Verminous Meningoencephalomyelitis
Robert J. MacKay
Verminous meningoencephalomyelitis is caused by the meander- ings of one or more parasites through the CNS and is therefore an extremely variable clinical entity.
Depending on the number, size, and location of the parasites and the duration of their migration through the brain or spinal cord, a spectrum of signs is possible, ranging from a nonprogressive localizing neurologic deficit to rapidly fatal, diffuse encephalitis. Verminous meningoencephalomyelitis usually occurs sporadically and has been associated with strongylid (Strongylus vulgaris), metastrongylid (Angiostrongylus cantonensis, P. tenuis), filarid (Setaria spp.), tylenchid (formerly rhabditid; Halicephalobus gingivalis), and spirurid (Draschia megastoma) nematodes, as well as warble fly larvae (Hypoderma spp.).Strongylus Vulgaris
Verminous myeloencephalitis due to S. vulgaris in the CNS is a rare, aberrant event resulting from embolization to the CNS of L4 or L5 larvae from verminous thrombi in the left ventricle, proximal aorta, or any of the aortic branches that supply the CNS.1,2 S. vulgaris larvae in the aorta migrate subintimally upstream from locations in the proximal cranial mesenteric artery.2 As a result of disintegration of thrombi in these aberrant locations, clot fragments and larvae migrate to the CNS. Three outcomes are possible: (1) acute massive infarction, ischemia, and edema of the brain; severe neurologic dysfunction; and death after a brief clinical course; (2) nonlethal or even subclinical embolization of the CNS that is followed by entry of one or more larvae into the CNS parenchyma, which wander therein for up to several months, producing associated neurologic signs; or (3) subclinical embolization and parasite migration. Subclinical larval migration occurs in relatively forgiving parts of the cerebral hemispheres and ends when the parasite dies or migrates out of the CNS.
A single larva can migrate through many levels of the CNS; in one case, an L5 S. vulgaris larva was estimated to have traveled 8 cm per day for several days along the spinal cord of a donkey.3 Virtually any clinical sign is possible, and signs are likely to change dramatically over time or even stop and then restart or spontaneously resolve. A larva may exit the CNS only to reenter at a different location and continue its migration. The donkey mentioned earlier was paraparetic and sitting like a dog because of larval damage through the midlumbar spinal cord; signs improved for a few days when the larva migrated out of the spinal cord, but then the animal collapsed into recumbency when the larva reentered and migrated within the cervical spinal cord.3 Thrombosis, infarction, and tortuous hemorrhagic or discolored tracts may be evident on gross examination. Microscopic findings include linear tracts of hemorrhage lined by neutrophils, macrophages, occasional eosinophils, and reactive glial cells. CSF changes associated with S. vulgaris migration include xanthochromia, protein concentration ranging from 32 to 550 mg∕dL, and increased nucleated cell count (42∕μL to 10,000∕μL).1-4 The differential counts range from 70% to 80% neutrophils, 12% to 19% mononuclear cells, and 1% to 2% eosinophils. Verminous myeloencephalitis due to S. vulgaris virtually disappeared after the introduction of the macrocyclic lactone anthelmintics in the 1980s; however, the increasing practice of selective deworming may enable the reemergence of large strongyles.5
Hypoderma Lineatum and Hypoderma Bovis (Cattle Grubs)
Hypoderma lineatum (common cattle grub) and Hypoderma bovis (northern cattle grub) are parasites of cattle that occasionally migrate in the horse (also in goats and deer). In the late spring or early summer, adult Hypoderma spp. flies (known as warble flies or heel flies') deposit eggs on hairs on the limbs or lower body.
First-stage larvae hatch in 5 to 7 days, penetrate the skin, and migrate in a dorsal direction along fascial planes, often following the paths of blood vessels or nerves.6 Over approximately 1 year, migrating larvae moult once or twice and arrive in subcutaneous tissues along the back. Their dorsally directed path may sporadically take larvae through the foramen magnum or other foraminae of the skull to penetrate and meander in the brainstem. Because of the large size of Hypoderma spp. larvae and their propensity for migration within the caudal fossa of the skull, neurologic signs are usually severe, progressive, and fatal.6,7 Typically, affected animals exhibit profound obtundation and signs of asymmetric cranial nerve dysfunction (e.g., head tilt and circling) that worsen quickly and lead to recumbency and death. Since the advent of pour-on and injectable systemic organophosphate insecticides in the 1950s and macrocyclic lactones in the 1980s for systematic treatment of cattle, Hypoderma populations have decreased dramatically in the United States and have been eradicated in several European countries, and so intracranial myiasis is now unlikely to occur in industrialized countries. Hypoderma diana, a parasite of deer, has also infested horses and presumably has the potential for CNS invasion.8Halicephalobus Gingivalis
H. gingivalis (previously Halicepbalobus deletrix, Micronema deletrix) is a free-living microbivorous tylenchid nematode that feeds on bacteria in rich organic environments such as decaying vegetation, compost, or manure.9,10 Cases of meningoencepha- lomyelitis caused by H. gingivalis occur sporadically worldwide in equids (including zebras) and occasionally in humans and cattle.11-17 The nematode opportunistically enters the body through breaks in the mucous membranes (and possibly skin) of the nose, mouth, prepuce, and mammary gland of horses and invades and proliferates locally to cause clinically apparent granulomas.18-23 Such masses can be locally invasive and destructive, particularly in the jaws, nasal cavity, and paranasal sinuses.18,24 In one case a foal was apparently infected by suckling from its dam, which had H.
gingivalis mastitis.25 From these superficial sites, larvae or adults may enter lymphatic or venous drainage and be distributed hematogenously to various organs and tissues.H. gingivalis has a propensity to invade and proliferate in the kidneys (Fig. 35.20), CNS, and eyes, but lesions have also been found in long bones, the heart, the lungs, the liver, the uterus, the testes, lymph nodes, and the walls of the aorta and pulmonary arteries.23,26-28 The brain is the usual site of CNS infection, with lesser involvement of the spinal cord or, in one instance, the cauda equina.29 The typical severe progressive neurologic signs are due to massive proliferation of nematodes adjacent to blood vessels and the associated florid perivascular granulomatous inflammation.9 Only female nematodes are present in lesions, and reproduction is by parthenogenesis.9
Clinical signs of H. gingivalis infection of the CNS depend on the location of the lesions and include asymmetric ataxia, hypermetria in the thoracic limbs, obtundation, behavioral changes, compulsive walking, head pressing, head tilt, circling, nystagmus, recumbency, convulsions, and coma.12-17,30-32 H. gingivalis meningoencephalitis is invariably fatal, regardless of treatment; affected horses die or are euthanized within several days of onset.26,33 CSF analysis in affected horses ranges from normal to xanthochromic appearance with increased protein and mild to moderate pleocytosis of nucleated cells. Differential analyses reveal mostly mononuclear cells with lesser numbers of neutrophils and occasional eosinophils. In many (possibly most) cases of H. gingivalis meningoencephalitis, the animals also exhibit characteristic renal lesions.26 The latter are usually multifocal large nodules in the renal parenchyma of one or
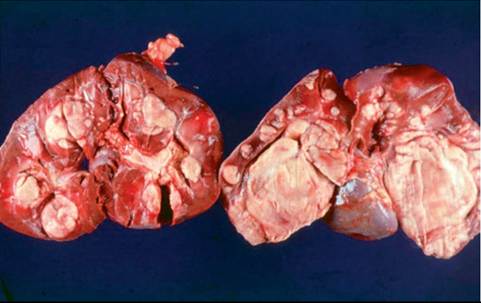
FIG. 35.20 Kidneys from a horse with disseminated Halicephalobus gingivalis infection, including fatal meningoencephalomyelitis.
both kidneys.26,34 Of potential diagnostic significance in such cases are a history of weight loss, hematuria, or polyuria, or a combination of these, and findings at initial examination of nematodes in the urinary sediment, high serum creatinine and calcium concentrations, and ultrasonographically evident renal masses.35-38 Severe progressive, usually unilateral verminous chorioretinitis or panophthalmitis may precede or coincide with the onset of signs of encephalitis.37,39,40 Efforts to eliminate subcutaneous or renal H.
gingivalis infections by surgery and anthelmintics are occasionally successful21 but, unfortunately and unpredictably, are often followed within several days to weeks by the onset of encephalitis.19,39,41-43Parelaphostrongylus Tenuis
P. tenuis (the meningeal worm) is a ubiquitous parasite of white-tailed deer in the eastern United States (north of a line through the middle of the states along the Gulf of Mexico44). Infective larvae are ingested within infested snails and slugs, exit through the abomasum, and then migrate to the dorsal horn of the gray matter of the spinal cord, where they mature into adults before traveling along the dorsal nerve roots to the venous sinuses and subarachnoid spaces over the cerebral hemispheres. P. tenuis is increasingly a cause of verminous meningoencephalomyelitis due to aberrant larval migration in the CNS of other cervids, goats, sheep, and New World camelids within the same geographic range. In 2003, six equine cases with cervical scoliosis were described.45 In each case, a unilateral multisegment contiguous lesion involved the dorsal horn of the gray matter on the convex side of the neck. In one case, cross-sections of a metastrongylid nematode were associated with the characteristic lesion, and the presumption is that all cases were caused by aberrant migration of P. tenuis. Five of the horses were younger than 1 year, and each exhibited acute onset of severe scoliosis after a variable prodrome with degrees of hypalgesia of the neck and cranial thorax, limb weakness, and limb ataxia, all on the side of the cervical convexity. Treatment with anthelmintics and antiinflammatories had no effect, and all affected animals were euthanized for humane reasons. An additional case, also in a young horse, was reported in 2007, this time with signs of obtundation, head tilt, circling, quadriparesis, and ataxia in all four limbs.46 Numerous larval stages, eggs, and occasional adults of both sexes were associated with granulomatous eosinophilic inflammation in the cerebellum and adjacent brainstem.
Presence of P tenuis has been confirmed by PCR in lesions from the brain and spinal cord.47,48 A P tenuis nematode was extracted from the anterior chamber of a horse with signs of anterior uveitis.49Angiostrongylus Cantonensis
A. cantonensis is a neurotropic metastrongylid parasite with a life cycle in rats closely analogous to that of P tenuis in whitetailed deer.50 It has long been endemic in the Pacific islands and Southeast Asia, but its range has spread into Australia, the United States, and the Caribbean. It is now well established among the wildlife of Louisiana.51 The definitive hosts are species of wild rats that become infected by ingesting the infective larvae in slugs or snails. The larvae migrate to the CNS to continue development before finishing the life cycle via the pulmonary vasculature. Inadvertent ingestion of infective larvae by atypical hosts such as humans, dogs, and horses may lead to aberrant migration in the CNS and signs of verminous meningomyeloencephalitis similar to those described earlier for S. vulgaris. Equine cases have been reported in two foals in Australia and an American Miniature Horse foal in Louisiana.52,53 Larvae migrated in the gray and white matter of the spinal cord and brainstem. CSF analysis revealed mild pleocytosis with small numbers of neutrophils and eosinophils. Specific ELISA tests are available for testing of CSF in humans and dogs.50
Draschia Megastoma
D. (Habronema) megastoma is a spirurid nematode that has been found in the brainstem of a horse from the southern United States.54 The adult worm is normally embedded in benign Pyogranulomatous masses in the equine stomach, but larvae can invade wounds to cause granulating summer sores and have been reported to cause pulmonary nodules. The two unusual features of the solitary report of encephalitis are, first, the parasite found at necropsy was an adult gravid female and, second, there was a quiescent period of 6 weeks during the clinical course when clinical signs improved before the horse's condition deteriorated again.
Setaria Species
Setaria spp. are long, threadlike filarid nematodes that live without causing adverse effect in the peritoneal cavities of animals worldwide.55 Microfilariae are released into the blood of the host and acquired by feeding mosquitoes, in which they undergo development to infectious larvae. Bovids outside the Americas are hosts to several setarial nematodes, including Setaria digitata, Setaria Iabiatopapillosa, and Setaria marsballi.56~558 When inserted by mosquitoes into atypical hosts such as horses, goats, and sheep, immature S. digitata nematodes may migrate aberrantly through the CNS and other organs of atypical hosts.57,59 This parasite has also migrated aberrantly in the CNS of cattle.60 Outbreaks of so-called epizootic cerebrospinal nematodiasis, lumbar paralysis, or kumri occur during the summer or autumn when mosquito intermediate hosts are active. Outbreaks have been reported in Japan, Taiwan, China, Korea, Sri Lanka, Burma, India, Nepal, Iran, Israel, and Saudi Arabia.57,59,61,62 Cases in horses are sporadic and often involve older horses; in goats, young animals are usually affected, and morbidity and mortality rates are up to 100%.57 S. digitata apparently does not occur in the United States56; however, a single case of verminous encephalomyelitis due to S. labiatopapil- losa has been reported in this country.63
Clinical signs are variable and are related to mechanical and inflammatory destruction along the tracks left in the brain or spinal cord by one or more larvae.59,64 In this regard, the pathologic features of setarial meningoencephalomyelitis are identical to those described earlier for S. vulgaris. Changes in the CSF associated with Setaria infestation include xanthochromia, pleocytosis (25 to 84 cells/uL), and a slightly increased protein concentration. The cells of one horse contained a small proportion of eosinophils and basophils, but this finding was inconsistent with other reports.
■ Treatment and Prevention When single or a few migrating larvae are involved, the use of combinations of anthelmintics and vigorous antiinflammatory treatment has yielded successful outcomes. The latter component is probably important to prevent the effects of strong inflammatory responses against killed parasites.50 Because penetration of the blood-brain barrier by anthelmintics is limited, high-dose benzimidazoles are often used for this purpose. Typical protocols are fenbendazole, 10 to 60 mg/kg by mouth or nasogastric tube, one to five daily doses, with dexamethasone (or equivalent), 0.05 to 0.1 mg/kg IV or IM, once daily for 3 days. Ivermectin was effective in goats with early signs of setarial myeloen- cephalitis57 but has not been effective in treatment of P tenuis or H. gingivalis cases in horses, even when used against H. gingivalis at a potentially toxic dose of 1.2 mg/kg (six times the recommended dose).35 Diethyl carbamazine citrate, 40 to 100 mg/kg daily, was effective in natural and experimental setarial cases in horses.65 Most types of verminous encephalitis are unlikely to occur in horses on a regular deworming program; however, H. gingivalis cases regularly occur in horses on any of a variety of regular anthelmintic regimens.