Several Common Physiological Changes Alter the Normal Balance of Starling Forces and Increase the Filtration of Water Out of Capillaries
An increase in capillary hydrostatic pressure (PJ favors the greater filtration of water. Capillary hydrostatic pressure can be increased by an increase in arterial blood pressure or by a decrease in arteriolar resistance.
An increase in arterial pressure causes more pressure to be transmitted down through the arterioles and into the capillaries. Likewise, a decrease in arteriolar resistance (e.g., a dilation of the arterioles) allows a greater portion of the arterial pressure to be transmitted into the capillaries. Capillary hydrostatic pressure can also be increased by a “backing up” (“damming up”) of venous blood. For example, an increase in central venous pressure causes blood to accumulate in the capillaries and raises capillary pressure. An obstruction to venous outflow (e.g., too tight a dressing on a limb) also causes blood to back up in the capillaries, which increases capillary hydrostatic pressure.Although several factors typically affect capillary hydrostatic pressure, the only important determinant of interstitial fluid hydrostatic pressure is the volume of fluid present in the interstitial space. An accumulation of interstitial fluid increases interstitial hydrostatic pressure. Removal of interstitial fluid decreases the pressure. As stated earlier, interstitial fluid hydrostatic pressure is usually slightly Subatmospheric (e.g., -7 mm Hg). When interstitial fluid hydrostatic pressure rises above atmospheric pressure, the accumulation of interstitial fluid becomes clinically noticeable as a swelling, or edema.
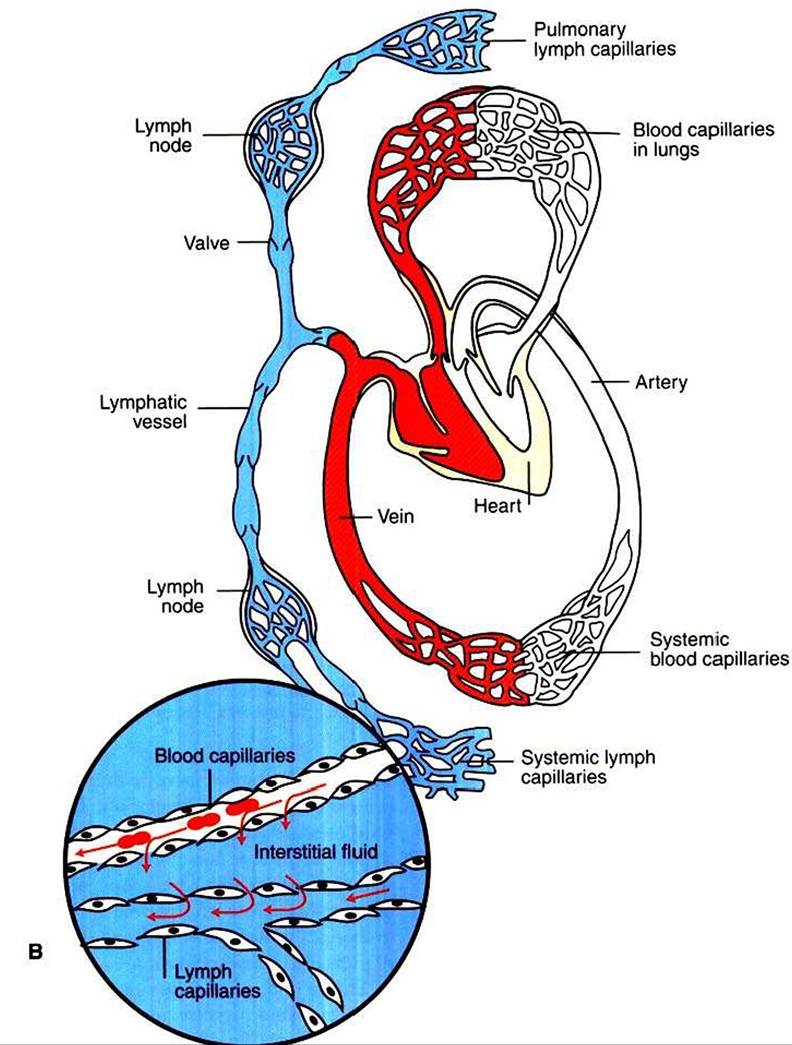
FIGURE 23-4 Continued.
The net oncotic pressure depends on the concentrations of proteins in the capillary plasma and in the interstitial fluid. The normal protein concentration in plasma is 7 g∕dl., which results in a plasma oncotic pressure of 25 mm Hg.
Any alteration in the concentration of proteins in the capillary plasma alters the plasma oncotic pressure.Similarly, changes in the interstitial protein concentration alter interstitial fluid oncotic pressure. Under normal circumstances, protein molecules are slightly too large to pass through the capillary pores or clefts. The main route for the delivery of plasma proteins into the interstitial fluid is through the three-step process of transcytosis. The first step is piιιocytosis (a form of endocytosis)i which involves the invagination of the capillary endothelial cell membrane to form an intracellular vesicle that contains plasma, including plasma proteins. Second, some of these vesicles cross the capillary endothelial cell from the side facing the bloodstream to the side facing the interstitial fluid. In the third step, some of these vesicles fuse with the outer membrane of the capillary endothelial cells; the vesicles discharge their contents into the interstitial space. This third step is called exocytosis. An increase in transcytotic activity increases the delivery of plasma proteins into the interstitial space and therefore increases interstitial fluid oncotic pressure. In addition, abnormal circumstances (e.g., tissue inflammation) can cause the capillary pores to open wide enough that plasma proteins can pass through.
Plasma proteins are removed from the interstitial space through lymph flow. The clefts or pores in the lymphatic capillaries are large enough to accommodate the passage of plasma protein molecules (in contrast to the smaller clefts or pores in blood capillaries). Therefore, when excess interstitial fluid flows into lymph capillaries, it carries with it any plasma proteins that are present in the interstitial fluid. The lymphatic fluid, containing these plasma proteins, flows to the thorax, where the fluid reenters the bloodstream at the subclavian veins.
The role of lymphatic flow in counteracting the accumulation of excessive interstitial fluid is especially important in the lungs.
Lung capillaries are more permeable to plasma proteins than are most capillaries in the systemic circulation. As a result, the oncotic pressure of interstitial fluid in the lungs is normally about 18 mm Hg. Capillary hydrostatic pressure in the lungs is generally about 12 mm Hg. (This value is lower than the capillary hydrostatic pressure for systemic capillaries because pulmonary arterial pressure is so much lower than systemic arterial pressure.) Interstitial hydrostatic pressure in the lungs is generally about -4 mm Hg (the same as intrapleural pressure). Summation of these Starling forces for lung capillaries yields the following: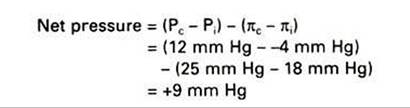
A net pressure of 9 mm Hg indicates that there is a substantial driving force for filtration of fluid out of the capillaries and into the lung interstitial spaces. The lung interstitial spaces would fill rapidly with water, and pulmonary edema would develop, were it not for the well-developed system of lymph vessels in the lungs. These vessels continuously remove interstitial fluid and prevent its excessive accumulation.