Approach to the Diagnosis and Management of Weight Loss in Adult Horses
Use the flow sheet in Fig. 9.3 to aid in decision making.
1. Take a general history and a diet history.
a. General history
i. Is the weight loss affecting one animal or many animals? If many horses are affected, what is the age range of the affected animals? How long has the caretaker noticed the weight loss? Has the diet been changed to manage the weight loss? What is the change in BCS of the horse(s)? How much weight has been lost? Is this an estimate of weight loss, or has the horse(s) been monitored on a scale or with a weight tape? Weight loss is often suspected but not documented in the initial complaint or history.
Acute weight loss of 5% to 10% is significant. If a weight tape will not fit around the girth of the horse or if the horse has a BCS of 1 to 3, a rough estimate of body weight can be made using measurements of the length and girth of the horse.17,18 Length is measured from the tuber ischium to the point of the shoulder, and girth is measured at the withers, behind the elbows, at the end of expiration.Chest girth (cm)2 ? Length (cm)
Body weight (kg) =------------------ ---------------------------- -------------
11,877
The weight of miniature horses should be obtained using a small animal clinic scale. If a scale is not available to weigh a miniature horse, then the following equation can be used to estimate the weight of the miniature horse.19
Body weight (kg)
(3.7 ? Chest girth in cm) + (2 ? Length in cm) - 348.5 = 22
ii. Is there any past or current clinical disease in the horse or herd? If so, when was the disease first diagnosed? How many animals were affected? What type of treatment was administered? Was the diet changed during this period of time? Question the caretaker closely about any clinical signs of diarrhea, coughing, dysphagia, or polyuria. What is the deworming history of the horse and herd? Has the deworming protocol been changed lately?
b.
Diet historyi. Type of feed. Obtain an accurate dietary history including the type and amount of feed offered (in pounds, ounces) and the amount of feed refused by the horse(s). It is essential that feeds are weighed accurately. What type and volume of forage is available? Inspect the pasture and all feeds for gross quality, evidence of
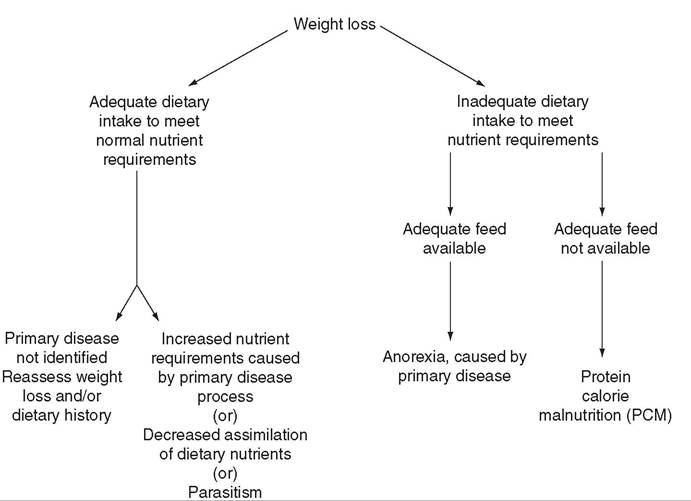
FIG. 9.3 Flow sheet for classifying conditions associated with weight loss.
■ TABLE 9.13
Daily Nutrient Requirements of Ponies and Horses of Mature Body Weight
| Category | Digestible Energy (Mcal) Crude Protein (g) | Calcium (g) | Phosphorus (g) | |
| Mature Ponies, 200 kg (440 lb) of Mature Body Weight | ||||
| Maintenance, average activity | 6.7 | 252 | 8 | 5.6 |
| Mares, last 90 days of gestation | 7.7-8.6 | 319-357 | 14.4 | 10.5 |
| Lactation, first 3 mo | 12.7-12.2 | 614-587 | 23.6-22.4 | 15.3-14.4 |
| Mature Horses, 400 kg (880 lb) of Mature Body Weight | ||||
| Maintenance, average activity | 13.3 | 504 | 16 | 11.2 |
| Mares, last 90 days of gestation | 15.4-17.1 | 637-714 | 28.8 | 21 |
| Lactation, first 3 mo | 25.4-24.5 | 1228-1174 | 47.3-44.7 | 30.6-28.8 |
| Mature Horses, 500 kg (1100 lb) of Mature Body Weight | ||||
| Maintenance, average activity | 16.7 | 630 | 20 | 14 |
| Mares, last 90 days of gestation | 19.2-21.4 | 797-893 | 36 | 26.3 |
| Lactation, first 3 mo | 31.7-30.6 | 1535-1468 | 59.1-55.9 | 38.3-36 |
| Mature Horses, 600 kg (1320 lb) of Mature Body Weight | ||||
| Maintenance, average activity | 20 | 756 | 24 | 16.8 |
| Mares, last 90 days of gestation | 23.1-25.7 | 956-1072 | 43.2 | 31.5 |
| Lactation, first 3 m | 38.1-36.7 | 1842-1761 | 70.9-67.1 | 45.9-43.2 |
| Mature Horses, 900 kg (1980 lb) of Mature Body Weight | ||||
| Maintenance, average activity | 30 | 1134 | 36 | 25.2 |
| Mares, last 90 days of gestation | 34.6-38.5 | 1434-1607 | 64.8 | 47.3 |
| Lactation, first 3 mo | 54.4-52.4 | 2763-2642 | 106.4-100.6 | 68.9-64.9 |
Modified from National Research Council.
Nutrient requirements of horses. Washington, D.C., 2007, National Academies Press.spoilage, abnormal color or odor, presence of weeds and mold, and quantity of feed the owner has at the facility. Has an analysis been performed on the forage (pasture grass and/or hay)? If yes, obtain a copy of the analysis for the patient record. How much time does the horse have to graze in a pasture? What type of grass is available in the pasture? Is the pasture overgrazed? Are there any plant toxins in the pasture or environment? Have there been any changes in the type of forage offered to the horse(s)? Hay quality is often not consistent between shipments. If grain or other supplemental feeds are used, what volume is fed and consumed by the horse(s)? Are any diet supplements fed to the horse? If so, what amount is fed? Does the horse have access to a salt or trace mineral block? How long has this diet been fed? Nutrient requirements of adult ponies and horses are listed in Table 9.13 and can also be calculated using the Nutrient Requirements of Horses free companion computer program (www.nap.edu/catalog/11653/nutrient-requirements -of-horses-sixth-revised-edition).
ii. Feeding management. How often are the horses fed? What type of feeder is used? Are mats placed under the feeders to reduce sand and dirt ingestion? Is there competition among the horses for food? Are there any toxic substances in the horse's environment? What is the water source for the horses? How many water sources are available? Is the water clean?
2. Perform a physical examination.
a. Observe the horse while it is eating. Can the horse prehend, masticate, and swallow food normally? Is the horse dys- phagic? Does the horse have a good appetite? Is the horse hungry? Are there any signs of neurologic disease?
b. Examine the patient closely to identify signs of concurrent disease (e.g., pyrexia, diarrhea, melena, dysphagia, abnormal dentition, icterus, nasal discharge, cough, dyspnea, tachycardia, cardiac murmur, dysuria).
c. What is the horse's body weight (scale or weight tape) and BCS (see Table 9.1)?
3. Examine the feces. What is the consistency of the feces? If the horse has evidence of diarrhea, review the section on diarrhea in Chapter 7. How long are the fibers in the feces? Perform a glove test. Is there evidence of sand in the feces? Horses can have a significant volume of sand in the large intestine while having negative fecal sand test results. Perform a fecal egg count. An enzyme-linked immunosorbent assay (ELISA) may be useful in diagnosing a tapeworm infection. Follow the parasite control program in Chapter 49 if the horse has evidence of fecal parasites or if a parasite infection is suspected despite a negative fecal egg count. Perform a fecal occult blood test; if the result is positive, see the section on melena in Chapter 7.
4. Perform blood analyses.
a. Perform a CBC including plasma protein and fibrinogen. Examine the results closely for indication of an inflammatory process (e.g., leukocytosis, neutrophilia, leukopenia, neutropenia, hyperfibrinogenemia, decreased plasma protein/fibrinogen ratio [below 10]). Calculate the erythrocytic indices, and characterize anemia, if present.
b. Perform a serum biochemical analysis. The serum albumin half-life is approximately 19 days in horses. Hypoalbumin- emia may be associated with colitis, internal abscessation, PCM, liver disease, renal disease, and granulomatous bowel disease, among other conditions. Albumin is often within normal limits in PCM until the patient is near death. Globulin (particularly γ-globulins) may be increased with inflammation, and the albumin/globulin ratio may be decreased. The glucose concentration is usually normal or elevated as a result of stress and may also be elevated in horses with pituitary pars intermedia dysfunction (PPID) and equine metabolic syndrome. Hyperlipidemia (serum triglyceride between 100 and 500 mg/dL) is commonly associated with early anorexia and can be present in horses with PPID.
Hyperlipemia (serum triglyceride above 500 mg/dL) is a serious condition associated with prolonged anorexia and hepatic lipidosis and is often found in miniature horses, ponies, and donkeys under severe physiologic stress (PCM and lactation). Unconjugated bilirubin levels can rise to 6 or 7 mg/dL with anorexia or decreased food intake. An elevated γ-glutamyltransferase (GGT) (above 25 IU/L) may indicate hepatic disease. Horses with PCM may have a low serum urea nitrogen if the protein malnutrition is prolonged and severe.5. Analyze the diet and improve the feeding program.
a. Determine if the energy, protein, mineral, and vitamin content of the diet meets the nutrient requirements of the horse at its current metabolic state and activity level (see Table 9.13). Include pertinent environmental and management factors in the nutrient requirement calculations. The quality of the feeds should be assessed.
i. Forage. Determine the nutrient content of forage or pasture with an analysis (see Boxes 9.3 and 9.4). A university extension service often can assist with a forage analysis. If the client does not purchase a large volume of hay, or if analysis cannot be performed, forage tables from the Nutrient Requirement Council reference books (www.nap.edu) or nutrient tables from the Equi-Analytical Laboratories forage laboratory database (www.equi-analytical.com) can be used to estimate the concentration of different nutrients in common forages and supplemental feeds.
ii. Grain, commercial feeds, and other supplemental feeds. Review the feed tag label to determine the nutrient concentration of protein and other essential nutrients. Contact commercial feed companies for the energy content of their products. Use nutrient databases to estimate the nutrient content of other feeds.
iii. Vitamins, minerals, and other dietary supplements. Review all products used on the horse(s). Ensure adequacy of all essential nutrients. Are there any nutrient toxicities? Are all products necessary? If botanical ingredients are fed, are there any nutrientdrug interactions or contraindications in feeding the botanicals?
b.
If the horse has a dietary deficiency, the problem should be corrected by a change in the diet or through appropriate supplementation. Contact an equine clinical nutritionist for guidance on ration formulation.c. If the dietary history indicates that adequate nutrients for maintenance, or the appropriate life stage, or performance have been steadily consumed, continue to search for another cause of the weight loss.
6. Perform ancillary diagnostic tests. If the weight loss is not caused by inadequate or poor-quality feed, additional diagnostic tests should be performed. Possible tests include but are not limited to ultrasound, gastric endoscopy, radiographs, serum or whole blood trace mineral analysis, serum insulin concentration, carbohydrate absorption tests (oral D-glucose, D-xylose [see Chapter 32]), and appropriate organ biopsy.