Atrial Fibrillation
Definition and Etiology
Atrial fibrillation (AF) is a cardiac arrhythmia characterized by a lack of coordinated atrial electrical activity. It is caused by an abnormality of impulse conduction that results from multiple small rapid and random reentrant activation of the atria or by one or more discrete rotors.
High resting vagal tone, commonly found in horses, shortens the action potential duration in atrial myocardial cells, making AF more likely to occur. AF can occur in the presence of atrial enlargement from atrial myocardial disease, atrioventricular valvular regurgitation, ventricular failure, myocarditis, endocarditis, autonomic nervous system imbalance, electrolyte or acid-base disturbances, anesthetic drugs or tranquilizer administration, unknown causes, or in the absence of detectable underlying cardiac disease (“lone” AF). Although “lone” AF has been a term used when no underlying cardiac disease can be found, in all likelihood, underlying atrial myocardial disease is present at the microscopic level that we are currently unable to detect.Clinical Signs and Differential Diagnosis
Large animals with AF may be asymptomatic at rest, and AF may be detected as an incidental finding in an otherwise normal horse. Horses that perform in rigorous athletic events usually have a history of exercise intolerance or poor performance. Other complaints may be exercise-induced epistaxis, respiratory disease, weakness, syncope, myopathy, colic, or CHF. Cattle with AF usually have underlying GI disease.280,281 Atrial premature depolarizations have also been reported in cattle with GI disease and may be a prelude to the development of AF.281 Foot rot, pneumonia, and endocarditis have also been associated with AF in cattle. Anorexia and decreased milk production are common in cattle with AF. AF and the clinical signs associated with it in horses and in cattle can be paroxysmal.
Paroxysmal AF usually lasts no more than 24 to 48 hours before spontaneous conversion to sinus rhythm occurs.282 Spontaneous conversion usually occurs in horses with small atria and an otherwise normal heart or in cattle with correction of the underlying problem. Transient potassium depletion associated with the administration of furosemide is a common cause of paroxysmal AF in horses. Administration of bicarbonate “milkshakes” has also been implicated in horses with paroxysmal AF. AF has also been associated with iatrogenic hyperthyroidism in horses due to the administration of Thyro L or supplements containing kelp or ground-up shellfish.Animals with AF have an irregularly irregular cardiac rhythm. In horses with AF, there is a high degree of underlying periodicity.283 Heart sounds vary in intensity, and no fourth heart sound is audible. The heart rate may be slow, normal, or elevated. In cattle with severe abdominal disease, the heart rate usually reflects the severity of the underlying disease. In horses the resting heart rate is usually normal to slightly elevated and is rarely above 50 beats per minute (bpm) unless there is underlying myocardial or valvular disease or the horse has another reason for tachycardia (colic, etc.). During exercise, horses with AF develop abnormally high heart rates that are usually 40 to 60 bpm higher than expected for each level of exercise, far exceeding the peak heart rate of 240 bpm at maximal exercise.284-286 The arterial pulse varies in intensity. A pulse deficit occurs when two beats occur in rapid succession and is infrequent unless the heart rate is elevated. Cardiac murmurs of grade 3/6 or louder are present in less than 50% of the horses and in even fewer cattle with AF.287-289 Signs of CHF (peripheral edema, jugular venous distention) may be present in some animals, but they are not caused by the arrhythmia. In these cases, AF occurs secondary to the atrial enlargement that occurs with the underlying valvular or myocardial disease.
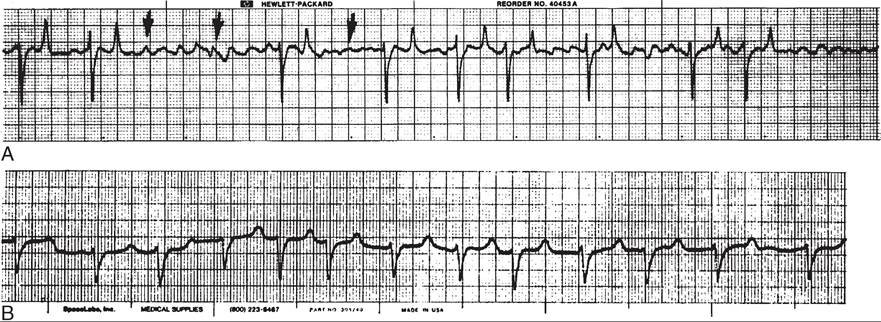
FIG. 30.31 Electrocardiograms showing atrial fibrillation in a horse (A) and cow (B). The irregular QT intervals and absence of P waves are apparent. Arrows point to fibrillation waves, which are apparent only in A.
Absence of an auscultable fourth heart sound in the presence of an irregular cardiac rhythm with no underlying regularity distinguishes AF from other cardiac arrhythmias. Sinus arrhythmia, which is also an irregular rhythm, has an audible fourth heart sound. Second-degree AV block, which is usually a regularly irregular rhythm, also has an audible fourth heart sound. However, underlying sinus arrhythmia is usually present in these horses, making it more difficult to distinguish second- degree AV block with sinus arrhythmia from AF. Any increase in sympathetic tone, such as occurs with exercise or excitement, should result in a regular rhythm in horses with second-degree AV block while those with AF will have persistent irregular rhythm. Ventricular and atrial ectopic beats usually occur with a relatively regular underlying rhythm. A complicated ventricular rhythm with more than one focus of activation may have characteristics similar to those of AF and must be distinguished from it by an ECG. Atrial tachycardia with varying degrees of atrioventricular block has similar auscultatory characteristics, and the underlying fourth heart sounds may be missed if the animal is auscultated in a noisy environment.
Clinical Pathology
In cattle with AF, acid-base and electrolyte disturbances occur frequently and are most likely attributable to the underlying primary disease. Most cattle with AF have GI disease, and the most consistent acid-base disturbance is metabolic alkalosis.289 Hypocalcemia, hypokalemia, and hypochloremia may also be seen in cattle with AF. Experimental induction of metabolic alkalosis with hypokalemia in cattle has been associated with development of AF.290 Most horses with AF have normal electrolytes, although the fractional excretion of potassium may be low, particularly in horses that sweat excessively or are routinely receiving furosemide for exercise-induced pulmonary hemorrhage.
cTnI may be elevated in horses with acute AF, particularly if the sample was obtained 4 to 6 hours after the onset of AF. In most horses, this will decrease rapidly in next day or two following the onset of AF. If the cTnI continues to climb or is very high, active myocardial disease should be suspected. Elevations of T3 or T4 may be present in horses that have been receiving supplements containing kelp, shellfish, or Thyro-L.The diagnosis of AF is made by ECG. The arrhythmia is characterized by an irregular R-R interval. The ventricular response rate is low, normal, or high, depending on the presence of heart disease or the severity of the primary disease. The ventricular complexes have normal polarity and amplitude but vary slightly in appearance from beat to beat. Similarly, the QT interval and appearance of the T wave vary. P waves are absent, replaced by fine undulations of the baseline called fibrillation or f waves. In some leads the f waves are barely visible, particularly in cattle (Fig. 30.31). In some cases, atrial flutter may be present with larger saw-tooth baseline undulations called flutter or F waves.
The echocardiogram is used to determine whether cardiac disease is present. The most significant change associated with the arrhythmia is a mild reduction in shortening fraction (24% to 28%) that occurs, in part, secondary to the loss of the atrial contribution to ventricular filling.291 Absence of the second (atrial) opening of the mitral valve, corresponding to atrial contractions, is also detected with AF.292 Conversion to sinus rhythm usually results in these echocardiographic findings returning to normal within several days if there is no underlying myocardial disease.291,293 Similar improvement occurs in horses with MR and AR after conversion to normal sinus rhythm.293 In many large animals with AF, no evidence of heart disease can be detected echocardiographically; these animals are often considered to have “lone” AF.
However, both electrical and structural remodeling of the atria occur in the horse with AF, which, although reversible early on, contributes to the persistence and recurrence of AF.294-296Abnormal echocardiographic dimensions, if detected, indicate that underlying heart disease is present. Measurement of the maximal left atrial dimension in the two-chambered view of the left atrium and left ventricle from the left cardiac window should be performed in peak systole to determine whether there is left atrial enlargement. This measurement is a more sensitive indicator of left atrial enlargement than the M-mode left atrium-to-aortic root ratio. In normal Standardbred and Thoroughbred horses, the left atrial diameter in this view should be 13.5 cm or less. Measurement of the left atrium- to-aortic root ratio can be performed in the 2D short-axis view of the aorta across the maximal short-axis diameter of the left atrium to obtain additional information about left atrial size.24 Measurement of the maximal diameter and area of the left atrium can also be performed in the four-chambered view in peak systole if the heart can be imaged in its entirety.24
Cardiac catheterization reveals normal cardiac output and blood pressure measurements in most awake horses with AF, but conversion to normal sinus rhythm may induce a reduction in mean right atrial, pulmonary arterial, and aortic pressures.297 Similar studies have not been reported in cattle.
Pathophysiology
Experimentally, rapid stimulation of the atrium can initiate AF, which can be sustained if the animal has a large heart and sufficient vagal tone.281,298-301 In horses and cattle the normal atria may be large enough to support AF once it is established. In addition, both species have a high vagal tone at rest. This combination of factors may be responsible for the large number of benign or functional cases of AF in large animals. The ventricular response during AF results from rate-dependent concealment of AF wavelets bombarding the AV node.283 Cardiac diseases such as endocarditis, atrioventricular valvular regurgitation, and CHF that result in atrial enlargement and rapid stimulation of the atria provide a setting in which AF can develop and can be sustained naturally.
Microscopic cardiac pathology might also create the proper setting for the development of conduction block and reentry.During AF there is no coordinated contraction of the atria, so ventricular filling is passive. Although this might be expected to reduce cardiac output, there is no evidence this occurs in resting horses without concurrent MR or AR.297 In several horses with AR or AR with MR, a decreased cardiac output was detected compared with horses without valvular insufficiencies before conversion.293 The cardiac output increased significantly in warmblood horses with valvular regurgitation after conversion. During exercise, however, the heart rate of horses with AF exceeds normal limits, often by 40 to 60 bpm for each level of exercise. This results in a decreased cardiac output and the resultant exercise intolerance that occurs in horses performing high-intensity athletic work. Even higher heart rates were reported in warmblood horses during lungeing exercise, with the majority of these horses exhibiting QRS complexes with abnormal morphology during exercise.302 Blood flow to other organs and viscera, although not studied, may be altered in large animals with AF, resulting in reduced GI motility, colic, reduced muscle blood flow, and poor milk production.
A,ι 1 ι,ι ∙ia τ^,297 303 C1 ’1
Atrial pressures are elevated in horses with Ah.29',303 Sustained high pressure is likely to produce dilation of the atria. With progressive dilation, secondary atrioventricular valve regurgitation may occur. During AF, blood flow to the atrial myocardium is reduced, and progressive fibrosis can also be a consequence of chronic AF. Sustained AF may result in progressive cardiac disease, although it is usually well tolerated in the horse.
Epidemiology
Standardbred, Thoroughbred, and draft horses have been reported to have the highest incidence of AF.285,28',288 Racehorses have been diagnosed most frequently, but AF has been found in all types of horses.287,288,293 Horses of all ages are susceptible to AF, but it occurs infrequently in ponies, foals, weanlings, and yearlings. Older horses, ponies, foals, weanlings, and yearlings with AF more frequently have underlying heart disease associated with the arrhythmia.
In cattle, AF is diagnosed more frequently in dairy cattle than in beef cattle, but there is no apparent breed predilec- 280289
tion., It is commonly associated with GI disease or abdominal pain in cattle.280,281,289 Foot rot and pneumonia can also be associated with development of AF in cattle.
Necropsy Findings
Many cattle and horses have “lone” AF without apparent underlying heart disease, so the necropsy findings reflect the primary disease. Microscopic cardiac pathology has been found in horses with AF that consists of focal atrial myocardial fibrosis, microvascular alterations, and cardiac nerve abnormalities.304-306 Multifocal or large areas of myocardial fibrosis were detected in dairy cows with idiopathic AF.307 Whether these changes predisposed to the development of AF, were a consequence of AF, or were aging changes has not been established. A minority of horses and cattle have endocarditis, CHF, or valvular lesions, and the necropsy findings reflect these conditions. In horses with AF, mitral valve disease was the most common valvular lesion.288 Pharmacologic and transvenous electrical cardioversion (TVEC) are both options for conversion of AF to normal sinus rhythm in horses.288,308-319
Treatment and Prognosis
Quinidine is the drug of choice for pharmacologic conversion of AF to normal sinus rhythm in horses and cattle. The drug is a negative inotrope at high dosages, causes systemic hypotension, increases the ventricular response rate, and can produce undesirable side effects and toxicity—it must be used with caution. In animals with CHF, quinidine therapy has considerable risk.288 Because most large animals have little or no underlying cardiac pathology, treatment with quinidine is usually successful in restoring normal sinus rhythm. Treated animals should be monitored frequently by physical examination, with careful auscultation and ECG recording. Continuous ECG recording using radiotelemetry should be performed throughout treatment.311 Animals should have normal acid-base balance and electrolyte concentrations before treatment. They should be adequately hydrated, allowed to drink and eat, or given additional oral fluids (horses) or IV fluids (cattle) during therapy. IV administration of quinidine gluconate is successful in converting horses with recent-onset AF to sinus rhythm.312 Quinidine gluconate is most successful when administered to horses with AF of 2 weeks or less. However, quinidine gluconate had been successful in converting horses with AF of 2 to 4 weeks’ duration. Horses with longer durations of AF should be treated with quinidine sulfate via nasogastric intubation. Quinidine is poorly absorbed after oral administration to cattle, so it must be given by IV infusion to obtain therapeutic concentrations. Cattle should be given IV fluids during quinidine infusion. Quinidine therapy should always be discontinued when conversion to normal sinus rhythm occurs.
Quinidine sulfate is the preparation most economically used in large animals, although quinidine gluconate has resulted in successful conversion of a cow with AF.320 Before therapy, a baseline ECG is recorded. Horses are given a dose of 22 mg/ kg of body weight in a suspension of water via nasogastric tube. At 2 hours (when blood concentration of quinidine should have peaked), they are evaluated closely for idiosyncratic or toxic reactions, such as nasal edema, cutaneous reactions (urticaria or wheals), laminitis, colic, marked diarrhea, or ataxia. An ECG is recorded. If conversion to normal sinus rhythm has not occurred and the QRS duration is not greater than 25% of the pretreatment QRS duration, and none of the aforementioned abnormalities have occurred, another dose is administered. Two hours after each dose is administered via nasogastric intubation, an ECG is recorded. If there has been no conversion to normal sinus rhythm and the horse is not exhibiting toxic or adverse reactions to quinidine, another dose is administered, up to a maximum of four doses. A plasma quinidine concentration should be obtained 1 hour after the fourth dose administered every 2 hours to be sure the horse will be able to tolerate another dose without experiencing toxicity. If the QRS complex is prolonged by more than 25% of the pretreatment value or if a fast (>80 to 100 bpm) sustained supraventricular arrhythmia, ventricular rhythm, colic, marked diarrhea, ataxia, nasal edema, or laminitis develops, therapy should be discontinued. Although laminitis is a frequently reported complication of quinidine sulfate therapy in the older literature, the actual incidence of laminitis associated with quinidine administration is rare.311 Nasal mucosal edema, neurologic signs, and prolongation of the QRS duration to greater than 25% of the pretreatment value are all signs of quinidine toxicity; if detected, the drug should be discontinued. Colic associated with high dosages of quinidine should also prompt discontinuation of treatment (at least for this attempt at conversion). If conversion has not occurred after a total of four to six doses (one every 2 hours) or after a cumulative dose of 88 to 132 mg/kg of quinidine sulfate has been administered, treatment intervals should be prolonged to every 6 hours (approximate half-life of quinidine).311 Only four doses of quinidine sulfate should be administered every 2 hours before switching to every 6 hours if plasma quinidine concentrations cannot be obtained in a timely fashion. The every-6-hour treatment can be continued until the horse converts or shows toxic or adverse side effects or the owner elects to discontinue treatment. The advantage of this treatment regimen is that steady-state plasma and myocardial concentrations of the drug are usually achieved. There is less quinidine toxicity, a lower total dose of quinidine sulfate is used, and horses that did not convert after the standard every-2-hour administration may convert with this treatment regimen. Digoxin at 11 μg∕kg PO twice daily can then be added to the therapeutic regimen if conversion has not occurred in 24 to 48 hours; it appears to be helpful in some horses.311 Concurrent administration of digoxin and quinidine will result in an increased plasma digoxin
O Tl,,, Jr O
321
concentration,321 so to prevent digoxin toxicity, concentrations should be monitored beginning the second day of combined quinidine and digoxin therapy. If this is not possible, the horse should not receive more than 2 days of combined digoxin and quinidine therapy.
TVEC has been successful in converting horses to normal sinus rhythm and is the preferred treatment for equine AF in some hospitals with the necessary equipment and specialists trained in this procedure. TVEC is particularly useful in horses in which adverse or toxic reactions to quinidine prompted discontinuation of antiarrhythmic therapy with the result that conversion to normal sinus rhythm was not achieved.316,319 TVEC is also the treatment of choice for horses that have marked resting tachycardia or excessively high heart rates. TVEC is also a good option for those with aberrant conduction or VA with sympathetic stimulation or exercise.
Quinidine sulfate at a dose of 48 mg/kg is suspended in 4 L of saline or lactated Ringer solution when cattle are treated for AF. This dose is administered at a rate of 1 L/h. IV fluids are administered simultaneously in the opposite jugular vein. Cattle should be monitored continuously during the infusion. Cattle frequently become depressed and develop diarrhea during the infusion of quinidine. These signs are side effects, and therapy can be continued. The infusion rate should be slowed if the ventricular response rate exceeds 100 bpm. If the QRS complex is visibly prolonged or a fast (>120 bpm) supraventricular arrhythmia or ventricular rhythm develops, therapy is temporarily discontinued. Just before conversion, some cattle have blepharospasm and are ataxic. The infusion should be discontinued as soon as conversion occurs. Therapy should be discontinued after the 4 L infusion even if conversion to normal sinus rhythm has not occurred.
During quinidine therapy the ECG shows predictable changes. The fibrillation waves become coarser and less frequent. The R-R interval becomes more regular as the heart rate increases. Before conversion there may be a rapid regular atrial rate with more than one saw-toothed flutter (F) wave or P wave for each QRS complex (atrial flutter or atrial tachycardia with atrioventricular block, respectively). At the time of conversion, a single P wave is present for each QRS complex. Frequently a large Ta wave is present and the ST segment is elevated. The ECG should be normal within 12 hours of conversion. A continuous 24-hour ECG is recommended in horses with AF after conversion to determine whether frequent atrial premature depolarizations are present. If the continuous ECG is normal and left atrial and ventricular function has returned to normal, the horse can be returned to training. If frequent trial premature complexes (APCs) are detected or left atrial contractile dysfunction persists, the horse should be rested and treatment with corticosteroids or antiar- rhythmics considered. The horse should not be returned to work until the APCs have resolved and left atrial contractile function has returned to normal. IV amiodarone and flecainide have been used to convert horses with AF,314,315,317 but amiodarone is less successful than quinidine for this purpose.314,317 VA was common in horses given flecainide, limiting its usefulness as a treatment for AF in horses.315
The resting ventricular response rate should be less than 60 bpm in horses and 100 bpm in cattle before quinidine therapy. TVEC is the preferred treatment in horses with high resting heart rates and high heart rate responses to stimulation or during prior quinidine therapy. Digoxin is recommended before quinidine therapy in horses where TVEC is not an option and in cattle with fast heart rates. One or two doses of digoxin (11 μg∕kg PO twice daily) are administered before initiation of quinidine therapy in horses with only mild tachycardia. In horses with very labile heart rates or problems with rapid ventricular response rate during a previous conversion, digoxin can be administered for up to 5 to 7 days before initiation of quinidine therapy. Cattle are given digoxin by IV infusion at 0.86 μg/kg/h or 11 μgZkg three times daily. The side effects of quinidine treatment (e.g., rapid ventricular response rate) may be decreased in animals pretreated with digoxin. Digoxin is also indicated as a pretreatment in horses with AF and very low FS (exercise, if possible. Their heart rates should not exceed 220 bpm at the maximal exercise desired. Heart rate control with oral digoxin or sotalol have been used to slow the ventricular response rate during exercise, but more work is needed to determine the efficacy and safety of this long term.322 Those with aberrant conduction and multiform VA during exercise should be retired from ridden or driven work.118
More on the topic Atrial Fibrillation:
- Atrial Fibrillation
- CHAPTER MENU
- Specific Heart Diseases
- Performing the Electrocardiogram
- References
- REFERENCES
- Abnormal Peripheral Pulse
- gastric Dilatationvolvulus syndrome
- Exercise Intolerance and Poor Performance in Horses
- Diagnosis of Cardiovascular Disease by Presenting Sign