyceridemia, are commonly reported in sepsis in foals, presumably secondary to altered fat metabolism.110,111 Serum triglyceride concentrations are higher in foals with positive blood cultures and higher in nonsurviving foals (survivors: 116mg∕dL median [41 to 379, range] versus nonsurvivors: 55 mg∕dL, median [10 to 311, range]).109
Electrolytes
As with adult horses, serum electrolyte concentrations in foals are maintained within a relatively narrow range. Disruption of the urinary tract or primary renal disease classically produces a hyponatremia, hypochloremia, hypocalcemia, hyperphosphatemia, and hyperkalemia. Many of these changes reflect the electrolyte intake associated with a milk diet and are less likely to occur when foals have received intravenous fluid therapy. Rhabdomyolysis due to selenium deficiency can cause a similar electrolyte profile to that of uroperitoneum in milk-fed foals.82 Although both conditions may be associated with increases in creatinine and BUN, concurrent and substantial increases in creatine kinase and aspartate aminotransferase are expected with rhabdomyolysis.
Hyponatremia, hypochloremia, and hypokalemia are commonly seen with diarrheal disease in foals. Severe hyponatremia is more commonly seen in older foals with diarrhea that are allowed to replenish fluid losses by consumption of plain water. Hyponatremia is also a feature of renal disease, but hypernatremia can occur when affected foals are treated with relatively high volumes of sodium-rich intravenous fluids in the face of inadequate urine output.
Elevated total and ionized calcium concentration can be present in foals born to mares with marked placentitis.40 Clinical hypocalcemia results in signs of tachycardia, sweating, tremor, muscular rigidity, and a stiff gait or recumbency. The syndrome is rare, but euthanasia is common due to failure to respond to calcium supplementation.112 Parathyroid hormone concentrations may be elevated, decreased, or normal, suggesting differing syndromes.