TUBULAR REABSORPTION AND SECRETION
1. What nephron part accounts for the greatest amount of reabsorption?
2. What is meant by transport maximum and how does it differ from renal threshold?
For reabsorption to occur, a substance must pass from the tubular lumen through the tubular epithelial cells, diffuse through the interstitial fluid (ISF), and enter the capillary.
A substance to be secreted must leave the capillary, diffuse through the ISF, and pass through the tubular epithelial cell into the tubular lumen. A sagittal section of tubular epithelium and its relationship to the tubular lumen and peritubular capillary are shown in Figure 11-15.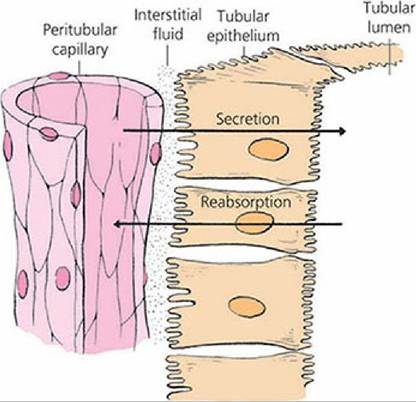
■ FIGURE 11-15 Structures that separate tubular fluid in the tubular lumen from plasma in peritubular capillaries. The energy requirement for reabsorption and secretion processes is provided by the Na+-K+-ATPase (“sodium pump”) located in the basolateral membrane of proximal tubule epithelial cells.
Reabsorption of Na+, Cl, Glucose, and Amino Acids
Substances important to body function, such as glucose and amino acids, enter tubular fluid by filtration at the glomerulus. Because of their relatively small molecular size, they pass easily through the glomerular membrane and their concentration in the glomerular.filtrate is equal to their concentration in plasma. Unless these substances are returned to the blood, they are excreted in the urine and lost from the body. In the epithelial cells of the proximal convoluted tubules, glucose and amino acids are transferred from the tubular lumen to the ISF, from where they diffuse into the peritubular capillaries. Their transport from the tubular lumen into the tubular epithelial cell is coupled with the transport of Na+. For example, Na+ and glucose (or an amino acid) are coupled to the same carrier when moving through the brush border of the epithelial cell from the lumen to the cytoplasm of the cell (Figure 11-16).
The energy for transport is associated with the active transport of Na+ through the basal and lateral membranes of the tubular epithelial cells. The active transport of Na+ out of the cell at the basal and lateral borders creates a chemical gradient for diffusion of Na+ from the tubular lumen, where its concentration is higher, into the cell cytoplasm. The transport of glucose and amino acids does not require additional energy because of their transport with Na+. Once glucose and amino acids are inside the cell and are uncoupled from their carrier, they diffuse through the basal and lateral borders into the ISF and from there into the capillaries. The protein carrier on which they were transported from the lumen into the cell with Na+ returns to its previous conformation to transport more glucose, amino acids, and Na+.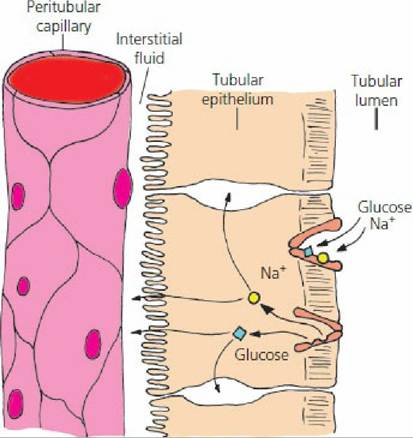
■ FIGURE 11-16 Transport of Na+ from tubular lumen into the tubular epithelial cell and its cotransport with glucose. The protein carrier conformation permits reception of Na+ and glucose from the lumen. Carrier conformational change permits Na+ and glucose release into the epithelial cytoplasm. Once released, the carrier returns to its original conformation for the reception of more Na+ and glucose. The Na+ released into the tubular epithelial cytoplasm is actively transported through the basal and lateral borders of the cells into the ISF and diffuses from there into the capillaries. Glucose follows the same pathways except that it is not actively transported. Amino acids are also cotransported with Na+ similar to that of glucose.
Because Na+ is transported from the tubular epithelial cells to the ISF, an electrical gradient is established between the ISF and the tubular lumen (lumen negative). The Cl- diffuses through membranes easily and its diffusion from the lumen follows the transport of Na+ into the tubular epithelium to maintain electrical neutrality.
Consequently the lumen has a low negativity in the proximal tubule, where much of the Na+ is reabsorbed.Reabsorption of Water and Urea
The removal of Na+, glucose, amino acids, and other substances from the lumen into the ISF and capillaries increases the concentration of water within the lumen and water is reabsorbed by osmosis into the ISF and capillaries. Reabsorption of water into the peritubular capillaries from the ISF is favored because of the relatively low HP and because of the increased colloidal osmotic pressure (loss of water, but not protein, at the glomerulus) in the peritubular capillaries. This situation is similar to that at the venous end of a muscle capillary (see Chapter 9).
The removal of water from the tubular lumen increases the concentration of diffusible substances (particularly urea), and they move from the lumen to the ISF and capillaries by simple diffusion. The proximal tubules reabsorb about 65% of H2O, Na+, Cl-, and HCO3- and 100% of the glucose and amino acids that were previously filtered at the glomerulus.
Secretion of H+, K+, NH3, and Organic Molecules
The transfer of substances from the capillaries into the ISF and hence to the tubular lumen - tubular secretion - occurs for several substances. The secretion of H+ occurs throughout the length of the nephron tubules (except in the thin limb of loops of Henle) and is coupled with the reabsorption of HCO-. The secretion of K+ occurs in the distal convoluted tubule and collecting tubules and ducts and is coupled with the reabsorption of Na+. Ammonia is secreted by the nephron tubules. Its rate of secretion varies, depending on the acid-base equilibrium of the body fluids (see later text). Several organic molecules are also secreted by the tubular epithelial cells into the tubular lumen. A substance similar to penicillin is lost from the body fluids because of tubular secretion.
Penicillin-Iike substances have been developed that persist in the body fluids for longer periods of time because their rate of secretion has been slowed.
Transport Maximum
Substances such as glucose that are associated with a carrier or that have active transport mechanisms for their reabsorption have a maximum rate at which they can be reabsorbed, known as the tubular transport maximum (Tm). When the Tm for the substance is exceeded, the substance will appear in the urine. In the disease known as diabetes mellitus, insulin is either deficient or lacking, and the movement of glucose from the plasma into body cells is impaired. Glucose concentration in the plasma therefore increases, causing the plasma and tubular loads of glucose to increase. The increased tubular load exceeds the availability of carrier molecules for its transport and reabsorption, and excess glucose continues its flow through the tubules into the urine. Because it is retained within the tubules, it contributes to the effective osmotic pressure of the tubular fluid, and water is also retained. In diabetes mellitus, glucose is detected in the urine and a greater volume of urine is formed. Greater amounts of water are lost from the body in the urine, so the afflicted animal drinks more water to compensate for the urine loss. Increased urine formation is known as diuresis. When it is caused by retention of water because of greater effective osmotic pressure in the tubular lumen, it is known as osmotic diuresis.
Not all of the hundreds of thousands of nephrons have the same Tm. The first appearance of glucose in the urine does not represent the Tm for the kidney; it represents the renal threshold (the plasma concentration of a substance when it first appears in the urine). The Tm for the kidney is reached when all nephrons are reabsorbing to their maximum ability. For glucose, the renal threshold (its plasma concentration when glucose first appears in urine) is about 180 mg/ dL and the Tm (its plasma concentration when further increments of glucose increase in the plasma result in similar increments of glucose increase in the urine) is about 260 mg/dL.
■