Body Cavities and Mesenteries
OPENING THE CAT
Exposure of the body cavities is not difficult if one looks before one leaps! Place the cat ventral side up on the tray. Palpate the sternum to locate the xiphoid process and remember that the sternum in the cat is elongate so do not panic if it appears that you are too far posterior.
Also, note that the xiphoid process is cartilaginous and will feel softer than the sternum. A good muscle dissection should have left you with the xiphihumeralis muscle in the chest area. The xiphoid process occurs approximately 1/4 to 1/2 inch cranial to the posterior edge of this muscle. During the following procedure, refer to Figure 3-1.All of the following instructions apply to the skinned side of the cat. Make a one inch horizontal incision through all muscle layers and connective tissue about 1/4 inch posterior to the tip of the xiphoid process with your scalpel (Incision 1). Take care to only cut through the muscles and not damage underlying organs. Insert your finger into the incision to determine whether you have penetrated the body cavity and to locate the diaphragm. There is a high probability that you have made your incision just posterior to the diaphragm. The diaphragm is a muscular partition separating the thoracic and abdominal cavities that feels similar to a taut balloon.
With scissors, extend the incision laterally on both sides toward the back of the cat along the curved contour of the diaphragm about 3-4 inches on each side (Incision 2). With a scalpel, very carefully loosen the diaphragm from the body wall allowing it to come to rest on the liver. From the original horizontal incision, make a caudally directed longitudinal incision one-half inch to one side of the midline. While you are making
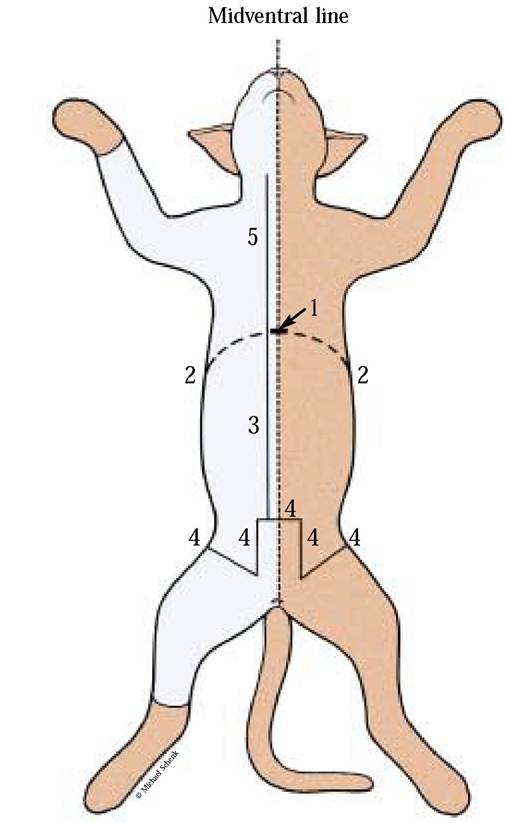
FIGURE 3-1 Incisions to expose internal organ systems.
this incision pull the abdominal wall up and watch for a midventral mesentery attaching the urinary bladder to the wall (Incision 3).
When within about 1/2 inch of this mesentery, stop. Laterally, cut about one inch to either side of the midline and then continue these cuts to the caudal end of the abdominal cavity to form a small door-like structure (Incision 4). If your specimen is a male, be careful not to destroy the spermatic cord, the inguinal canal or vas deferens. The cord can be recognized because it contains not only the vas deferens but also injected blood vessels lying on the medial aspect of the leg and passing over the brim of the pelvis continuing through the inguinal canal and through the abdominal muscles. Extend the incisions laterally from the caudal cuts (above), again avoiding the inguinal canal and spermatic cords.To expose the organs of the thoracic cavity, with scissors cut from the xiphoid process cranially (toward the head). Your incision should be 1/2 inch from the midventral line of the skinned side of the specimen (Incision 5). As you approach the neck region you will be cutting through muscles in which major blood vessels and nerves occur (arteries— red, veins—blue, nerves—white). To avoid destroying these structures, we recommend that you cut through one muscle at a time. Firmly grasp the thoracic wall of the skinned side and reflect back until you hear a cracking sound. Gently lift the opposite side with the intact skin and observe the mesentery adhering to the midventral body wall. Carefully, with your scalpel release the mesentery from the body wall allowing it to fall on the surface of the underlying organs. Just lateral to the attachment of this mesentery, on either side, observe an artery and vein adhering to the inner surface of the ventral thoracic wall. Again, with your scalpel, release these vessels from this surface. If necessary, remove some of the muscle. Now, with both hands grasp the rib cage on the unskinned side and quickly reflect back the thoracic wall until you hear a cracking sound.
Until you have read the next sections, do not remove or disturb any tissues that might appear fatty or membranous, particularly, the greater omentum [Figure 3-2].
To preserve these delicate membranes, it is highly recommended that the mesenteries be studied before consideration of the viscera.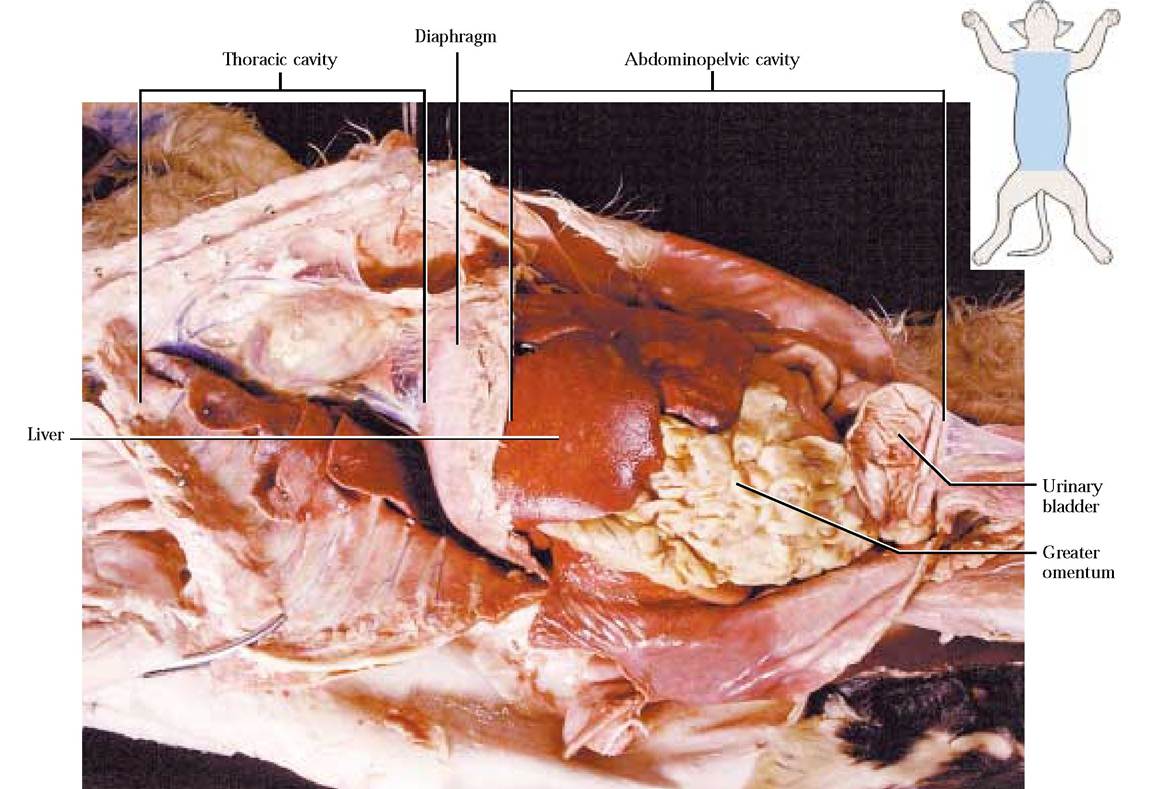
BODY CAVITIES
OR COELOMIC CAVITIES
Among both invertebrates and vertebrates we see bodies that have evolved with body cavities lined with mesenteries allowing organs that are suspended within them to move independently of the general body surface. In general, this has allowed animals to develop a number of important characteristics and to become larger and more mobile.
Vertebrate body cavities are typically lined with a shiny membrane called a serosa. The serosa lining the body wall is known as the parietal layer and the outer covering reflected over the surface of most organs suspended in these cavities is a continuation of this membrane called the visceral serosa. In reality, what we refer to as a cavity in the living animal is a potential space containing a small amount of lubricating fluid, allowing free sliding movement of the organs. Mesenteries are membranes suspending organs within the cavities and extending between the parietal and visceral layers.
To illustrate the relationship of the parietal and visceral membranes associated with cavities, imagine a ball with a fist thrust into it. The fist represents any organ projecting into the cavity. The layer of the ball surrounding the fist is analogous with the visceral membrane and the outer ball surface is analogous with the parietal membrane. The space between the two ball surfaces is analogous with a body or coelomic cavity [Figure 3-3A].
In mammals, including the cat or human, the coelomic cavity is divided into a thoracic and abdominopelvic (peritoneal) cavity by the unique muscular diaphragm [Figure
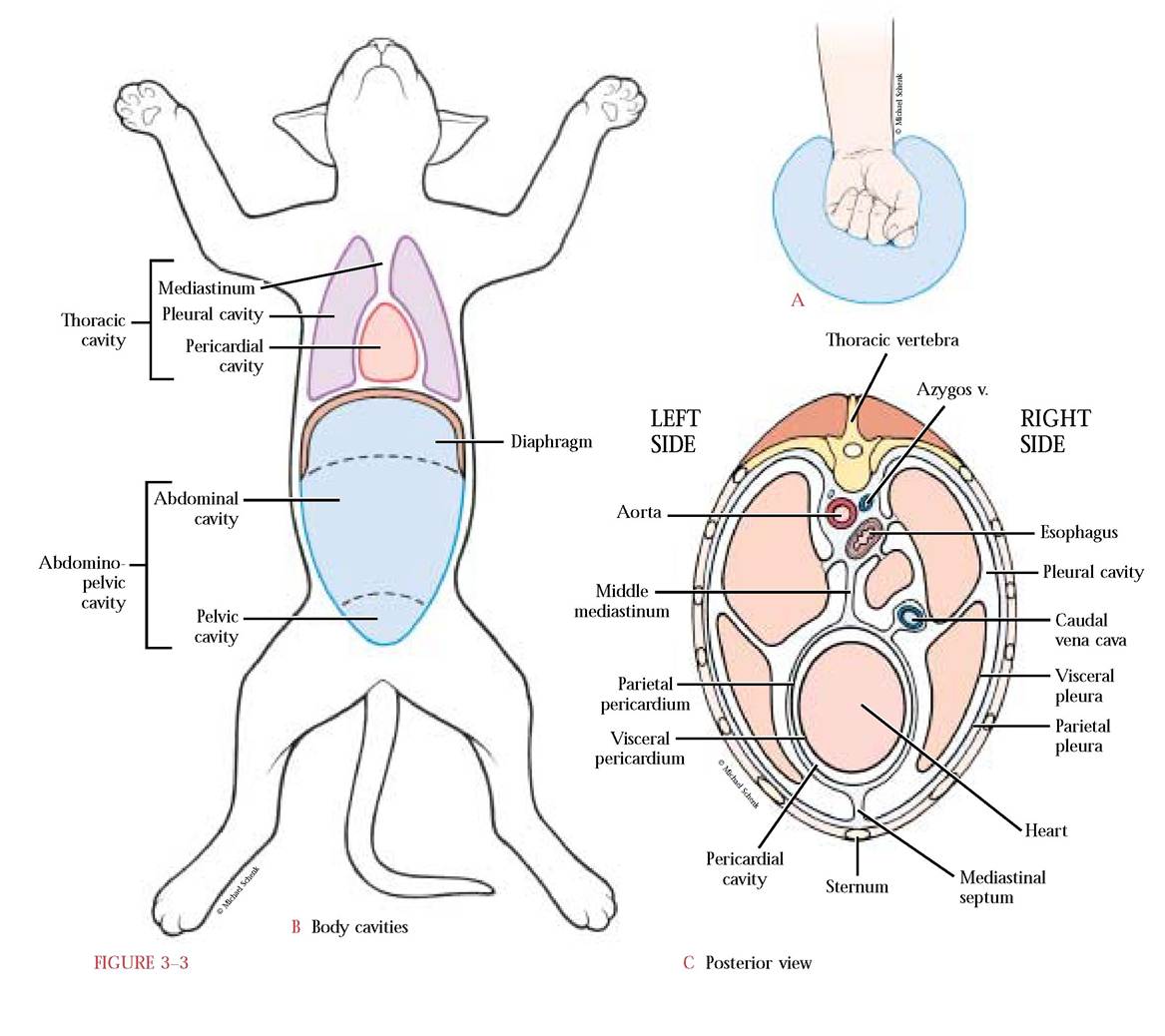
3-3B]. The thoracic cavity is further subdivided into a more or less central pericardial cavity surrounding the heart and paired lateral pleural cavities containing the lungs.
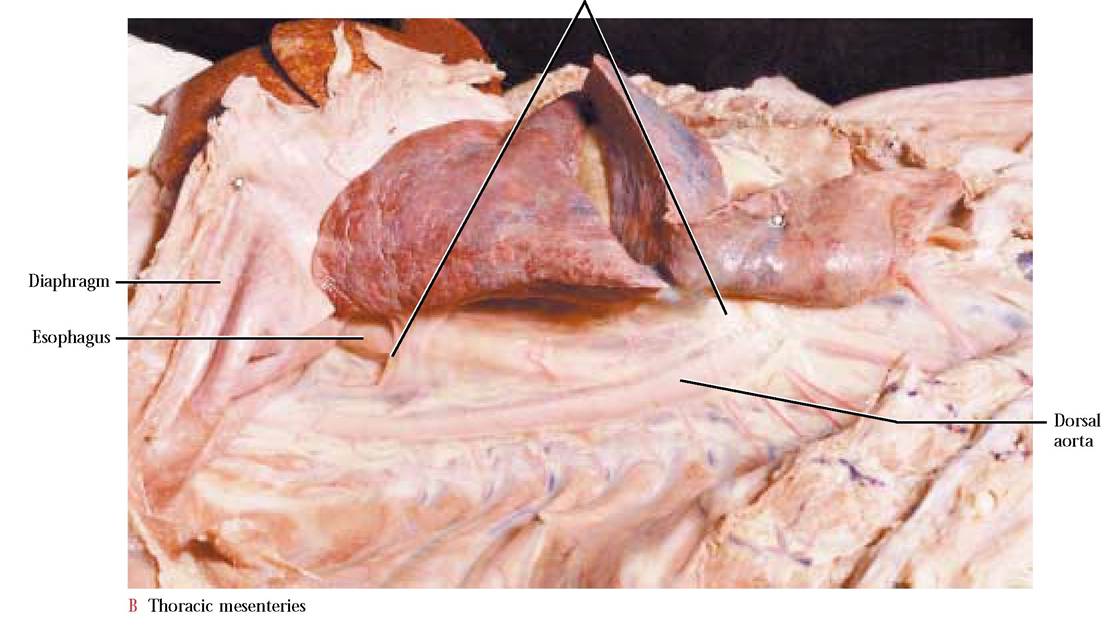
Between the two pleural cavities is a potential space, the mediastinum, in which is located the heart and its cavity, the esophagus, the trachea, major blood vessels, nerves, and some endocrine organs all of which are held in place by loose connective tissue [Figure 3-3C].The abdominopelvic cavity is arbitrarily divided by an imaginary line drawn from the ilial crest to the pubic rim, defining an abdominal space and a pelvic space. In the abdominal cavity are suspended primarily digestive organs while in the pelvic cavity are urinogenital organs and the distal organs of the digestive tract [Figure 3-3B].
MESENTERIES OF THE THORACIC CAVITIES
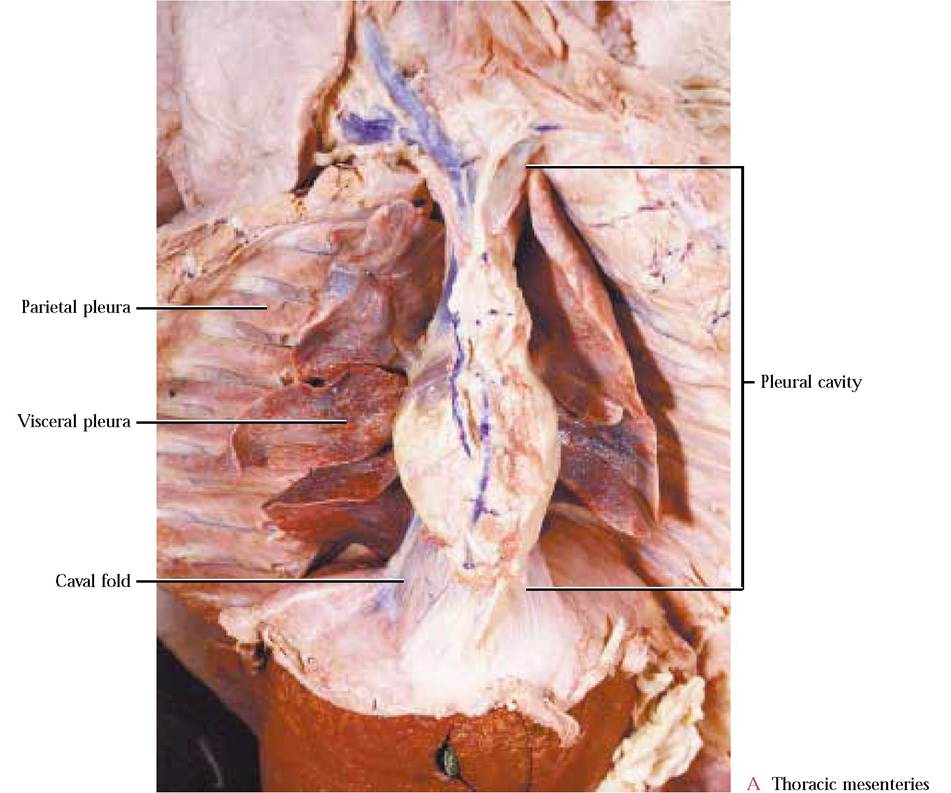
The pleural cavities are delimited by the parietal pleura as a glistening membrane that continues as the reflected visceral pleura, the outer covering of the lungs. The joined left and right medial parietal pleurae form the mediastinal septum. It is located both ventral and dorsal to the pericardium and continues anterior to the heart and adheres to the organs residing in the mediastinum. Take note that the ventral portion of the mediastinal septum is that membrane that you loosened from the mid-ventral thoracic body wall when you “opened the cat. ” The right postero-ventral portion of the mediastinal septum forms a pocket, the caval fold, into which projects the small accessory lobe of the right lung. Notice that a large blue blood vessel, the posterior vena cava, adheres to the medial portion of this mesentery. With your fingers, very carefully pull one of the lungs laterally and observe the stretched mesentery, the pulmonary ligament [Figure 3-4B].
The serosal membranes associated with the heart are similar in their relationships to those of the pleural membranes and their association to the lungs. With a pair of scissors make a slit in the ventral portion of the pericardial sac to appreciate the pericardial cavity. The parietal
Pulmonary ligament
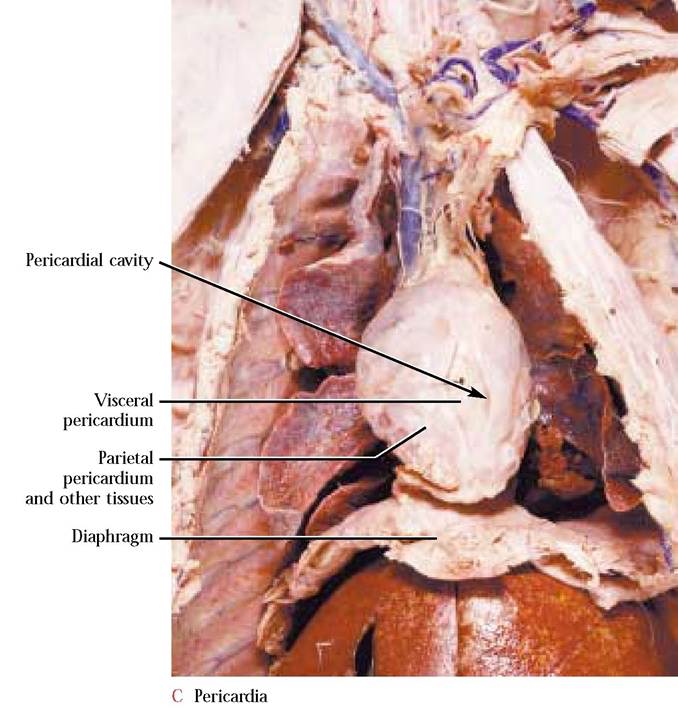
pericardium defines the potential space called the pericardial cavity and then reflects over the surface of the heart as the visceral pericardium [Figure 3-4C]. In contrast to the pleura, the parietal pericardium is intimately associated externally with other tissues forming the pericardial sac.
MESENTERIES OF THE Abdominopelvic cavity
Carefully separate the diaphragm from the liver and identify the whitish area, the central tendon of the diaphragm, where the muscles of the diaphragm converge. This is also the site of contact between the liver and the diaphragm. Three ligaments can be identified between the diaphragm and the liver. The most prominent of these is the falciform ligament found between the left and right halves of the liver and extending to the ventral abdominal wall. The thickened free margin of this membrane is the round ligament, a remnant of a fetal blood vessel. The continuation of the falciform ligament
on either side of the central tendon of the diaphragm is the coronary ligament [Figure 3-5].
The very conspicuous and fragile greater omentum must be handled with caution [Figure 3-6]. It lies over most of the visceral organs, holding them in place, and is liberally laced with fat, since it is the site of fat storage. Quite often, the greater omentum is tucked among the coils of the small intestine and may even be attached by strands of serosa to the dorsal parietal peritoneum. Carefully loosen the omentum with your fingers from the intestinal loops, clipping, if necessary, the strands anchoring it dorsally.
The greater omentum is a double layered, apron-like mesentery extending from the greater curvature of the stomach and attaching to the dorsal wall of the peritoneal cavity. The ventral layer of this two-layered mesentery, attached to the greater curvature of the stomach and extending to the pelvic region, turns back on itself toward the stomach as the dorsal layer [Figure 3-7]. It then passes dorsal to the stomach, incorporating the tail of the pancreas and ultimately attaches to the dorsal peritoneal wall. That portion of the ventral layer of the greater omentum, extending from the stomach to the spleen is called the gastrosplenic ligament [Figure 3-6].
The potential space between the dorsal and ventral layers is the omental bursa.
To demonstrate this cavity, carefully separate the two layers and with your scissors cut along the bottom of the apron. Slowly pull the two layers apart and observe the “sac-like cavity. ” The opening of this sac, the epiploic foramen, opens dorsally into the peritoneal cavity, thereby establishing continuity between the omental bursa and the peritoneal cavity. As you are holding the two layers of the omentum, have your partner shine a pen light between the layers, while peering craniad to observe this opening [Figure 3-7]. The foramen opens dorsally and just to the right of the lesser omentum, discussed below.A much less extensive mesentery extending from the liver to the lesser curvature of the stomach and the duodenum is the lesser omentum. That portion of this mesentery between the liver and the stomach is known as the gastrohepatic ligament and the continuation of this mesentery between the liver and the duodenum is the hepatoduodenal ligament [Figure 3-6]. Part of the caudate lobe of the liver projects ventrally into this mesentery. Blood vessels, “bile ducts,” nerves and lymphatic vessels pass on the right through the free surface of this mesentery.
A short, somewhat inconspicuous mesentery, the hepatorenal ligament, stretches from the caudate lobe of the liver to the parietal peritoneum covering the right kidney [Figure 3-8]. Do not destroy this ligament, since there is no corresponding ligament on the left side.
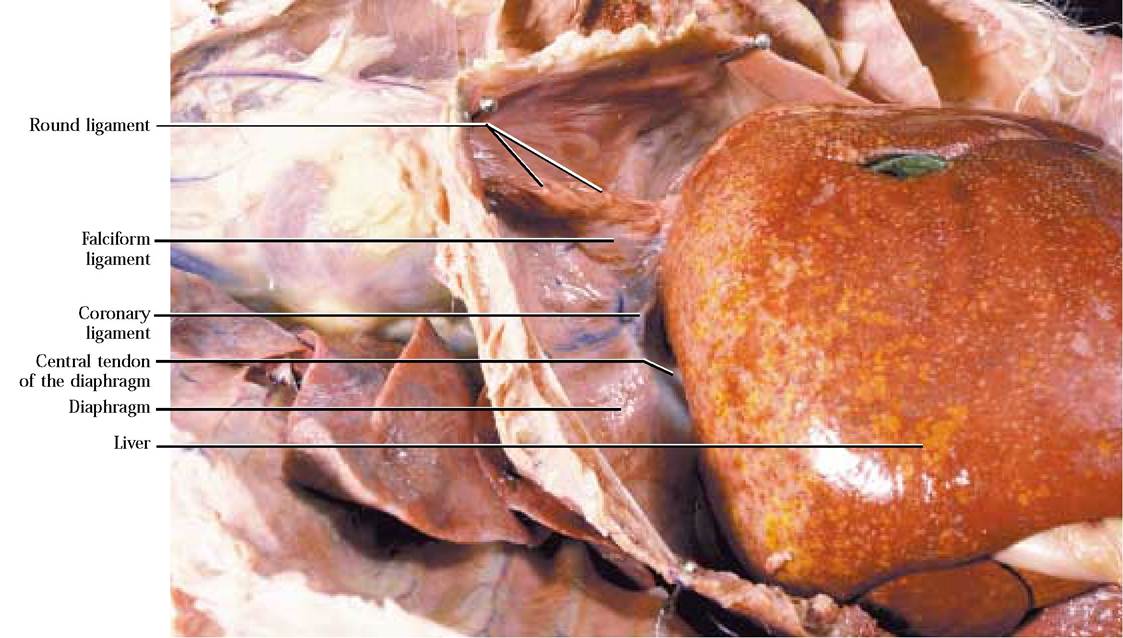
FIGURE 3-5 Ligaments associated with the liver and diaphragm.
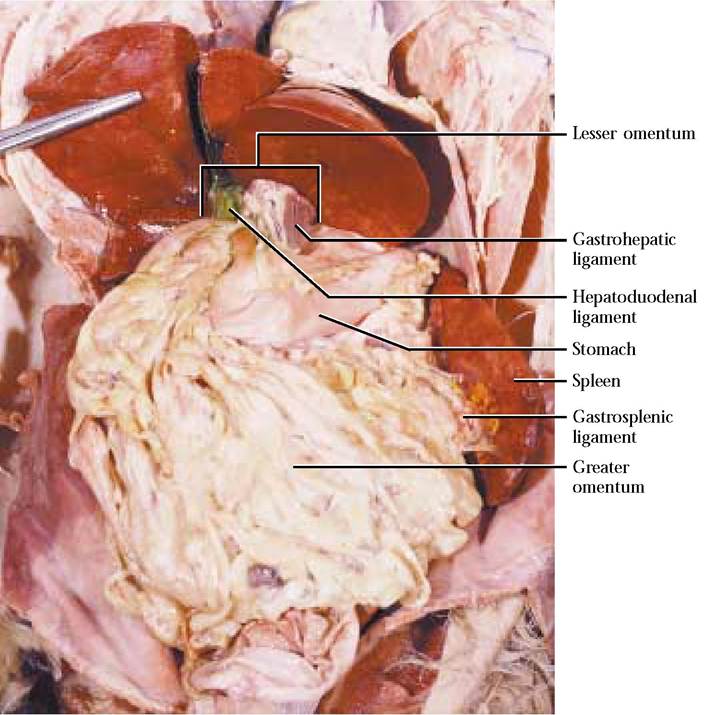
FIGURE 3-6 Greater and lesser omentum.
Also on the right side is an oftentimes more conspicuous and fragile, triangular mesentery, the duodenocolic fold, extending from the duodenum to the mesocolon [Figure 3-9]. On the left side of the peritoneal cavity and extending from the dorsal layer of the greater omentum to the opposite side of the mesocolon is another triangular gastrocolic ligament [Figure 3-9].
From the dorsal body wall, the large intestine (colon) is suspended by a part of the dorsal mesentery, the mesocolon [Figure 3-9]. To appreciate its extent, gently pull the colon ventrally. At the same time, observe that the duodenocolic fold and gastrocolic ligament merge with the mesocolon at opposing acute angles.
Gently lift the coils of the small intestine and observe the extensive mesentery suspending and supporting this organ. Notice the wealth of blood vessels coursing through this mesentery. That portion of this mesentery that supports the duodenum and the head of the pancreas is called the mesoduodenum, while the remainder that
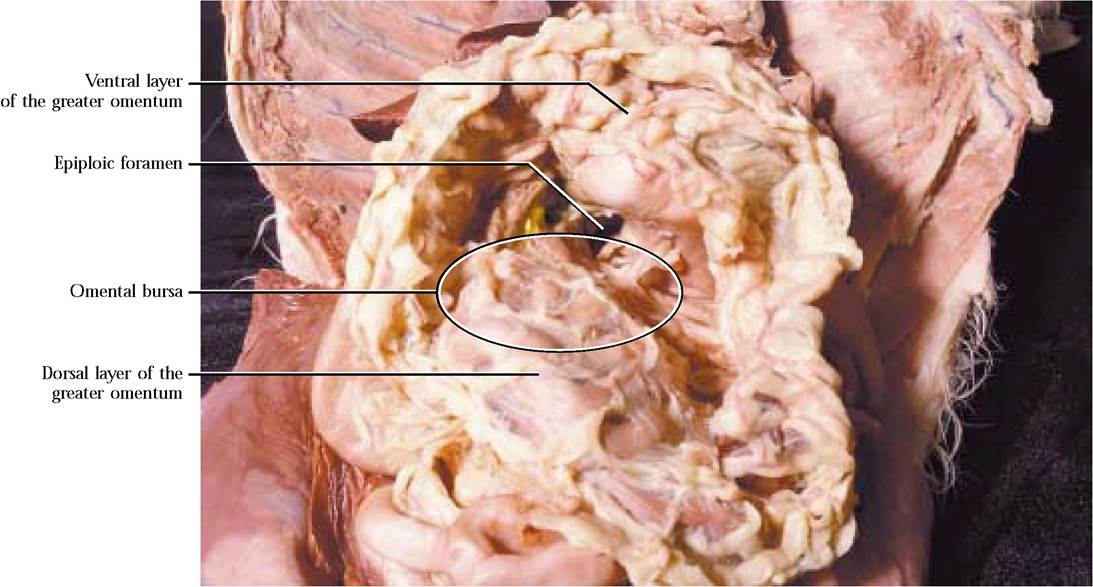
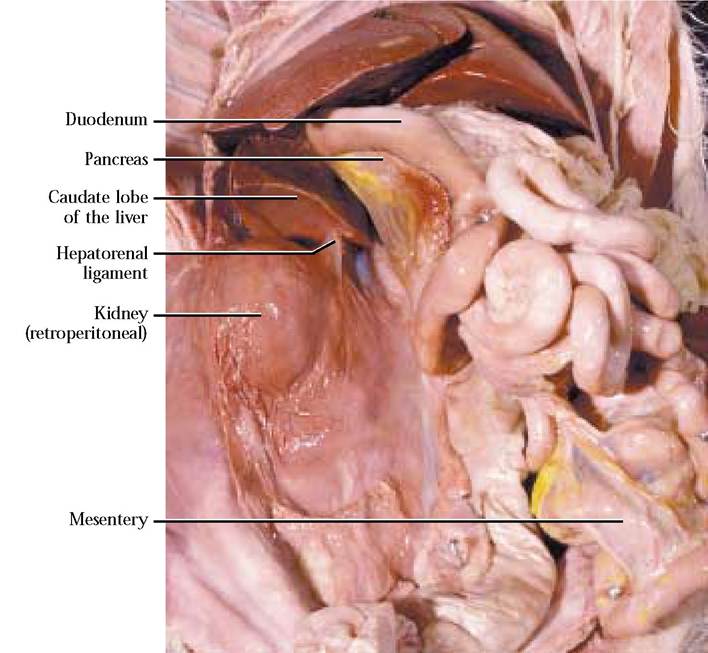
FIGURE 3-8 Hepatorenal ligament.
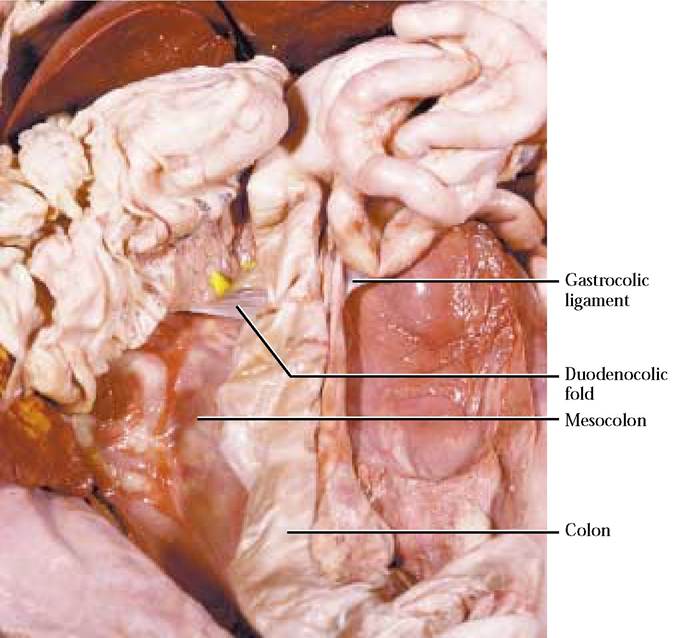
FIGURE 3-9 Mesenteries of the abdominopelvic cavity I.
supports the jejunum and ileum is the mesentery proper [Figure 3-10].
Three prominent mesenteries anchor the urinary bladder in the abdominopelvic cavity. The median vesical ligament extends from the ventral surface of the urinary bladder to the ventral body wall. Both sides of the urinary bladder are anchored to the lateral body wall by the lateral vesical ligaments. Along the free edge of the lateral ligaments runs the round ligament that is the remnant of the fetal umbilical arteries that carried oxygen poor blood to the placenta [Figure 3-11]. There is a generous rounded pad of fat attached to each of the lateral vesical ligaments that may often mask them.
If your specimen is a female, an elongated broad ligament supports the internal reproductive structures. The most extensive part of the broad ligament is the mesometrium supporting the uterus. The portion of the broad ligament, much less extensive, and supporting the ovary is the mesovarium and the least extensive, supporting the uterine tubes (oviducts) is the mesosalpinx. The cranial end of the ovary is attached to the body wall by a thickened suspensory ovarian ligament. The caudal end of the ovary is held in place by a second thickened band called the ovarian ligament, extending between the ovary and the cranial end of the uterine horns. Almost perpendicular and lateral to the mesometrium is the round ligament [Figure 3-12]. It is the female counterpart of the gubernaculum in the male, that will be discussed in the reproductive system.
If your specimen is a male, mesenteries associated with the reproductive system are largely outside the main body cavities and will be discussed with the reproductive system.
Extensions of the abdominopelvic cavity into the pelvic region occur in both sexes. In the male, that part of the cavity that extends between the large intestine and the urinary bladder is the rectogenital pouch and the cavity that extends between the urinary bladder and the ventral body wall is the pubovesical pouch [Figure 3-11].
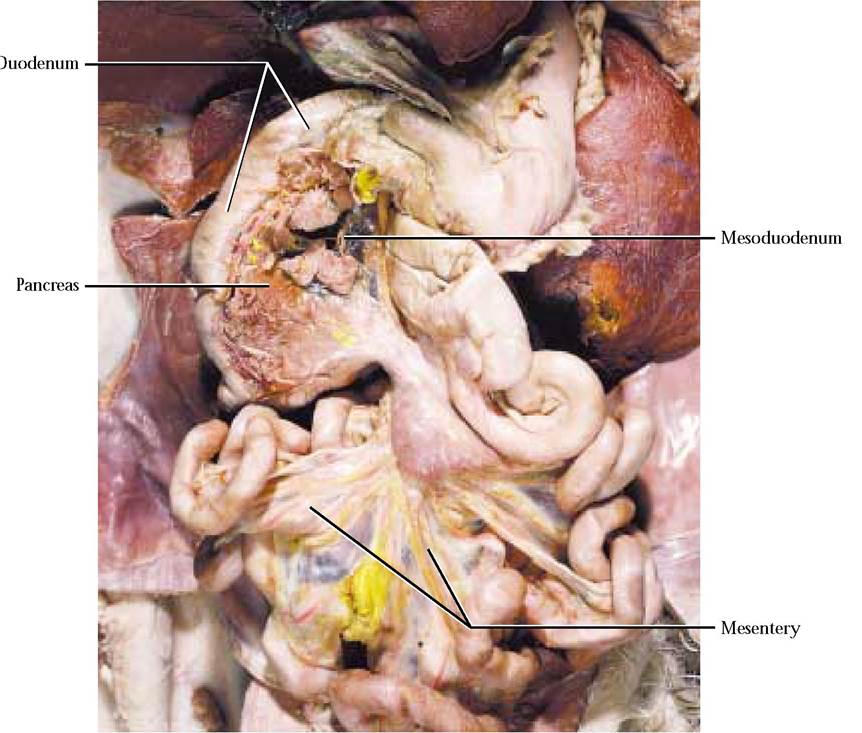
FIGURE 3-10 Mesenteries of the abdominopelvic cavity II.
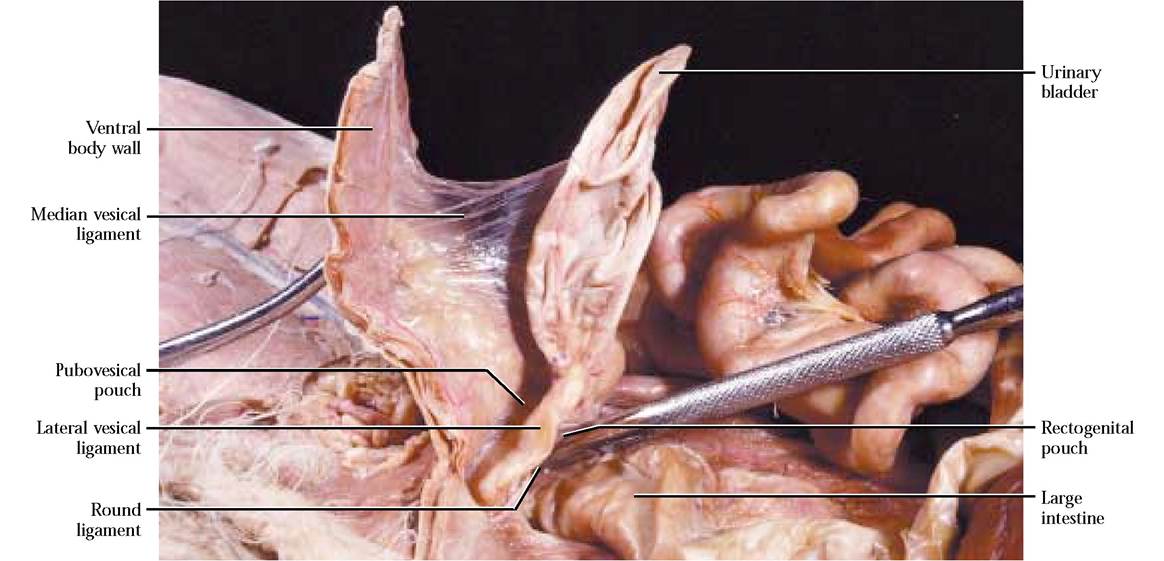
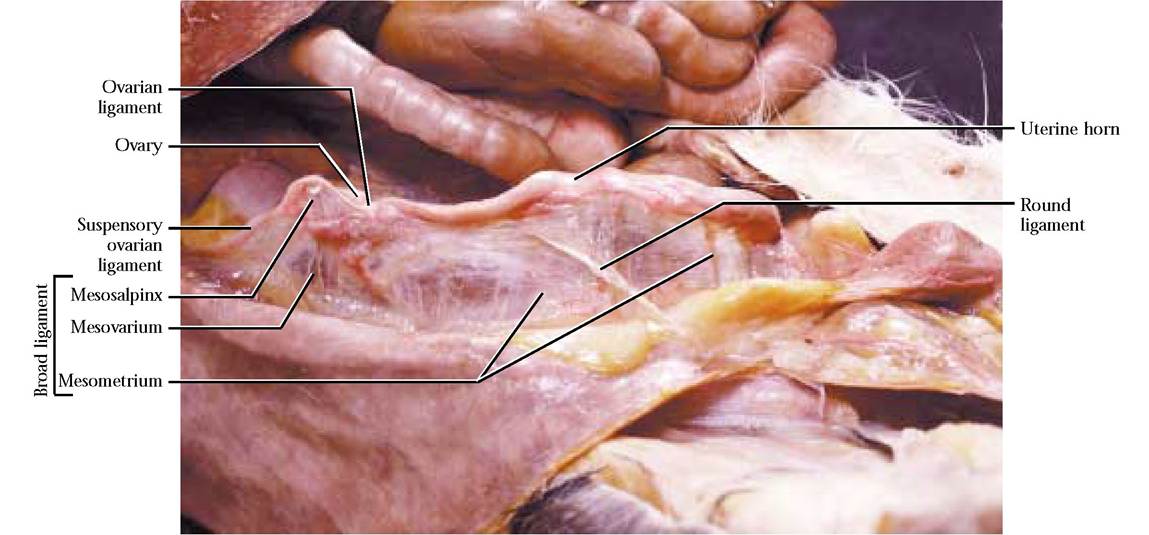
FIGURE 3-12 Mesenteries of the female reproductive system.
In contrast, in females, since the uterus passes between the large intestine and the urinary bladder, there are three spaces versus the two in males. The rectogenital pouch occurs between the large intestine and the uterus, the vesicouterine pouch lies between the uterus and the urinary bladder and the pubovesical pouch is in the same position as in the male, between the urinary bladder and the ventral body wall [Figure 3-13].
Mesenteries and cavities in humans are very similar. A very obvious outward sign of one of the functions of the greater omentum (fat accumulation) in humans is known as a “beer belly. ”
id="Picutre 106" class="lazyload" data-src="/files/uch_group31/uch_pgroup304/uch_uch7238/image/image106.jpg">
FIGURE 3-13 Female abdominopelvic region. The three pins in this figure mark the position of the pelvic pouches.