COUNTERCURRENT MECHANISM
1. What is the function of the countercurrent mechanism?
2. Differentiate between the countercurrent multiplier and countercurrent exchange systems.
3. What is the tone of tubular fluid as it enters the distal tubule?
4.
What functions are served by the recirculation of urea?Preparation of the tubular fluid (after it leaves the proximal tubule) for the conservation or elimination of water depends on the existence of a very high osmolality in the ISF of the renal medulla. The osmolality increases with distance from the cortex, reaching a maximum in the innermost aspects of the medulla. The maximum value varies by species. In the dog, it is about 2,400 mOsm/kg H2O, compared with plasma osmolality of about 300 mOsm/kg H2O. The high osmolality exists because of the countercurrent mechanism. It is established by the activities of the loops of Henle and is maintained by the special characteristics of the blood supply to the medulla (the vasa recta).
A countercurrent system of tubules or vessels exists where the inflow of fluid runs parallel to, counter (opposite) to, and close to the outflow for some distance. These characteristics are common to the anatomic arrangements of the loops of Henle and the vasa recta. Accordingly, the countercurrent mechanism in the kidney comprises two countercurrent systems: the countercurrent multiplier (loops of Henle) and the countercurrent exchanger (vasa recta).
Countercurrent Multiplier System
The countercurrent multiplier is represented in Figure 11-17 by: (1) the descending limb, (2) the thin segment of the ascending limb, and (3) the thick segment of the ascending limb of the loop of Henle. Osmolality changes of the tubular fluid occur as it progresses through the loop of Henle because of the permeability characteristics of the loop of Henle limbs and segments coupled with an active cotransport of NaCl in the thick segment of the ascending limb.
In the descending limb (impermeable to solutes, permeable to water), water diffuses by osmosis to the higher osmotic pressure of the ISF, and solute concentration (mostly NaCl) increases while approaching the hairpin turn of the loop of Henle. The thin segment of the ascending limb is permeable for NaCl and impermeable for H2O. Therefore, water remains in the tubule and NaCl diffuses (because of concentration gradient) to the ISF. In the thick segment of the ascending limb, NaCl is actively transported (cotransport) to the ISF and water continues to be retained. Whereas the osmolality of the tubular fluid entering the descending limb was 300 mOsm/kg H2O, the tubular fluid leaving the ascending limb and entering the distal tubule has been diluted (osmolality 185 mOsm/kg H2O). Tubular fluid osmolality changes (described in upcoming sections) that determine whether the urine is dilute or concentrated occur in the distal tubule and collecting ducts.
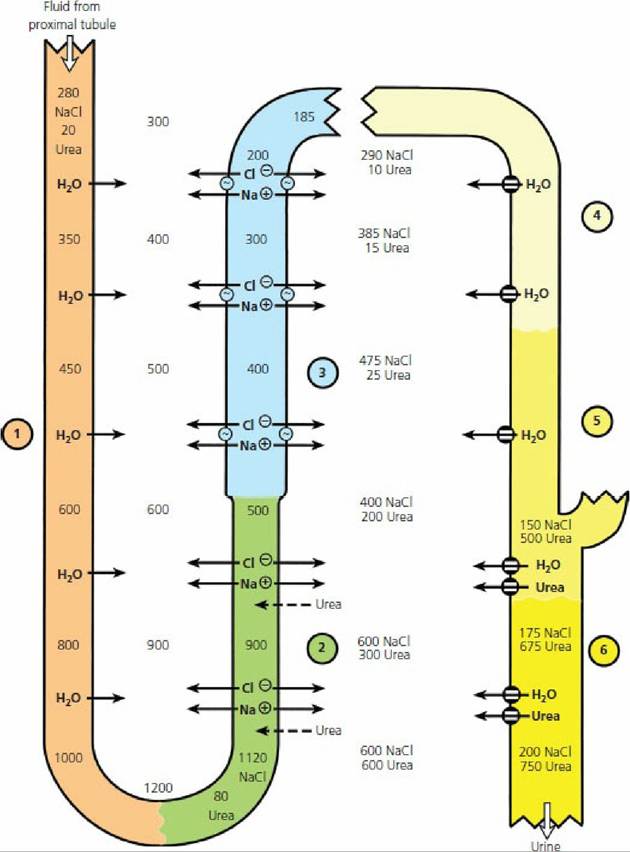
■ FIGURE 11-17 Countercurrent multiplication in the loop of Henle and recirculation of urea. Values shown (in milliosmoles per kilogram H2O) are hypothetical but approximate those of humans under conditions of low water intake. Single numbers represent total osmolality. Identified numbers (NaCl, urea) represent a specific contribution to total osmolality. Transport of NaCl and urea at the level of the thin segment of the ascending limb of the loop of Henle is by simple diffusion. Active transport of Na+ in the ascending thick limb is coupled with the transport of Cl- (cotransport). Water channels (also urea) on the right are open (influence of antidiuretic hormone). In this example, urine is being concentrated. Circled numbers identify locations as follows: (1) descending limb of the loop of Henle; (2) thin segment of ascending limb of loop of Henle; (3) thick segment of ascending limb of the loop of Henle; (4) cortical collecting duct; (5) outer medullary collecting duct; (6) inner medullary collecting duct.
See text for details. (From Reece WO. Kidney function in mammals. In: Reece WO, ed. Dukes’ Physiology of Domestic Animals. 13th edn. Ames, IA: Wiley-Blackwell, 2015.)The vertical osmotic gradient in the ISF (lower in outer medulla, higher in the inner medulla and at a hairpin turn) is established and maintained by: (1) continued active transport of NaCl by the thick segment,of the ascending limb, (2) concentration of tubular fluid in the descending limb, and (3) passive diffusion of NaCl from the lumen of the thin segment of the ascending limb into the inner medullary ISF.
Countercurrent Exchanger System
A countercurrent exchanger is a countercurrent system in which transport between outflow and inflow is entirely passive. The vasa recta act as countercurrent exchangers (Figure 11-18). They are permeable to water and solutes throughout their length. In the descending limbs, water is drawn by osmosis from the plasma of the vasa recta to the hyperosmotic ISF (created by the countercurrent multiplier) and the solutes diffuse from the ISF into the vasa recta. In the ascending limbs, solutes diffuse back into the ISF and water is drawn by osmosis back into the vasa recta. The net result is that the solutes responsible for the vertical medullary gradient are mostly retained in the ISF of the medulla. The vasa recta carry away slightly more solutes than are brought into them.
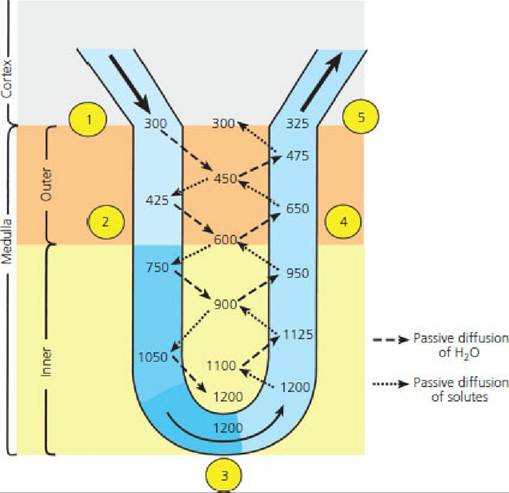
■ FIGURE 11-18 Countercurrent exchange in vasa recta. Values shown (milliosmoles per kilogram H2O) approximate those of humans. Blood enters from the cortex near circled number 1 with a milliosmolality of about 300 and descends through an increasingly hypertonic peritubular fluid in the medulla (circled number 2). Water diffuses out and solute diffuses in until the hairpin turn is reached (circled number 3). The blood then ascends through decreasing hypertonicity, and water diffuses in and solute diffuses out (circled number 4).
When blood returns to the cortex (circled number 5), the milliosmolality is only slightly higher than when it entered the vasa recta. (From Reece WO. Kidney function in mammals. In: Reece WO, ed. Dukes’ Physiology of Domestic Animals. 13th edn. Ames, IA: Wiley-Blackwell, 2015.)An increased rate of medullary blood flow would reduce the time for diffusion of solute from the ascending limb back to the ISF, and the blood leaving the ascending limb would have higher concentration of solute. The result would be a gradual loss or washout of the medullary gradient, referred to as medullary washout. Medullary loss of solute is normally prevented because the blood flow to the vasa recta is reduced (vasa recta comprise 10% to 20% of kidney blood flow) and it is often characterized as sluggish. All of the excess salt removed from the medullary ISF by the vasa recta must be replaced by the loops of Henle for the osmotic gradient to be maintained. If countercurrent blood flow in the vasa recta did not exist and blood from the descending limbs of the vasa recta returned directly to the renal vein instead of counterflowing into the ascending limb, the solute of the renal medulla would be quickly removed instead of being retained.
Role of Urea
In addition to NaCl, urea also contributes to the high solute concentration in the ISF of the kidney medulla. Urea presence is accomplished by a recirculation mechanism for urea between the collecting ducts and the loop of Henle (see Figure 11-17). Recirculation means that urea diffuses from the inner medullary collecting ducts into the ISF, and from there diffuses into the lumen of the thin segment of the ascending limbs of the loops of Henle. Diffusion occurs because of the permeability of these nephron parts for urea and because of concentration differences (high to low concentration). After the entrance of urea into the loops of Henle, it is retained there because of membrane impermeability until it again arrives at the inner medullary collecting ducts, which have a variable permeability depending on the amount of antidiuretic hormone (ADH) (see following section). The recirculation mechanism and high concentration of urea in the medulla not only assist the countercurrent multiplier system and osmotic gradient but also ensure excretion of urea when urine output is low. For example, if urine is formed at the rate of.2 mL/min and it has a urea concentration of 2 mg/mL, then 4 mg of urea would be excreted each minute. If, however, urine formation is reduced to 1 mL/min (greater reabsorption of water), the concentration of urea is increased to 4 mg/mL and excretion is maintained at 4 mg/min. The concentration of urea remains high in the collecting ducts because the concentration is also high in the ISF (diffusion from the collecting duct limited by concentration difference).
■