Weight Loss
The clinical problem of weight loss suggests that an individual large animal patient or a herd has lost weight over a known period of time. It may also suggest that the patient has reached a subnormal adult weight and size (see section on decreased growth and decreased weight gain, earlier).
Late pregnancy, early lactation, and intense exercise are normal physiologic conditions commonly accompanied by mild to moderate weight loss. Late pregnancy can be associated with decreased body condition (Fig. 9.2) without actual weight loss because weight is gained with the conceptus. During pregnancy and lactation the loss of body condition may be mild, resulting in a low normal BCS, or the loss may be severe and can threaten the health of both the dam and neonate.Weight loss in adult animals is most commonly associated with one or more of the following circumstances (other causes are listed in Boxes 9.6 and 9.7):
• Anorexia
• Increased nutrient demands
• PCM
• Micronutrient deficiencies
• Parasitism
Anorexia usually occurs secondary to a primary disease. A decrease in DMI occurs in dairy cows when temperature and humidity (Temperature Humidity Index, THI) exceed the coping mechanisms of the animals.12 Increased nutrient requirements are associated with normal physiologic conditions (e.g., pregnancy, lactation, exercise, cold weather) and pathologic processes (e.g., sepsis, trauma, parasitism, burns). Mild to severe PCM is often associated with inadequate feed quality or quantity but can also be caused by increased energy requirements resulting from adverse environmental conditions. Weight loss can also occur with a deficiency of essential micronutrients such as copper, cobalt (vitamin B12), or vitamin A. Parasitism should always be on the differential list in an animal that has lost weight.
Mechanisms of Weight Loss
Anorexia is the loss of appetite or lack of desire for food; it may be complete or partial.
It is a primary mechanism for weight loss of short or intermediate duration. Weight loss results from decreased nutrient intake. When partial anorexia occurs over a long period, the weight loss may be subtle and go unrecognized. Acute, complete anorexia results in more dramatic rapid weight loss.In domestic species, anorexia is usually associated with a primary disease condition and is regulated by cytokines including interleukin (IL-1) and tumor necrosis factor alpha (TNF-α), released during an inflammatory response.13 Resolution of the primary disease process usually results in a return to voluntary food consumption. Anorexia must be differentiated from dysphagia by observation. The distinction between the conditions that cause anorexia and those that control hunger and satiety is not clear; however, many diseases that cause anorexia also result in dehydration, electrolyte imbalances, and/or acid-base disorders.
In addition to causing anorexia, many disease processes cause an increase in the nutrient requirements for basal metabolism. Nutrient requirements for maintenance, growth, pregnancy, lactation, and exercise have been well defined for many large animal species. Nutrient requirements in disease have not been adequately evaluated in large animals, and most information is currently extrapolated from humans, laboratory animals, and small animal species. In human patients, published estimates indicate that requirements for energy and protein increase approximately 10% after elective surgery, 20% with fractures, 30% to 60% with severe infection or sepsis, 40% with peritonitis, and 50% to 110% with major burns.14,15 In humans, the resting energy expenditure is estimated to increase by 14% for each degree Celsius increase in body temperature.16 Extrapolation of these data directly to equine and ruminant patients is probably not possible; however, the figures do indicate the degree of change in nutrient requirements as a result of disease.
The stress of many disease processes results in an increase in serum cortisol and glucagon. The decreased insulin/ glucagon ratio alters the production of glucose and results in hyperglycemia because of enhanced hepatic gluconeogenesis. An increase in sympathetic activity appears to regulate fat oxidation, the increased release of fatty acids from cellular lipid stores, and the development of hypertriglyceridemia in many patients with sepsis. Protein degradation and a negative nitrogen balance are also hallmarks of the acute response to infection. Weight loss resulting from protein and lipid catabolism is often observed in large animal patients with sepsis, owing to altered metabolic activity and nutrient requirements. In horses, particularly obese ponies or donkeys or pregnant mares, who may be stressed, the increased cortisol coupled with innate insulin resistance may predispose these animals to the development of hyperlipemia and/or hyperlipidemia.In conditions such as burns, peritonitis, pleuritis, colitis, and granulomatous bowel disease, nutrients (particularly proteins) are lost. In many disease conditions, concurrent anorexia and increased nutrient requirements greatly increase the risk of PCM and weight loss. Certain conditions such as Johne's disease in ruminants and granulomatous enteritis in horses are also associated with a malabsorption or malassimila- tion syndrome. In these types of diseases, nutrients are not efficiently digested and absorbed; anorexia may be absent, and dietary intake may appear normal, but weight loss still occurs.
PCM continues to be a persistent problem in domestic animals. Inadequate ingestion of energy and protein obviously
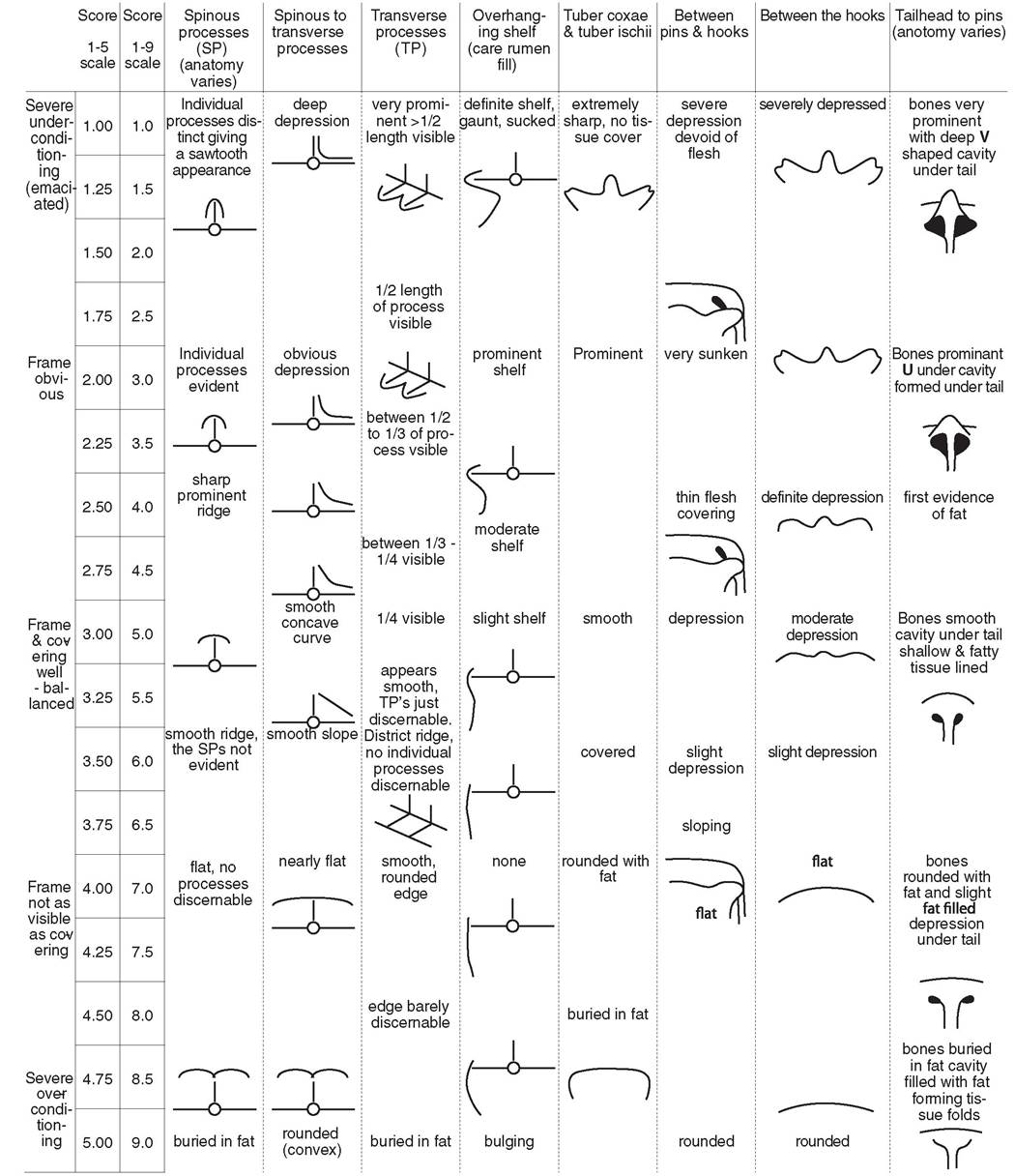
FIG. 9.2 Body condition scoring system for dairy cows. (From Edmonson AJ, Lean IJ, Weaver LD, et al: A body condition scoring chart for Holstein dairy cows. J Dairy Science. 72(1)68-78, 1989.)
| ■ BOX 9.6 | |
| Causes of Weight Loss in Horses | |
| Common Causes | Equine adenovirus |
| Protein-calorie malnutrition (PCM) | Equine infectious anemia |
| Dental disease | Equine viral arteritis |
| Jaw abnormalities | Anhidrosis |
| Gastric ulcers Right dorsal colitis | Uncommon Causes |
| Parasitism (small strongyles, large strongyles, tapeworms, bots) | Botulism |
| Sand enteropathy | Micronema deletrix, infection of the central nervous system |
| Pneumonia (bacterial, viral) | Nigropallidal encephalomalacia |
| Pleuritis, pleuropneumonia, pulmonary abscessation | Nutritional rhabdomyolysis |
| Recurrent airway obstruction | Rabies |
| Internal abdominal abscess | Rectus capitus ventralis muscle rupture |
| Peritonitis | Spinal abscessation |
| Streptococcus equi (lymph node abscessation, pulmonary or | Prognathia, brachygnathia |
| mesenteric abscessation) | Pyloric stenosis |
| Acute renal failure | Basophilic enterocolitis |
| Chronic renal failure | Colonic fistula |
| Pituitary pars intermedia dysfunction | Ileal hypertrophy |
| Neoplasia (alimentary tract) | Strongylus vulgaris, thromboembolism Micropolyspora faeni, hypersensitivity pneumonitis Pleural mesothelioma |
| Less Common Causes | Rhodococcus equi, infection |
| Equine herpes myeloencephalopathy | Tuberculosis |
| Equine motor neuron disease | Mammary carcinoma |
| Oral foreign body | Malignant mesothelioma |
| Guttural pouch infection | Ovarian adenoma |
| Otitis media, interna | Pancreatic neoplasia |
| Paranasal sinus infection | Pulmonary neoplasia |
| Esophageal abnormalities (esophagitis, diverticula) | Skeletal or vertebral neoplasia |
| Vesicular stomatitis | Testicular neoplasia |
| Gastric impaction | Portal vein shunt |
| Gastric squamous cell carcinoma | Liver fluke |
| Duodenal ulcers | Theiler's disease-associated virus (TDAV) |
| Inflammatory bowel disease (basophilic enterocolitis, eosinophilic | Enzootic cystitis |
| enterocolitis, granulomatous enteritis, lymphocytic-plasmacytic | Polycystic disease |
| enteritis, multisystemic eosinophilic epitheliotropic enterocolitis) | Diabetes mellitus |
| Chronic colonic impaction | Hyperparathyroidism |
| Idiopathic diarrhea | Pheochromocytoma |
| Giardiasis | Steatitis |
| Fungal pneumonia | Brucellosis |
| Pneumoconiosis (silicosis) | Multiple cartilaginous exostoses |
| Tuberculosis | Bullous pemphigoid |
| Cholelithiasis | Eosinophilic dermatitis |
| Chronic hepatitis | Fungal granuloma |
| Horsefly-deerfly infestation | |
| Atrial fibrillation | Lupus erythematosus |
| Cardiac or great vessel anomalies | Panniculitis |
| Congestive heart failure | Pemphigus foliaceous |
| Endocarditis, pericarditis | Seborrhea |
| Splenic rupture, abscess | Wound myiasis |
| Amyloidosis | Babesiosis |
| Glomerulonephritis | Erythrocytosis |
| Pyelonephritis | Histoplasmosis |
| Renal neoplasia | Myeloproliferative disease |
| Renal tubular acidosis | Phycomycosis |
| Urinary bladder neoplasia | Tularemia |
| Urolithiasis | Goiter |
| Infectious arthritis | Phosphorus deficiency |
| Osteomyelitis | Thiamine deficiency |
| Granulosa cell tumor Lymphoma, lymphosarcoma | Vitamin A deficiency |
| Malignant melanoma | Toxins |
| Autoimmune anemia or thrombocytopenia | 4-Aminopyridine |
| Purpura hemorrhagica | Aflatoxicosis |
| Coccidioidomycosis | Arsenic toxicity |
| Cryptococcosis | Dioxin |
| Nocardiosis | Fluorosis |
| Agammaglobulinemia | Mercury toxicity |
■ BOX 9.6
Causes of Weight Loss in Horses—cont'd
Pentachlorophenol
Phenylbutazone, flunιxιn meglumine, and other nonsteroidal antiinflammatory drugs
Selenium toxicity
Vitamin D calcinosis
Vitamin K3 toxicity
Zinc toxicity
Plant Toxins
Crofton weed (Ageratina adenophora)
Plant calcinosis (Cestrum diurnum, Trisetum flavescens, others)
Pyrrolizidine alkaloid toxicosis (Senecio spp., Amsinckia spp., Crotolaria spp., others)
Red maple leaf (Acer rubrum)
Jimsonweed (Datura spp.)
White snakeroot (Eupatorium rugosum)
Yellow star thistle (Centaurea solstitialis), Russian knapweed (Centaurea repens)
Exotic Diseases
Besnoitiosis (Besnoitia bennetti)
Burkholderia pseudomallei Dourine (Trypanosoma equiperdum)
Equine dysautonomia (grass sickness) Glanders (Burkholderia mallei)
Mal de caderas (Trypanosoma equinum) Nagana (Trypanosoma spp.)
Stachybotryotoxicosis
Surra (Trypanosoma evansi) Trombiculiasis
Trypanosoma hippicum
| ■ BOX 9.7 | |
| Causes of Weight Loss in Ruminants | |
| Common Causes | Lingual injury, abscess |
| Protein-calorie malnutrition (PCM) | Otitis media, externa |
| Dental abnormalities | Sinusitis |
| Pharyngeal, retropharyngeal abscess | Esophageal malfunctions |
| Actinobacillosis | Omasal impaction |
| Actinomycosis | Abomasal impaction |
| Diarrhea (Enterotoxigenic Escherichia coli, Salmonella, bovine | Colonic obstruction |
| virus diarrhea, coronavirus, rotavirus infection, Cryptosporidium | Aspiration pneumonia |
| parvum, coccidiosis, winter dysentery [B], other causes) | Micropolyspora faeni hypersensitivity pneumonitis |
| Johne's disease (paratuberculosis) | Pleuritis |
| Parasitism (lungworms, gastrointestinal parasites) | Tuberculosis |
| Abomasal ulcer | Brisket disease |
| Displaced abomasum | Endocarditis |
| Subacute ruminal acidosis | Vena caval thrombosis |
| Vagal indigestion | Thymic lymphosarcoma (B) |
| Bacterial pneumonia, pulmonary abscessation | Stomatitis (ulcerative, vesicular, papular [B]) |
| Infectious bovine rhinotracheitis | Glomerulonephritis |
| Traumatic reticuloperitonitis, pericarditis | Urachal abscess, bladder abscess |
| Hepatic abscess | Postparturient hemoglobinuria |
| Liver fluke infestation | Renal amyloidosis |
| Ketosis | Eperythrozoonosis |
| Fat necrosis (B) | Sarcocystosis (B) |
| Leptospirosis | Dermatophilosis |
| Pyelonephritis, cystitis | Psoroptic mange |
| Urolithiasis | Goiter |
| Mammary abscess | Cobalt deficiency |
| Mastitis | Sodium chloride deficiency |
| Anaplasmosis (B) Bovine leukosis | Water deprivation |
| Septic arthritis | Uncommon Causes |
| Lameness (infectious and claw horn lesions [bovine digital derma- | Bovine spongiform encephalopathy |
| titis, sole ulcers, white line disease, etc.], pedal osteomyelitis) | Sporadic bovine encephalomyelitis |
| Lice or ked infestation | Omental bursitis (B) |
| Sarcoptic mange | Bronchobiliary fistula (B) |
| Wound myiasis | Pulmonary listeriosis |
| Copper deficiency | Endocardial fibroelastosis (B) |
| Selenium deficiency | Cholelithiasis |
| Bluetongue (O) | Neoplasia (other than bovine leukemia virus) Ulcerative posthitis, vulvitis (B) |
| Less Common Causes | Local and systemic mycoses |
| Coenurosis (gid) | Fungal granuloma |
| Sarcocystis | Systemic candidiasis |
| Mandible, maxilla fracture | Mycoplasma, arthritis |
| Loss of teeth, periodontal disease | Polycythemia (B) |
Continued
| ■ BOX 9.7 | |
| Causes of Weight Loss in Ruminants—cont'd | |
| Idiopathic granulocytopenia or thrombocytopenia | Fescue (B) |
| Hypersensitivity to soy or milk replacer | Fireweed (Kochia scoparia) |
| Phosphorus deficiency | Geigeria spp. (exotic) |
| Vitamin A deficiency | Gossypol (cottonseed) (Gossypium spp.) |
| Zinc deficiency | Grass staggers (Phalaris spp.) Hairy vetch (Vicia villosa) |
| Toxins | Leucaena leucocephala (exotic) |
| 4-Aminopyridine | Locoweed (Oxytropis, Astragalus) |
| Aflatoxicosis | Mushroom (Amanita spp.) |
| Arsenic | Perennial broomweed (Gutierrezia sarothrae) |
| Chlorpyrifos | Pimelea spp. (exotic) |
| Cobalt | Pyrrolizidine alkaloid toxicosis (Senecio spp., Amsinckia spp., |
| Crude oil | Crotolaria spp., and others) |
| Diesel fuel | Sneezeweed (Helenium hoopesii) |
| Ergotism | Tung tree (Aleurites fordii Hemsl.) |
| Ethylene glycol | White snakeroot (Eupatorium rugosum) |
| Fluorosis Furazolidone | Yellow-wood (Terminalia oblongata spp. oblongata) (exotic) |
| Herbicides | Exotic Diseases |
| Kerosine | Malignant catarrhal fever |
| Lead toxicity | Babesiosis (Babesia bigemina, Babesia bovis) |
| Mercury toxicity | Besnoitiosis (Besnoitia besnoiti) |
| Polybrominated biphenyls | Bovine petechial fever (Ehrlichiaondiri) (B) |
| Selenium toxicity | Burkholderia pseudomallei |
| Sodium chloride toxicity | Contagious bovine pleuropneumonia (Mycoplasma mycoides |
| Trichothecene (T-2) | mycoides) (B) |
| Vitamin D3 toxicity | East Coast fever (theileriosis) |
| Zinc toxicity | Echinococcosis |
| Stachybotryotoxicosis (exotic) | Foot-and-mouth disease (Aphtae epizooticae) Ibaraki disease (epizootic hemorrhagic disease) (B) |
| Plant Toxins | Ovine encephalomyelitis (O) |
| Acorn, oak (Quercus spp.) | Schistosomiasis |
| Bermuda grass (prussic acid) | Surra (Trypanosoma evansi) |
| Bracken fern (Pteridium aquilinum) Cocklebur (Xanthium spp.) | Trypanosomiasis (Trypanosoma spp.) |
B, Bovine; O, ovine.
results in weight loss, but PCM and associated weight loss can occur through several other mechanisms. The most direct cause is that the animals receive an inadequate volume of feed to meet their dietary requirements. This can occur as frank underfeeding of all animals or as a consequence of inadequate feeding facilities that create competition among animals for available feed. The latter circumstance occurs most dramatically when animals of varying ages are mixed; the younger animals with the highest requirements are often pushed away by older, dominant individuals.
The quality of the diet, particularly dietary forages such as hay and pasture, is an important factor in the development of PCM and total nutrient intake. Table 9.1 lists guidelines for estimating the maximum daily intake by cattle. It is evident that as forage quality (digestibility) decreases, maximum daily intake decreases because poor-quality feed must remain in the rumen for an increased period of time before it is sufficiently digested to allow passage through the reticuloomasal orifice. Maximum dry matter intake (DMI) as a percentage of body weight is somewhat higher in small ruminants than in cattle. However, the energy requirement per kilogram of body weight is higher in small ruminants than in cattle. Similar estimates for maximum DMI in horses related to forage quality are not available, yet horses will consume on average 2% of their body weight as DMI, with some studies reporting intakes as high as 4% of body weight. Horses do not have a pregastric fermentation organ (rumen) and can ingest slightly more of the same quality forage than cattle. Low-quality forages are often the
cause of PCM, even when an unlimited quantity is available. The best way to determine the nutrient content of forage, grain, and pelleted feeds is to have the feed analyzed by a forage laboratory. Feed analysis instructions are provided in Box 9.3. Feed tag labels or forage databases can be referenced if an analysis is not performed.
Environmental factors can have a major influence on nutrient requirements and can increase the subsequent risk for PCM and weight loss. The most important environmental factor is the ambient temperature. Nutrient requirements for maintenance change with a decreasing ambient temperature as follows:
• Adult horses: Estimated increase in digestible energy (DE) requirements by 2.5% for every degree Celsius below the lower critical temperature (LCT). The LCT for adult horses ranges from 5° C to -15° C, depending on the horse's adaptation to the environment. In cold temperatures, when the hair coat is wet, the maintenance DE requirement may be increased by as much as 50%.7
• Beef cattle: 1% increase in maintenance energy requirements (total digestible nutrients [TDN], net energy of maintenance [NEm], digestible energy [DE], and metabolizable energy [ME]) for each 1° C drop below 20° C (68° F).
• Dairy cattle (lactating): 25% increase in energy requirements (TDN, net energy of lactation [NEl]) as ambient temperature drops from 20° C (68° F) to -10° C (14° F).
• Sheep with 10-cm wool: 1% increase in energy requirements (TDN, ME, DE) for each 1° C drop below lower critical temperature (approximately -10° C).
There are also additive effects of wind and rain that increase energy requirements in large animal species. As nutrient requirements increase, the dietary intake must also increase to prevent weight loss associated with PCM. Horses in inclement weather may not be able to consume enough forage to meet their increased energy requirements, and for these animals, dietary fat and limited grain supplementation may be required.
Deficiencies of micronutrients (trace minerals, B vitamins) often result in inefficiencies in basic biochemical pathways. These inefficiencies, if marked, can be associated with weight loss. Genetic errors in metabolism can cause similar disturbances, but these usually manifest as decreased growth and even death in young animals.
Parasitism is a common cause of weight loss in adult domestic animals. The mechanisms by which parasite infestation can result in weight loss include a loss of body fluid and tissues resulting in increased nutrient requirements, competition for nutrients in the gastrointestinal tract, malassimilation and malabsorption, inflammation resulting in increased nutrient requirements, micronutrient deficiencies, and organ or vascular damage from migrating parasite larvae. Anorexia may also develop in the advanced stages of severe parasitism.