Countercurrent Exchange in the Vasa Recta Removes Water from the Medullary Interstitium Without Reducing Medullary Interstitial Hypertonicity
The diffusion of water from the descending thin limb into the interstitium would dilute the effect of salt and urea transport into the interstitium and cause swelling of the inner medulla if it were not for the ability of the vasa recta to remove the reabsorbed fluid from the medullary interstitium.
The walls of the vasa recta are permeable to water, salts, and urea. The relatively high plasma oncotic pressure in the vasa recta entering the medulla favors the movement of water into the capillary lumen, and NaCl and urea equilibrate with the interstitial concentration. Thus, as the vessels descend in the inner medulla, the plasma osmolality and urea concentration rise as the vasa recta near the hairpin turn, then fall as it ascends out of the medulla (Figure 43-4).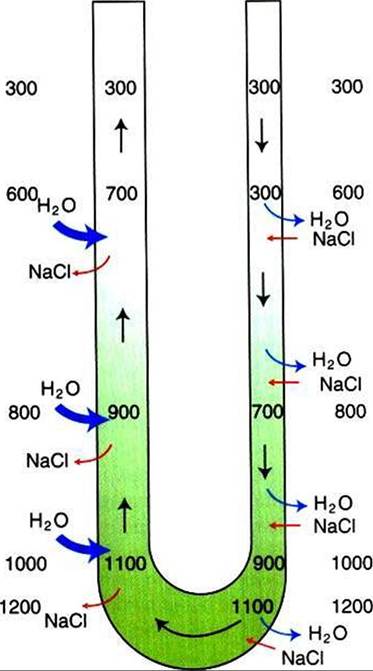
FIGURE 43-4 Countercurrent exchange in the vasa recta. The walls of the vasa recta are permeable to both water and salt (NaCI). Plasma entering the medulla in the descending vasa recta has an osmolality of approximately 300 mθsm∕kg H2O1 which increases as plasma traverses deeper regions of the medulla, where the interstitial osmolality is elevated. Similarly, after the hairpin turn, the plasma osmolality progressively decreases as the vessel ascends into regions of lower interstitial osmolality. In both arms of the vasa recta, the gradient between the plasma and interstitial osmolality is reduced by movement of water and solute in opposite directions. This system prevents the dissipation of the medullary concentration gradient. In addition, there is net removal of water from the interstitium because of the relatively low hydrostatic pressure and relatively high oncotic pressure in the vasa recta.
What is the net effect of passive equilibration of the interstitial fluid with the plasma in the vasa recta? Two observations indicate that by the time the ascending vasa recta leave the medulla, there has been net movement of fluid into the capillary: (I) the plasma oncotic pressure has fallen, and (2) the blood flow in the ascending vasa recta is approximately double that in the descending vasa recta. Thus the countercurrent arrangement of the vasa recta, the passive equilibration of the plasma with the changing interstitial osmolalities in different regions of the medulla, and the relatively high initial plasma oncotic pressure allow the removal of both water and solute from the medullary interstitium, without dissipating the medullary hypertonicity.