Ventricular Tachycardia
Definition and Etiology
Ventricular tachycardia (VT) is a cardiac arrhythmia characterized by a rapid rhythm originating in the ventricle. This rhythm originates below the bundle of His in the specialized conduction system, surrounding ventricular myocardium, or both.323 VT may be caused by disorders in impulse formation, impulse conduction, or a combination of the two.323 Ventricular reentry is an important mechanism in the genesis of sustained VT, whereas abnormal automaticity is probably responsible for idioventricular rhythms and parasystole.
Changes in autonomic tone may also be important in the genesis of VT. Early afterdepolarizations are thought to be the mechanism responsible for ventricular tachyarrhythmias associated with sympathetic stimulation. Late coupled ventricular complexes or a very premature ventricular depolarization are usually required to initiate VT. VT can occur when there is myocarditis, myocardial necrosis, fibrosis, fibro-fatty infiltrate or neoplasia, bacterial endocarditis (especially involving the aortic or mitral valve), autonomic nervous system imbalance, hypoxia, ischemia, electrolyte or metabolic disturbances, anesthesia, drug administration, sepsis, endotoxemia, toxic myocardial injury, or aortic root rupture, or it may be associated with other, unknown causes.96,233,248,324,325Clinical Signs and Differential Diagnosis
The clinical signs detected depend on the ventricular rate, type of VT (uniform or multiform), duration of VT, and severity of the underlying cardiac disease.325 Large animals with VT may be asymptomatic at rest if the rhythm is relatively slow and uniform, or they may have severe CHF with rapid uniform or multiform VT.325 Exercise intolerance is common and may be so severe that the animal has frequent syncope.
Other complaints include depression, weakness, colic, respiratory distress, coughing, ventral edema, and pulmonary edema. Acute viral or bacterial respiratory disease with high fever may precede development of VT in horses or may occur concurrently with it. Gastrointestinal disease and primary myocardial disease are more common in horses with VT.324,326 Horses with severe hemorrhage are also at increased risk for VA.327 In cattle, VT occurs most frequently secondary to sepsis and toxemia. Anorexia and decreased milk production are common in affected cows.Animals with sustained VT have a rapid heart rate with a regular (uniform) or irregular (multiform) rhythm.328-331 Heart rates as high as 300 bpm have been detected in horses with VT. Heart sounds vary in intensity, with some loud booming sounds (“bruit de cannon”). Arterial pulse may be variable or uniform, with normal (slower rate) or weak (rapid rate) intensity pulses. Pulse deficits frequently occur, particularly with rapid or multiform VT.Jugular pulses are commonly detected in large animals with VT. The large pulse waves seen in the jugular vein are cannon “a” waves that occur when the right atrium and ventricle contract simultaneously. Cardiac murmurs are not commonly detected. Signs of CHF are usually present when VT is rapid and sustained but are uncommon in animals with slower or paroxysmal VT.328-330 Signs of right-sided CHF (ventral edema, venous distention) usually predominate with sustained uniform VT and increase in severity the longer the duration and more rapid the rate of the arrhythmia. Signs of left-sided CHF (coughing, expectoration of foamy fluid, respiratory distress) usually predominate with multiform VT.
The presence of jugular pulses and bruit de cannon in an animal with a rapid regular rhythm helps distinguish VT from sinus or supraventricular tachycardia. Multiform VT can be difficult to distinguish from AF, because both arrhythmias have an irregular rhythm with heart sounds that vary in intensity.
Jugular pulses may also be detected in large animals with AF but are usually less prominent than in animals with VT. Although large animals with multiform VA usually have more severe clinical signs, an ECG is necessary to distinguish these arrhythmias.Clinical Pathology
Electrolyte, metabolic, or toxic causes of VT may be present in large animals with primary GI disease. Hypomagnesemia and hypokalemia have also been associated with development of VT.331 Serum creatinine and BUN may be elevated in horses and cattle in CHF associated with prerenal azotemia. Serum osmolality, BUN, and creatinine increase and urine osmolality decreases acutely in horses with experimental monensin toxi-
177
cosis. Initial decreases in serum potassium and serum calcium have also been reported in these animals. Marked elevations of cTnI have been seen in horses with VT.195,196,326 cTnI is a more sensitive indicator of myocardial injury; therefore cTnI is currently preferred for detection of myocardial injury in horses, cattle, South American camelids, and small ruminants. Cardiac isoenzymes of CK and LDH are often elevated if there is recent myocardial injury associated with VT. Elevation of the myocardial fraction of CK (CK-MB) in excess of 5% of the total CK is compatible with myocardial injury in horses.177 A neutrophilic leukocytosis, elevated SAA, and hyperfibrinogenemia may be detected in animals with infectious myocarditis or bacterial endocarditis or may be elevated owing to the primary underlying disease. In most large animals with VT, however, hematologic findings are normal.
The diagnosis of VT is made from the ECG. A series of four or more ventricular premature complexes (VPCs) is diagnostic of VT.324,332 The electrocardiographic appearance of the VPC may be widened and bizarre, or the QRS duration and appearance of the QRS and T may be near normal, especially in horses (Fig. 30.32).324,325 Although the duration of QRS complexes that are ventricular in origin is usually within the normal range reported for horses, it is usually longer than the QRS duration of the horse's normal sinus beats.324 The major direction of the QRS complex is usually oriented opposite to that of the T wave.
The R-R intervals may be regular or irregular. The morphology of the QRS complexes may be similar (uniform) or may vary widely with multiform VT (Fig. 30.33). Atrioventricular dissociation is usually present, with an atrial rate slower than the ventricular rate. Fusion beats and capture beats may be detected. VT can be sustained or paroxysmal.The echocardiogram is used to determine whether cardiac disease is present. The echocardiogram is usually abnormal in large animals with primary myocardial disease and normal in large animals with secondary VT, except for the changes associated with the VT itself (see Fig. 30.15). Abnormal echocardiographic findings that may be detected in large animals with primary myocardial disease include myocardial dyskinesis, hypokinesis, and akinesis; abnormal myocardial echogenicity; decreased FS, ET, and EF; loss of the normal systolic and diastolic undulations of the aortic root; and detection of spontaneous contrast, small aortic root, and large pulmonary artery. Occasionally the echocardiographic abnormalities created by VT may be difficult to distinguish from those of primary myocardial disease. Rupture of the aortic root at the right sinus of Valsalva should be considered in horses with acute onset of uniform VT and colic.
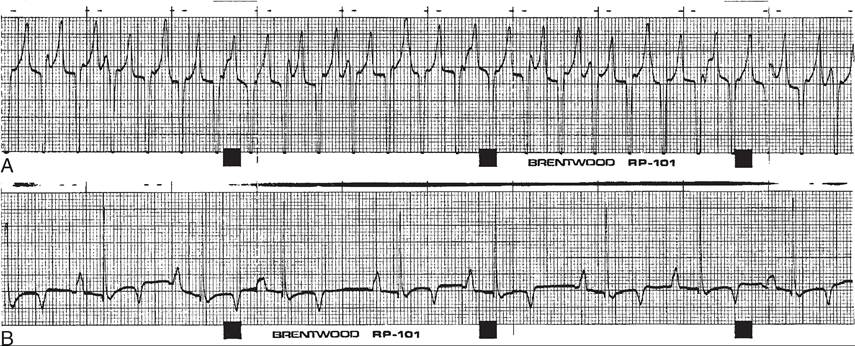
FIG. 30.32 Lead II electrocardiogram obtained from a horse with sustained uniform venticular tachycardia (VT) and congestive heart failure before (A) and after (B) conversion to sinus rhythm. Note the abnormal QRS and T configuration and slower atrial rate during the sustained VT.
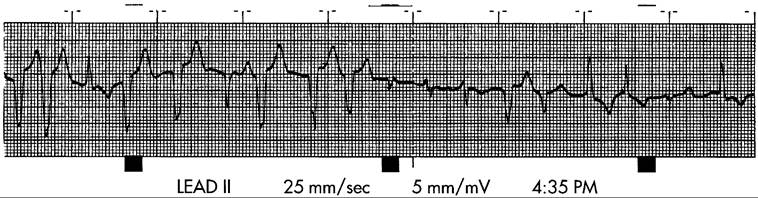
FIG. 30.33 Lead II electrocardiogram obtained from a horse with multiform ventricular tachycardia and acute onset of pulmonary edema. Note the multiple different QRS and T configurations and the elevated ventricular rate.
Cardiac catheterization may reveal severe hypotension and low cardiac output.
In healthy ponies with pacing-induced VT, stroke volume decreased significantly when the ventricle was paced at 150, 200, and 250 bpm.333 Mean left atrial pressure, mean pulmonary arterial pressure, and right ventricular systolic pressure increased significantly when the ventricle was paced at 220 and 250 bpm. Aortic pressure and cardiac output decreased in these ponies at 250 bpm, but the decrease from resting values was not statistically significant. Myocardial perfusion in the papillary muscles and subendocardium decreased significantly with pacing-induced VT at a rate of 250 bpm. Decreases in cardiac output, arterial blood pressure, and myocardial perfusion are even more marked in animals with underlying myocardial disease or multiform VT, as are the changes in left atrial, pulmonary arterial, and right ventricular pressure.Pathophysiology
VT is probably initiated spontaneously by late coupled ventricular complexes, whereas one very early ventricular premature depolarization can often initiate VT electrically.323 Sympathetic stimulation may also provoke VT by increasing the amplitude of the early afterdepolarizations, culminating in a run of VT.323 This may be the mechanism of some of the exercise-induced VT in horses. Reentry in the ventricle is an important cause of sustained VT, particularly in human patients with dilated cardiomyopathy and ischemic heart disease. The area of reentry is reportedly small (drug for most large animal practitioners—is rapidly acting, administered IV, and has a short duration of action and minimal hemodynamic effects. However, this drug has central nervous system side effects in horses (hyperexcitability and seizures) and must be used at a lower dosage than in cattle. Quinidine gluconate (or quinidine sulfate in cattle) is effective in large animals but is less rapidly acting, has negative inotropic effects at large doses or if primary myocardial disease is present, causes hypotension, and can produce undesirable adverse or toxic reactions. Magnesium sulfate can cause hypotension but has no other recognized adverse cardiovascular effects. It is less rapidly acting than lidocaine, but in both normomagnesemic and hypomagnesemic patients it may be effective when other antiarrhythmics fail. IV procainamide, IV and oral propafenone, and IV flecainide have also been used successfully in horses with VT. IV propafenone is indicated for refractory VT and has been used successfully in several horses that did not respond to lidocaine, quinidine, procainamide, or magnesium sulfate. However, it is currently unavailable in the United States. Sotalol has been successful in several horses with VT and is available in an intravenous formulation.339 Other antiarrhythmics such as propranolol have been used with less success but have converted large animals with sustained VT.