Edema Is a Clinically Noticeable Excess of Interstitial Fluid
Edema is a common clinical problem. Edema results either from excessive filtration of fluid out of capillaries or from depressed lymphatic function. One common cause is increased venous pressure.
Increased venous pressure can result from the application of a too-tight dressing on the extremity of an animal. The resulting constriction of the veins impedes the outflow of venous blood from the limb. Blood backs up in the limb veins, which increases venous pressure. Blood then backs up in the capillaries and increases capillary hydrostatic pressure. As shown in Figure 23-5, the increase in capillary hydrostatic pressure leads to an excessive filtration of capillary fluid into the interstitial space. When this accumulation of fluids becomes clinically noticeable, the patient is said to exhibit edema.Three factors (safety factors) limit the degree of edema. All three safety factors depend on an increased interstitial fluid
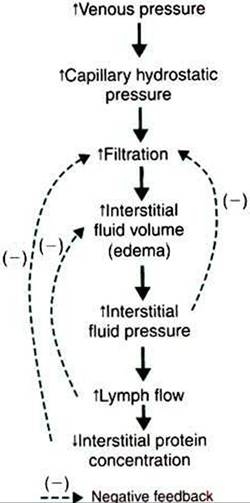
FIGURE 23-5 Increase in venous pressure leads to increase in interstitial fluid volume (edema). The dashed lines (negative feedback) indicate the counteracting effects of the three safety factors against edema. First, an increase in interstitial fluid hydrostatic pressure reduces the rate of filtration back toward normal. Second, an increase in lymph flow reduces interstitial fluid volume back toward normal. Third, a decrease in interstitial fluid protein concentration reduces the rate of filtration back toward normal.
volume leading to an increase in interstitial fluid hydrostatic pressure. The first safety factor is that the increased interstitial fluid pressure acts directly to oppose or limit filtration. Interstitial fluid pressure does not need to rise above capillary hydrostatic pressure to limit edema. Any increase in interstitial fluid pressure (e.g., from a normal value of -7 to +2 mm Hg) helps to change the net balance of the Starling forces in the direction of reducing excessive filtration.
The second safety factor against edema is that increased interstitial fluid pressure promotes lymph flow. Lymph flow removes edema fluid from the tissue and therefore helps to limit the degree of edema.
The third safety factor is an indirect consequence of increased lymph flow. Recall that interstitial fluid normally has a small amount of plasma protein, usually the result of transcytosis. This protein exerts a small but significant oncotic pressure that favors filtration. As lymph carries away interstitial fluid under these circumstances, the proteins originally present in the interstitial fluid are carried away by the lymph, and fluid relatively free of proteins is being added to the interstitial space by the increased filtration. Therefore the interstitial protein concentration and interstitial fluid oncotic pressures decrease, which helps reduce filtration.
To summarize, venous obstruction causes capillary hydrostatic pressure to increase, which increases filtration. Edema develops. Three safety factors then come into play to limit the
degree of edema. A steady-state degree of edema is eventually reached, in which interstitial fluid is removed by lymph vessels as fast as it is filtered.
Another common clinical situation that leads to an increased venous pressure (and therefore edema) is heart failure. If the right ventricle fails (i.e., if right ventricular contractility decreases), blood backs up or pools in the right atrium and venae cavae. This increase in venous and atrial pressures is beneficial in one respect: it increases preload, which helps promote diastolic filling of the failing ventricle. An increased diastolic ventricular volume helps restore the stroke volume of the failing right ventricle back toward its normal level (recall Starlings law of the heart). Although the increased venous pressure is beneficial in terms of restoring the stroke volume toward normal, the increased venous pressure often leads to excessive capillary filtration and edema in the systemic organs.
Systemic edema therefore is a common complication of rightsided heart failure. The edema is often most noticeable in the dependent regions of the body, such as the lower extremities, particularly if the patient remains standing for a long time. Systemic edema also is often noted in the abdomen. When edema develops in the abdominal organs, excess interstitial fluid tends to ooze out and accumulate in the peritoneal space. Excessive fluid in the peritoneum is called ascites. Marked ascites is common in patients with right-sided heart failure.Failure of the left ventricle leads to increased left atrial pressure and increased pulmonary venous pressure. The result is an increase in capillary filtration in the lungs, which leads to an increase in the amount of interstitial fluid in the lung tissue, or pulmonary edema. In extreme cases, some of the excess interstitial fluid oozes into the alveolar and bronchial air spaces of the lungs, and frank fluid is found in the airways. Such a patient typically coughs up a frothy fluid.
A decreased plasma protein concentration is another common cause of edema (Figure 23-6). One common cause of decreased plasma protein concentration is a decrease in the rate of plasma protein production by the liver. This occurs in malnutrition and leads to the clinical syndrome of kwashiorkor. Victims Ofkwashiorkor typically look emaciated, except that the abdomen is grossly distended by ascites (edema fluid in the peritoneum). Another cause of abnormally low plasma protein concentration is an increase in the rate of loss of proteins from the body. Protein loss occurs in kidney disease. For example, in nephrotic syndrome, the kidney glomerular capillaries become permeable to plasma proteins. Plasma proteins leave the bloodstream and enter the urinary tubules (nephrons) of the kidney. A chronic loss of proteins in the urine reduces the plasma protein concentration. Therefore the presence of substantial amounts of plasma protein in the urine is an alarming clinical sign.
Severe burns are another common cause of the loss of plasma proteins from the body. The capillaries of burned skin become permeable to both fluid and proteins. Substantial amounts of plasma can leave the body through these damaged
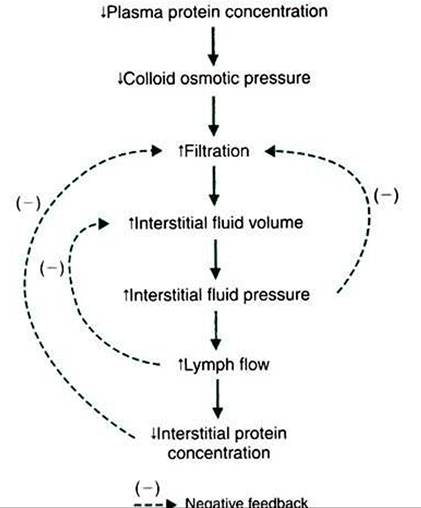
FIGURE 23-6 Decrease in plasma protein concentration leads to edema, but three safety factors limit the degree of the edema, as shown in Figure 23-5.
capillaries. The presence of plasma proteins in the fluid weeping from a burn site accounts for the typical yellow color of that fluid. If the water and electrolytes lost through burns are replaced through the intravenous administration of saline or lactated Ringer s solution or through the ingestion of salt and water, and if the plasma proteins are not replaced, the plasma protein concentration decreases.
Whether it results from decreased production or increased loss, a decrease in plasma protein concentration leads to a decrease in plasma colloid osmotic pressure. This alters the balance of the Starling forces in a direction that favors excessive filtration of fluid from the capillaries (see Figure 23-6). Interstitial fluid accumulates and edema is noticed. However, the same three safetv factors that limit edema in the case of increased venous pressure (see Figure 23-5) also operate in the case of decreased plasma protein concentration. The degree of edema is limited by (1) an increased interstitial fluid pressure, (2) an increased lymph flow, and (3) a decreased interstitial protein concentration.
Another cause of edema is lymphatic obstruction. Clinically, this situation is called lymphedema. Inflammatory diseases and cancers that produce obstruction of the lymphatic vessels cause lymphedema. Also, in certain parasitic diseases, microfilaria lodge in the lymph nodes and obstruct lymph flow. Filarial parasites cause the pronounced edema seen in cases of elephantiasis. Lymphedema also occurs as a secondary consequence of surgical procedures that damage lymph nodes.
A common example of this in human medicine is the edema of the arm that follows radical mastectomy. The removal of axillary lymph nodes during radical mastectomy creates scar tissue that impairs lymphatic drainage from the arm.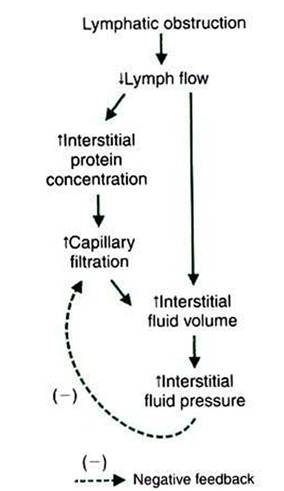
FIGURE 23-7 Lymphatic obstruction leads to edema. Lymphedema is clinically troublesome because only one of the normal three safety factors is operative to limit the degree of edema.
Figure 23-7 traces the causes of edema after lymphatic obstruction and shows why lymphedema is clinically so troublesome. Lymphatic obstruction decreases lymph flow. Interstitial fluid accumulates instead of being removed, and edema results. The accumulation of edema fluid raises interstitial fluid pressure, which acts as a safety factor to limit the excess capillary filtration. However, the second and third safety factors discussed earlier are absent in the case of lymphedema because these factors depend on an increase in lymph flow. In lymphedema a decreased lymph flow is the causative problem, so there cannot be an increased lymph flow (second safety factor) to compensate for the edema. An additional complicating factor with lymphatic obstruction is that interstitial proteins accumulate instead of being carried away by the lymph. Therefore the third safety factor that protects against edema (decreased interstitial fluid oncotic pressure) is also compromised in lymphedema.
Another cause of edema is physical injury or an allergic reaction to antigen challenges. Physical trauma, such as a scratch or a cut on the skin, results in a localized bump or swelling. A similar swelling is observed when the skin reacts to an irritating agent or antigen challenge. An allergic swelling can also occur in bronchial tissue during an asthmatic reaction. The edema of asthma can be life threatening because it limits airflow to the lungs. As shown in Figure 23-8, an injury or antigen challenge leads to the release of the chemical histamine from mast cells in the affected tissue.
Histamine has two effects that cause edema. First, histamine increases the permeability of capillaries to proteins. As proteins leave the bloodstream and accumulate in the interstitial space of the damaged tissue, they increase the interstitial fluid oncotic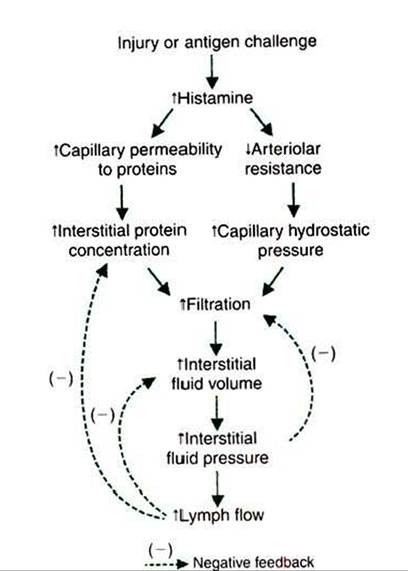
FIGURE 23-8 Histamine mediates the changes that lead to edema in response to a physical injury or an antigen challenge.The normal three safety factors against edema are intact and help to limit the degree of edema.Treatment with an antihistamine (a drug that blocks histamine receptors on arterioles and capillaries) also helps to reduce edema in these cases.
pressure, which promotes filtration of fluid. Second, histamine promotes filtration by relaxing arteriolar smooth muscle. The arterioles dilate, and the resulting decrease in arteriolar resistance allows more of the arterial blood pressure to impinge on the capillaries. This leads to an increase in the capillary hydrostatic pressure, which promotes filtration. Although histamine promotes excess fillration and edema through two mechanisms, all three safety factors that protect against edema are intact and act to limit the degree of edema.
Other situations also cause edema, but the examples discussed here cover some of the most common causes of clinical edema. These examples also reinforce an understanding of the interplay of the osmotic and hydrostatic forces that act on water to govern its filtration out of capillaries or its reabsorption into capillaries.