Urolithiasis
Stacey R. Byers
Definition and Etiology
Urolithiasis is a common metabolic disease in all livestock species, but castrated small ruminants are particularly at risk. Uroliths cause disease through trauma to the urinary tract and obstruction of urinary outflow.
Urolithiasis can occur in outbreaks, as an endemic problem in group-housed animals, or as an individual disorder.The clinical signs of urolithiasis vary and are based on duration, extent (complete vs. partial), and location of the obstruction. Early clinical signs can be remarkably subtle and may include anorexia, depression, and mild bloat. A history of colic and straining to urinate or defecate may be provided, and novice owners often mistake stranguria for constipation or tenesmus. If investigating a sick, intact, or castrated male small ruminant, urolithiasis should be high on the differential list, regardless of the clinical signs.
Four common disorders can result from urolithiasis: acute urethral obstruction, chronic urethral obstruction, urethral rupture, and urinary bladder rupture. Less commonly seen are ureterolithiasis and hydronephritis.
Clinical Signs and Differential Diagnoses
Acute Urethral Obstruction
Impacted calculi lead to urethral trauma and progressive bladder distention, resulting in stranguria and abdominal pain. Affected animals may be restless, tread, swish their tails, and grind their teeth. Goats and camelids may vocalize. Tachycardia, tachypnea, and mild bloat secondary to ruminal stasis are common findings. Stranguria is manifested as repetitive bouts of stretching and contraction of the abdominal muscles. Straining may induce secondary rectal prolapse, so urethral obstruction should be investigated as the primary disease in cases of rectal prolapse. Rarely, affected calves develop a visible dilation of the urethra at the midline of the perineum proximal to the obstruction.1 Anuria occurs if urethral obstruction is complete, whereas urine may dribble in cases of partial obstruction.
Crystals or blood may be found on the hairs of the preputial tuft; in cases of anuria the hairs are dry. If a urine sample can be collected for dipstick analysis, proteinuria and occult hematuria are frequently detected.Rectal palpation (digital rectal palpation in small ruminants and camelids) often reveals pulsation of the pelvic urethra. In cattle, bladder distention is palpable per rectum, although if bladder or urethral rupture has occurred, the bladder is typically not palpably enlarged.
Abdominal palpation may be useful in affected small ruminants, small camelids, and pot-bellied pigs. The examiner should place the fingertips of each hand into the ventral flank on each side of the abdomen. While slowly pressing the fingertips toward midline in the caudal abdomen, the examiner may encounter an orange- to grapefruit-sized, firm, spherical structure, which is the distended bladder. Severe bladder distention will not be palpated in cases of incomplete urethral obstruction or bladder rupture.
Common sites for urolith obstruction include the distal aspect of the sigmoid flexure, near the insertion of the retractor penis muscles in cattle, and the urethral process in sheep and goats. However, uroliths can be found along any length of the urethra.
Owing to the frequent lack of specific clinical signs, acute urethral obstruction can resemble a variety of diseases. Tachycardia, colic, bloat, and anorexia are characteristic of GI obstruction, but auscultation and percussion of the abdomen, abdominal succussion, rectal palpation, and transabdominal or transrectal ultrasonographic examination should differentiate this condition from acute urethral obstruction. Encephalopathies, salmonellosis, coccidiosis, and proctitis from rectal prolapse or trauma frequently cause tenesmus. Additional signs of primary neurologic or GI dysfunction should be evident with these diseases.
Although rare in male ruminants, primary UTIs may result in dysuria and pollakiuria. Bladder distention is uncommon with UTI, and large numbers of WBCs and bacteria are present in the urine sediment.
Occasionally, an animal with urolithiasis successfully voids the obstructing urolith(s). The resultant traumatic urethritis might cause dysuria, but the rate and ease of urination typically improve over time and with anti-inflammatory treatment.
Juvenile male camelids have been observed straining or posturing to urinate. On cystotomy, no uroliths have been discovered. Etiology has not been conclusively determined, but transrectal ultrasound has identified prostatitis in some individuals. It is suspected that hormonal influences or ascending UTIs may be contributing to prostatic or urethral inflammation.
In younger animals, it is important to consider congenital abnormalities (e.g., ectopic ureter(s), pelvic displacement of the urinary bladder, urethral duplication). Congenital abnormalities may manifest at birth or not until later, depending on the level of observation and whether the defect results in obstruction, partial obstruction, or constant urine dribbling.
Chronic Urethral Obstruction
Uncommonly, partial urethral obstruction causes chronic dysuria and stranguria if calculi impair but do not completely obstruct urine outflow.2 If a chronic partial obstruction is present, the affected animal has a characteristic slow or intermittent urine flow during voiding. Lethargy, reduced appetite, and thin body condition are evident if renal failure has developed. On rectal palpation, the bladder may be small, and thickening of the bladder wall may be palpable.2
Urine dribbling may also occur in animals with neurologic disease, previous urethral trauma (stricture formation), congenital anomalies of the urogenital tract, infection, or neoplasia. Contrast urethrography may be used to identify the presence of strictures or anomalous structures. Small ruminants with the internal form of ulcerative posthitis may dribble urine. In such cases, characteristic preputial lesions are present. Tumors of the urinary tract, although rare compared with urolithiasis, may cause gradual obstruction in cattle, small ruminants, and camelids.
If there is a complete urethral obstruction for approximately 36 hours or more, the animal is at risk of developing bilateral hydroureter and hydronephrosis, and imaging studies of the kidneys and ureters are warranted.
Urethral Rupture
Urethral rupture is a common complication of urethral obstruction in ruminants and camelids. The wall of the obstructed urethra undergoes pressure necrosis, causing leakage of urine into the subcutaneous tissue of the perineum and ventral abdomen. Sequelae include cellulitis, penile adhesions (possibly creating phimosis), urethral fistula formation, and urethral stricture. Erection failure secondary to vascular obstruction of the corpus cavernosum of the penis has been reported as a sequela to urethral obstruction and rupture in a goat.3
Affected animals are frequently depressed and inappetent and have bilaterally symmetric, pitting edema in the ventral perineum, inguinal region, prepuce, and ventral abdomen (Fig. 34.18). Swelling of the abdominal wall may extend as far forward as the axillae. The affected areas are initially warm and painful on palpation. As necrosis progresses, the tissues become cool, dark, nonpainful, and potentially gangrenous. A fistula may develop to allow urine to escape. Fever may occur if tissue necrosis and sloughing are extensive. Transrectal palpation or ultrasound reveals a small bladder.
Ventral abdominal swelling is also found with umbilical or scrotal hernias and omphalophlebitis. These conditions can be differentiated from urethral rupture by careful palpation of affected tissues, aspiration of any fluid pockets for cytologic examination, and ultrasonography. In bulls, penile hematomas may cause localized swelling of the prepuce in the prescrotal
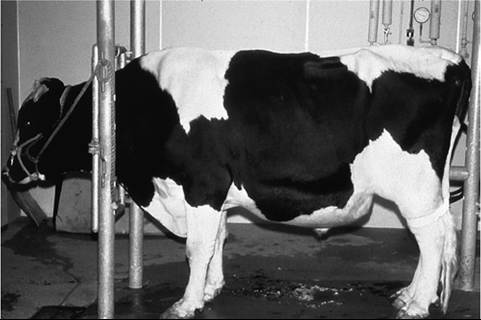
FIG. 34.18 Urethral rupture in a Holstein steer. Tissue swelling from urine accumulation may extend to the sternum and axillae.
region and caudal sheath, but the swelling does not involve the ventral abdominal wall.
Aspiration of a suspected penile hematoma is not recommended because of the risk of iatrogenic infection.Urinary Bladder Rupture
In all ruminants and camelids, prolonged bladder distention secondary to urethral obstruction may result in pinpoint perforations, tears, or necrosis of large areas of the bladder wall. In cows, bladder rupture may also occur as a rare complication of dystocia.4 Rupture of an urachal remnant may also result in uroperitoneum.5 The dorsum of the bladder fundus is the most common site for rupture, but bladder rupture can occur at any site.
Relief of bladder distention causes cessation of stranguria. Bilateral distention of the ventral abdomen develops within 1 to 2 days after rupture and is accompanied by worsening clinical signs of depression, anorexia, weakness, dehydration, and shock. Ballottement of the abdomen may elicit a fluid wave. Rectal temperature may be normal, but shock may result in hypothermia. The animal's breath may smell like ammonia. On transrectal or transabdominal palpation, the bladder is small or not palpable. Transabdominal ultrasonography reveals a large volume of free fluid and a collapsed or partially filled bladder. Abdominocentesis yields a large volume of blood-tinged fluid; the fluid may smell like urine when heated, although this is quite subjective. On occasion, urine will translocate into the thoracic cavity or scrotum through the inguinal canals. Uremia and dehydration result in debilitation and eventual death if medical and surgical treatments are not provided.
Seepage of urine across the bladder wall and into the abdominal cavity may occur in cases of severe bladder distention; in such cases, rupture is often imminent.
Differential diagnoses for bladder rupture include diffuse peritonitis, ileus, enteritis, vagal indigestion, ascites, caudal vena caval thrombosis, and hypoproteinemia. Marked peritoneal cavity effusion may be found in cases of mesothelioma or lymphoma.
These conditions are differentiated from bladder rupture through transrectal palpation, ultrasonography, cytologic and chemical analysis of peritoneal fluid, evaluation of serum chemistry, and abdominal exploratory surgery.Ureterolithiasis and Nephrolithiasis
Animals with acute ureteral obstruction may show severe colic with stretching, kyphosis, treading, collapse, and vocalization. Signs of distress may be less severe or even absent if obstruction is intermittent or incomplete.6 Enlargement of the blocked ureter may be palpated transrectally, and if the left ureter is obstructed, enlargement of the left kidney may be appreciated. Transabdominal or transrectal ultrasound may aid in the diagnosis in small ruminants and camelids. Pyelonephritis can be the inciting cause of ureteral obstruction or renal calculosis. With ureteral or renal rupture, uroperitoneum or retroperitoneal accumulation of urine may occur.
Similar signs of abdominal pain or colic can result from GI or urinary tract obstruction in ruminants and camelids. Auscultation and percussion of the abdomen, rectal palpation findings, ultrasonography, or radiography may allow for differentiation of GI obstruction from ureteral or renal obstruction. Cases of ureteral or renal calculosis without colic may show nonspecific signs of illness, and serum chemistry, urinalysis, and ultrasound examination are needed for definitive diagnosis.
Ancillary Diagnostic Tests
Examination of the Urethral Process in Small Ruminants
Sedation or general anesthesia facilitates extrusion of the penis for examination. Because of its diuretic effect, xylazine may exacerbate bladder distention and is not recommended. Diazepam (0.1 to 0.2 mg/kg IV) and acepromazine (0.05 to 0.1 mg/kg IV or IM) have been used successfully, either as sole agents or in combination with butorphanol (0.05 to 0.1 mg/kg IV). Alternatively, isoflurane by mask can be used.
An adjunct or alternative to sedation is administration of epidural anesthesia, which provides greater patient comfort and eliminates muscular resistance to penile extrusion. One milliliter of 2% lidocaine per 15 kg (33 lb) of body weight is injected into the epidural space at the lumbosacral junction. Lower dosages may provide sufficient anesthesia. The total dose should not exceed 15 mL of 2% lidocaine in any small ruminant, regardless of size. If CSF is obtained, half of the epidural lidocaine dosage can be administered as a true spinal block. Hindlimb motor blockade is expected with either epidural or true spinal anesthesia at this site; the effects typically last 1 to 2 hours.
To exteriorize the penis, the sheep or goat is propped up on its rump and the hind legs are pulled up alongside the trunk. For larger sheep or goats, this can be aided by a person sitting (e.g., in a chair or on a bale of straw), with the animal propped up between his or her legs. It is critical that the animal be positioned such that its spine is perpendicular to the floor. Addition of lidocaine jelly or several milliliters of 2% lidocaine added to a water-based lubricant and squirted into the prepuce may decrease discomfort for exteriorizing the penis. The examiner can then exteriorize the penis by pushing the sigmoid flexure cranially from the base of the scrotum while pulling the sheath caudally. In some animals and overconditioned males, the preputial mucosa must be carefully grasped with small forceps or Allis tissue forceps to aid in extruding. The penis can then be grasped with a piece of gauze to keep it exteriorized. The urethral process can then be inspected and palpated for the presence of discrete uroliths or sandlike grit within the lumen. If the urethral process is obstructed, it can be amputated with a scalpel blade (see Surgical Treatment section later).
ULTRASONOGRAPHY AND RADIOGRAPHY. A presumptive diagnosis of urolithiasis can usually be made through historical and physical examination findings. Ultrasonographic and radiographic evaluation of the urinary tract is useful for confirming the diagnosis, locating obstruction sites, and aiding in determining prognosis.7-11 In cases of prolonged urethral obstruction (≥48 hours) or urethral obstruction with severe azotemia, it is prudent to perform ultrasonographic examination of the kidneys before considering surgical treatment. Detection of severe hydronephrosis warrants a poor prognosis for recovery.
Ultrasonographic evaluation of the bladder of pot-bellied pigs, small ruminants, and camelids is most easily accomplished through transabdominal scanning directed caudodorsally from the inguinal area. Both kidneys of small ruminants and camelids and the bovine right kidney can be examined from the right paralumbar fossa. In cattle, transrectal examination of the pelvic urethra, bladder, ureters, and left kidney can be performed. Marked distention of the bladder, thickening of the bladder wall, and echogenic material within the bladder lumen may be seen with acute urethral obstruction. A large volume of free fluid in the abdomen is characteristic of uroperitoneum and is suggestive of existing or impending rupture.
Radiographic examination of the urinary tract is limited to pot-bellied pigs, camelids, small ruminants, and young cattle. Lateral views of the abdomen can be used to detect and locate radiopaque calculi in the bladder and urethra.9 This is accomplished most easily with the animal in lateral recumbency with the hindlimbs pulled caudally. It is also essential to image the entire urethra to determine the presence and location of additional stones.
Intravenous, normograde or retrograde contrast urethrography can assist in the detection of radiolucent urethral calculi, urethral strictures, or urethral rupture. A contrast urethrogram can be performed in adult bucks and rams and some older castrated males by placing a catheter approximately 5 cm into the penile urethra and injecting 10 to 30 mL of water-soluble contrast media. The catheter should be completely filled with contrast material before insertion into the urethra to avoid accidental introduction of bubbles into the catheter. Injection should be performed slowly with minimal pressure to avoid iatrogenic urethral rupture. The technique may not be possible in juveniles and wethers as the penile frenulum limits exteriorization of the penis. Following tube cystostomy, contrast urethrography can be performed by injecting the contrast material into the bladder through the catheter. The catheter can then be clamped shut temporarily to detect stones, strictures, or urethral rupture.
Clinical Pathology
ACUTE AND CHRONIC URETHRAL OBSTRUCTION. Hematologic and serum chemistry findings may be unremarkable in ruminants with acute urethral obstruction uncomplicated by urethral or bladder rupture. Hyperglycemia and a stress leukogram may be present. With time, hemoconcentration and azotemia develop secondary to reduced water intake. Hematuria and proteinuria are consistent abnormalities, whereas crystalluria is a variable finding. With chronic urethral obstruction, hyponatremia, hypochloremia, hypocalcemia, hyperphosphatemia, and severe azotemia with isosthenuria suggest extensive nephron damage caused by hydronephrosis. Pyuria is present with traumatic urethritis, cystitis, or secondary bacterial infection.
BLADDER RUPTURE. Bladder rupture and accumulation of urine in the abdomen result in hematologic and serum biochemical parameter alterations that worsen over time. Urine osmolality is normally two to three times that of extracellular fluid (ECF), and urine contains higher concentrations of urea, creatinine, and potassium but lower concentrations of sodium and chloride than ECF. Therefore, movement of water, urea, and electrolytes occurs along diffusion gradients, resulting in hyponatremia, hypochloremia, hyperphosphatemia, uremia, and hemoconcentration.
Serum potassium concentration in ruminants with bladder rupture is more variable, depending on appetite and time before diagnosis. Although animals with uroperitoneum are at risk of hyperkalemia, serum potassium concentration tends to be normal or low in ruminants with bladder rupture, even if uroperitoneum exists for several days. Anorexia may contribute to hypokalemia or normokalemia in these cases, and aldosterone release secondary to volume depletion results in dramatic increases in salivary potassium excretion, providing an alternative route of potassium excretion in affected animals. Once in the GI tract, potassium absorption may be diminished by ileus and preferential absorption of sodium over potassium. Alkalosis, which occurs secondary to hypochloremia, may also serve to reduce ECF potassium concentration by encouraging movement of potassium intracellularly.
Although only a small fraction (and Nephrolithiasis
Azotemia and secondary hydronephrosis are most severe if the obstruction is bilateral. With chronic ureteral obstruction, hyponatremia, hypochloremia, hypocalcemia, hyperphosphatemia, and severe azotemia with isosthenuria suggest extensive nephron damage caused by hydronephrosis. Pyuria is present with traumatic urethritis, cystitis, or secondary bacterial infection.
Pathophysiology
Multiple factors influence the development of urinary calculi, but of primary importance is the development of high urinary concentrations of soluble ionized minerals (crystalloids) that aggregate to form insoluble crystals. Supersaturation of urine with a calculus-forming crystalloid is a prerequisite for urolith development, but supersaturation alone is not solely responsible for urolith initiation because normal urine is typically supersaturated with a variety of calculogenic ions.12 Urine contains variable concentrations of mucopolysaccharides, ions, and organic acids that act as intrinsic inhibitors of crystallization. Through physical and electrochemical interactions, these compounds maintain calculogenic minerals in a colloidal suspension. Calculus formation is initiated if supersaturation of urine with appropriate crystalloids exceeds the protective capabilities of the crystallization inhibitors. The crystalloids are rendered insoluble and precipitate out of the aqueous phase of urine. Calculi enlarge as further mineral precipitation takes place on the crystal surfaces. Dietary, environmental, and management influences interact to determine the degree of supersaturation of urine with calculogenic minerals. Dehydration, with resultant concentration of urinary minerals, would appear to be a potential contributing factor in the development of all types of uroliths.
The solubility of some calculogenic crystalloids is influenced by urinary pH. Struvite (magnesium ammonium phosphate), calcium phosphate, and calcium carbonate uroliths are less soluble in alkaline urine, whereas calcium oxalate solubility is not affected by changes in urine pH within the physiologic range. The effect of urinary pH on silica calculi is debatable, but there is a trend toward reduction in formation under conditions of mild aciduria.13
Primary UTIs are considered an uncommon cause of ruminant urolithiasis. Purulent debris within the urinary tract may serve as a nidus for crystal development, and bacterial ureases may increase urinary pH, thereby reducing the solubility of certain crystalloids. Vitamin A deficiency has been incriminated as a contributory factor for urolith development by leading to metaplasia of urinary tract epithelium.12 This may create nidi for calculogenesis through desquamation of cells or altered cell surface characteristics.
Feeding patterns may influence the risk for calculogenesis. Meal feeding exerts an osmotic draw of fluid into the rumen from the ECF. This leads to a release of antidiuretic hormone that results in a transient decline in urine output and an increase in urine concentration. These changes in urine composition can be limited through ad libitum feeding.14
The influence of water hardness (dissolved mineral content), in particular in magnesium concentrations, has been implicated in the pathogenesis of this disease in ruminants.15
PHOSPHATIC CALCULI. Ruminants consuming rations high in phosphorus (grain-based rations) typically develop struvite (magnesium ammonium phosphate hexahydrate) or apatite (calcium phosphate) calculi.12,16 Rations where the calcium/ phosphorus ratio is less than 2 : 1 are particularly prone to cause outbreaks of urolithiasis.12 However, the role of phosphorus in urolith formation is not clearly defined, and struvite urolith formation appears to be primarily affected by the magnesium and, to a lesser extent, other minerals in the diet.12,17,18 Magnesium absorbed from the gut is excreted through the kidneys. High potassium in the diet alters the dietary cation-anion difference (DCAD) and increases the risk of urolith formation (see more about DCAD in Prevention section later).19
Ruminant saliva is rich in phosphorus, and the GI tract is the primary route of phosphorus excretion in ruminants. In theory, ruminants consuming pelleted rations produce less saliva, which would reduce GI phosphate losses and increase urinary phosphate excretion. Struvite uroliths are typically white or gray, usually smooth, radiopaque, and easily broken.12 They can be found as a single stone or sandlike debris, which is more commonly seen in ruminants.
SILICA CALCULI. Silica urolithiasis is primarily a problem of ruminants grazing native rangeland grasses of western North America. A fraction of dietary silica, as unpolymerized silicic acid, is dissolved in the ruminal fluid of the grazing animal, absorbed, and excreted in the urine.12 Water intake is usually intermittent in ruminants on rangeland. During periods of water deprivation, water and sodium resorption by the kidneys results in the formation of highly concentrated urine. Calculi can develop as the silicic acid concentrates and polymerizes to the less soluble form, polysilicic acid.
The incidence of silica urolithiasis can be increased by feeding sheep rations that have a high calcium-to-phosphorus ratio (≥ 2.8 : 1) and induce more alkaline urine.13,20 It is important to note that a high calcium-to-phosphorus ratio in the diet can help to prevent one type of urolith (struvite) but may be a contributory factor for another (silica). This underscores the importance of both ration and urolith mineral analyses in the formulation of preventive measures for this disease.
Silica uroliths in ruminants are hard, smooth, white to brown, radiopaque, and often layered.12 The uroliths are usually composed of about 20% mucoprotein, 75% silicon dioxide, and variable amounts of calcium oxalate and calcium carbonate.12
CALCIUM-BASED CALCULI. The two main types of calciumbased uroliths are calcium carbonate and calcium oxalate. Calcium carbonate uroliths are common in small ruminants grazing lush, rapidly growing clover pastures or being fed alfalfa hay.21 Forages like these are rich in calcium and low in phosphorus and magnesium and have high oxalate content. In the gut, oxalate avidly binds calcium and makes it unavailable for absorption. With gradual introduction of oxalate-rich diets, ruminal bacteria efficiently metabolize oxalate to bicarbonate, so metabolism of oxalate in the rumen may increase the availability of dietary calcium. These factors may combine to increase urinary calcium excretion and alkalinize urine, thereby promoting calcium carbonate calculogenesis.
Oxalates in the diet, as well as low calcium and decreased water intake, may increase the risk of forming calcium oxalate stones. Given its low solubility, calcium oxalate crystals are often present in normal urine and may be incorporated into other uroliths as a trace component.22
Calcium carbonate uroliths have a characteristic round, smooth shape and copper color and are often present as multiple uroliths scattered throughout the lower urinary tract. Calcium oxalate uroliths are typically dense, hard, white to yellow, and either smooth or jagged.12
Epidemiology
GENDER. Obstructive urolithiasis in ruminants and camelids is almost exclusively a disease of males and castrated males. Urinary calculi appear to develop to a similar degree in female ruminants, but most calculi can pass through the relatively short, distensible urethra of the female, making urethral obstruction uncommon. The urethra of the male is long and surrounded by the less distensible corpus spongiosum and tunica albuginea.
Research indicates calculi form to a similar extent in the urinary tracts of intact and castrated male ruminants. The increased predisposition for urethral obstruction in steers and wethers may be due to the loss of testosterone on urethral diameter.23,24 However, because many castrated small ruminants are kept as pets, factors such as diet, environment, and age are likely to differ compared with intact males. Specific gender risks in camelids and pot-bellied pigs are not well described; in commercial pigs, urolithiasis is generally associated with husbandry problems such as improper calcium/phosphorus ratio in the ration and inadequate water availability.25
SEASON. The incidence of urolithiasis increases in hot, arid months in warm climates and in late fall and winter in North America. Seasonal effects are likely due to limited water availability and decreased consumption with colder weather.
AGE. All ages of ruminants are at risk for developing obstructive urolithiasis. The tendency for this disease to be seen in younger ruminants may be the result of dietary influences because younger animals are more often fed concentrates for weight gain and eventual slaughter than are mature males kept for breeding. Because relatively fewer mature males are kept for breeding, the apparently increased prevalence of urolithiasis in younger animals may simply reflect the greater numbers of younger males and castrated males at risk.
OTHER. Inherent differences in an individual animal's mineral metabolism or urinary tract health may also play a role; some animals can ingest a calculogenic diet and remain unaffected, while others develop uroliths rapidly. Animals prone to develop uroliths may have ineffective protective capabilities within the urinary tract, such as a lack of crystallization inhibitors.
Certain breeds of ruminants appear to be predisposed to urolithiasis; for example, African pygmy and Nigerian dwarf goats appear to be prone to developing this disease. Again, because these goats are often kept as pets, it is possible they may be fed or managed in ways that increase their disease risk; further, they may be more likely to be seen by a veterinarian compared with ruminants intended for food or kept out on rangeland.
Necropsy Findings
When the entire length of urethra is opened along the sagittal plane, hemorrhage and necrosis of the urethral mucosa are evident at the site of obstruction. Attention should be paid to examination of the distal urethra in camelids, the urethral process in sheep and goats, and the sigmoid flexure in cattle. Calculi may be relatively large, discrete mineral aggregates or very fine and sandlike. Calculus material should be collected for analysis of mineral composition (Box 34.1). Occasionally, no calculi can be found in the urinary tract, but mucosal trauma and necrosis of the bladder or urethra persist.
■ BOX 34.1
Urolith Analysis Laboratories
Minnesota Urolith Center
University of Minnesota
College of Veterinary Medicine
1352 Boyd Avenue, B325
St. Paul, Mn 55108
Phone: 612-625-4221 www.urolithcenter.org
G.V. Ling Urinary Stone Analysis Laboratory
2108 Tupper Hall
University of California Davis
School of Veterinary Medicine
Davis CA 95616
Phone: 530-752-3228 http://www.vetmed.ucdavis.edu/usal/
Canadian Veterinary Urolith Centre
University of Guelph, Laboratory Services Division
95 Stone Rd. W.
Guelph, ON N1H 8J7
Phone: 519-823-1268 ext. 57454 www.uoguelph.ca/ahl/sites/uoguelph.ca.ahl/files/EnglishCV UCForm2017.pdf
Urethral rupture is characterized by the subcutaneous accumulation of urine in the inguinal area, prepuce, and ventral abdomen and hemorrhage at the site of the urethral defect.
In cases of bladder rupture, the abdominal cavity is filled with a large volume of blood-tinged fluid. Defects in the bladder wall vary in size and location, and necrosis of large areas of bladder wall may be present. In rare cases, the bladder wall is intact but obvious uroabdomen exists, suggesting transmural seepage of urine.
Hydronephrosis, hydroureter, and bladder wall hypertrophy may be present in animals with chronic urethral obstruction.2
Treatment and Prognosis
SALVAGE. Steers and feeder lambs may be sent for immediate slaughter if urethral obstruction is diagnosed before development of azotemia or urinary tract rupture.
MEDICAL TREATMENT. Medical treatment of urolithiasis is aimed at relief of the obstruction and correction of any fluid and electrolyte abnormalities. The antispasmodic effect of certain tranquilizers may facilitate passage of a urethral obstruction. These drugs may also aid in relaxation of the retractor penis muscle, which results in straightening of the sigmoid flexure to facilitate passage of calculi. In small ruminants, medical treatment with IV fluids, NSAIDs, or tranquilizers alone is usually unsuccessful, resulting in surgical intervention or euthanasia.
While stabilizing a patient before surgery or as an adjunct to medical treatment, the bladder can be drained with a percutaneous catheter inserted in the lower flank or ventral abdomen. Long IV catheters or a suprapubic catheter can be inserted, using ultrasonography as a guide, and temporarily left in place. Percutaneous infusion using Walpole solution has been used following cystocentesis in goats.26 Urine was removed, and the solution infused into the bladder one to three times to decrease the urine pH to 4 to 5. This process was thought to promote chemical dissolution of uroliths in the bladder and urethra.
Ruminants and camelids with urinary tract obstruction, particularly those with uroperitoneum, often require preoperative stabilization of hypovolemia and correction of electrolyte abnormalities, especially if surgery is to be performed under general anesthesia or with the animal restrained in recumbency. Fluid therapy should be guided by analysis of serum electrolyte concentrations. An initial bolus of hypertonic (7%) saline followed by physiologic (0.9%) saline solution can be used to correct intravascular volume deficits, hyponatremia, and hypochloremia. Calcium salts can be added to the fluids if indicated.
Empirical supplementation of IV fluids with potassium should be avoided because the potential for hyperkalemia always exists. Hyperkalemia can induce bradycardia and fatal cardiac dysrhythmias, and this effect is augmented by concurrent hyponatremia. Administration of dextrose, sodium bicarbonate, and/or insulin (regular insulin at 0.25 to 0.4 U/kg) reduces serum potassium concentration by promoting movement of potassium from the extracellular to the intracellular space. Blood glucose should be closely monitored when insulin is administered. Uremic animals undergoing IV fluid therapy may develop pulmonary edema, so attention must be paid to respiratory rate, auscultatory findings, and respiratory effort during fluid therapy.
Slow drainage of urine from the abdominal cavity reduces pressure on the diaphragm and slows progression of metabolic derangements caused by uroperitoneum. This can be difficult to achieve as the omentum is prone to occluding the cannula. In long-standing cases of uroabdomen, urine may also be present in the thorax, further warranting close observation of respiratory function during anesthesia. Thoracocentesis to remove thoracic urine is indicated if respiratory function is compromised; otherwise, abdominal drainage usually induces resolution of thoracic urine accumulation.
Although bacterial infection is not considered to be a common primary cause of urolithiasis, secondary UTIs may develop after surgical intervention. Loss of the flushing effect of urination, urinary mucosal damage, impaired host cellular defenses secondary to uremia, and indwelling urinary catheter placement may contribute to the development of ascending UTI. Perioperative antibiotic therapy is therefore prudent, with due consideration of withdrawal times in animals intended for slaughter.
SURGICAL TREATMENT. There are multiple surgical options for urolithiasis, which are dictated by economic considerations, intended use of the animal, available facilities and equipment, types of stones, and status of the patient.27 Removal or bypass of the obstruction and restoration of urine output are the goals of surgical treatment. The prognosis for both short- and long-term survival will vary according to the patient's status and the surgical procedure chosen. Acute renal failure is an occasional sequela to urinary tract obstruction and should be considered in the prognosis. Regardless of the surgical technique used, the client should be forewarned about the future risk of reobstruction.
Urethral catheterization and retrograde flushing may dislodge urethral calculi and restore urine flow, but successful clearance of the urethra is rarely achieved and retrograde flushing under pressure may result in urethral rupture or may simply flush stones back into the urethral diverticulum rather than the bladder. Retrograde passage of a catheter may allow for localization of the urethral obstruction, potentially guiding further surgical treatment. Passage of a catheter into the bladder of ruminants and camelids is exceedingly difficult as the catheter typically becomes lodged in the urethral diverticulum near the ischial arch.
Surgical options range from standing procedures in a field setting to surgery under general anesthesia in a hospital. All of the factors mentioned earlier contribute to the wide range of procedures that have been developed, and surgeon preference, case selection, and owner compliance are critical to the success of a technique.
In sheep and goats, amputation of an obstructed urethral process is a simple procedure that may at least temporarily restore urethral patency. The urethral process can be removed without detrimental effects on breeding soundness. Recurrence of urethral obstruction is extremely common, and urethral patency is often maintained for only hours to days before reobstruction occurs.28 This may provide enough time to allow feeder lambs and kids to survive until slaughter.
Penectomy is an option for animals intended for slaughter and is similar to the perineal urethrostomy for risk of stricture formation. Prepubic urethrostomy, perineal urethrostomy, and modified proximal perineal urethrostomy are surgical options for ruminants not intended to be used for breeding.29,30 In small ruminants, postoperative stricture of the stoma or recurrent obstruction with additional calculi is a long-term risk with urethrostomy procedures. Ischial urethrostomy with placement of a Foley catheter into the bladder has been used as a treatment for urolithiasis in heavy feedlot steers and bulls.31 If urethral damage is not severe, this procedure allows the breeding ability of bulls to be maintained.31
Urethrotomy can be used to remove the obstructing calculi followed by primary closure of urethra; however, there is a risk of urethral stricture, adhesions resulting in phimosis in breeding males, and reobstruction with additional calculi.
A Vesicopreputial anastomosis procedure has recently been described in a small number of goats as an option for management of recurrent obstructions.32
Cystotomy can be used to remove calculi from the bladder and maintain breeding soundness. In small ruminants and camelids, bidirectional (normograde and retrograde) flushing is used to restore urethral patency.28 Even if the urethra is successfully cleared of calculi, traumatic urethritis may cause significant postoperative dysuria in these animals. Therefore, some surgeons prefer to also perform a tube cystostomy to allow for rest and healing of the irritated urethra.
Tube cystostomy (surgical or percutaneous placement) allows urine to exit the bladder through a temporary Foley or other type of suprapubic catheter, which is anchored in the bladder lumen and exits the ventral abdomen.33-35 Urethral patency is restored when calculi are spontaneously expelled from the urethra, dissolved, refluxed into the bladder, or removed via urethrotomy. Spontaneous resolution of urethral obstruction after tube cystostomy may take several weeks or longer, and urethral rupture at the site of obstruction due to pressure necrosis can occur. To judge when removal of the catheter is appropriate, the catheter can be clamped shut and the animal observed for urination through the urethra. Fewer complications of tube cystostomy have been reported with surgically placed tube cystostomies versus percutaneously placed cystic cathe- 3335
ters.33, The primary complication is a dislodged catheter, followed by tears of the bladder, leakage of urine into the abdomen, adhesions of the bladder to intestine or body wall, and obstruction of the catheter.
In cases of urethral rupture where patency of the entire urethra is the preferred outcome, tube cystostomy is often the sole feasible option. Primary repair of the urethral defect is rarely successful because of swelling and maceration of the damaged mucosa and risk of stricture formation. Contrast medium can be introduced into the bladder through the catheter to monitor urethral patency, locate urethral obstruction, or identify urethral rupture. The catheter can also be used to lavage the bladder to facilitate dissolution of calculi using Walpole solution or a commercially available urinary lavage product (Renacidin, Guardian Laboratories, Hauppauge, N.Y.).35
In cases of bladder rupture, the urine should be drained from the abdominal cavity and a surgical procedure should be performed to divert urine to the exterior. If primary repair of the bladder defect is desired, a laparotomy and cystotomy or tube cystostomy can be performed. Primary repair of the bladder defect is not always necessary, however, because spontaneous sealing of the bladder with fibrin or omentum can occur. Daily or continuous abdominal drainage may have to be performed until spontaneous sealing occurs. Tears are more likely to seal spontaneously if they are located on the dorsal aspect of the bladder.
In bladder marsupialization the apex of the bladder is exteriorized using a small paramedian incision, and the seromuscular layer of the bladder is circumferentially secured to the abdominal wall. A cystotomy is performed, and the bladder mucosa is secured to the skin, creating a permanent opening for urine drainage from the bladder to the exterior.36 Advantages of bladder marsupialization include decreased hospitalization time and expense for the owner. However, complications include chronic urine scalding, ascending bacterial infection, stricture formation, reobstruction, and bladder prolapse.
Ureteral calculi may be removed by ureterotomy.3 Nephrectomy may be performed in unilateral cases of obstructive nephrolithiasis.38 If unilateral nephrectomy is under consideration, measurement of BUN, serum creatinine, and USG should be performed, and US and renal biopsy can be used to evaluate the remaining kidney.
POSTOPERATIVE CONSIDERATIONS. Continued assessment of hydration status, urine output, serum creatinine, and serum electrolyte concentrations is indicated after surgery. Postobstruction diuresis may result from tubular damage, accumulation of urea or natriuretic factors, or preoperative fluid therapy. Induction of modest diuresis through fluid therapy after surgery may help to reduce azotemia and accumulation of blood clots and bacteria in the urethra.
Antimicrobial therapy with an antibiotic that achieves high urine concentrations is warranted. Duration of antimicrobial therapy depends on the surgical procedure chosen, residue withholding considerations, legal restrictions on use of certain products, and whether or not UTI exists at surgery. For tube cystostomy, antimicrobial therapy is recommended by some while the tube is in place and for at least 1 week after the tube is removed. A study examining indwelling Foley catheters identified Aerococcus and Enterococcus most frequently, and 42% of cultures were resistant to two or more antibiotics.39 Therefore, it is recommended to submit urine samples for culture and sensitivity testing.
Prevention
A preventive approach to urolithiasis begins with a search for risk factors associated with the diet, management, and environment. Whenever possible, ration analysis and mineral analysis of the urolith(s) should be performed to accurately identify causative dietary factors. Consult Box 34.1 for urolith analysis laboratories. If uroliths are not obtained, ration analysis and a thorough dietary history may provide a strong suggestion of the urolith type. Considering the central role of urinary supersaturation in calculogenesis, the ultimate aim of preventive measures should be reduction of urinary concentration of calculogenic mineral ions. The urine should be diluted to such an extent that the calculogenic ions are less prone to precipitate. Dilution of urine is achieved through increased salt and water intake.
DIETARY MANAGEMENT. Prevention of urinary calculi can be difficult because of the conflicting dietary effects of minerals, pH, individual animal susceptibility, and feed availability. General guidelines for prevention of phosphatic calculi require adjustment of the dietary calcium-to-phosphorus ratio to a level of greater than 2 : 1, which can be performed by reducing the amount of grain or other high-phosphorus dietary components and/or increasing calcium in the diet with forages like alfalfa or other legumes. Use of a 0 mEq/kg DCAD diet using ammonium chloride has been shown to help reduce urinary pH to between 6.0 and 6.5 without significantly decreasing blood pH.18 Increasing the quantity of long-stem forage in the ration may increase salivary flow and fecal phosphate excretion.
Because restriction of dietary silica intake in ruminants grazing native grasses is not feasible, dietary management is limited to salt (sodium chloride or ammonium chloride) supplementation to increase water consumption and thereby produce a diuretic effect to reduce urinary calculogenic compounds. Loose salt or lick salt is unlikely to be ingested in sufficient quantities to affect water intake. Gradually increasing quantities of sodium chloride or ammonium chloride in creep feed can help reduce silica urolith development in calves and lambs.13,19 The feeders should be located near a reliable source of palatable water. In one study, reduction of the dietary calcium-to-phosphorus ratio from 2 : 1 to almost 1 : 1 resulted in a trend toward reduced silica calculi formation.19 Prevention of calcium carbonate uroliths in pet small ruminants can be reduced by feeding or supplementing with grass hay rather than feeding alfalfa alone. Salting the grass hay with increasing concentrations of salt may increase water consumption to help maintain a dilute urine. Use of ammonium chloride can aid in urine acidification and increase water consumption.
Ammonium chloride supplementation fed at a level of 0.5% to 1.5% of ration dry matter was found to reduce urine pH to 6 to 6.5 in a group of goats.18 Urine pH in this range should increase the solubility of struvite and apatite crystals. However, the pH of the urine is also influenced by the relative concentrations of strong cations (sodium and potassium) and strong anions (chloride and sulfate) of the entire ration, so the efficacy of ammonium chloride in reducing urinary pH may vary among different livestock operations, because the concentration of these cations and anions will vary among rations.18,40 Long-term or excessive supplementation with ammonium chloride has been reported to result in chronic metabolic acidosis with a corresponding decrease in bone density and excessively low urine pH.18,40 Ammonium chloride is not palatable, so mixing the salt with a more palatable low-potassium product (e.g., sucrose) is typically necessary. Some animals appear to have a renal physiologic adaptation resulting in gradually increasing urine pH with long-term feeding of ammonium chloride. Owners can monitor for changing urine pH with urine pH strips used on a weekly basis. Pulsed feeding of ammonium chloride can be attempted if the urine pH begins to increase.
WATER MANAGEMENT. Maximizing water intake is an important aspect of urolithiasis prevention, regardless of the urolith type involved. Cleaning water containers should be a regular practice. White water containers allow owners to see contamination of the water with dirt and feed; this may prompt more frequent cleaning. Water palatability may also be improved by providing shade for water containers during the summer and heaters in the fall and winter. Automatic waterers should be checked regularly for proper function. Shallow containers capable of rapid refilling provide higher rates of water turnover, resulting in less stagnation.
In operations involving multiple animals or large pastures, placement of multiple watering sites might allow for more frequent intake. This is especially true for sheep, whose banding instinct usually prevents individuals from traveling alone to distant watering sites.