Elimination systems
Key points
■ Somatic innervation causes contraction of the external (striated muscle) urethral sphincter. Fibres arise in the S1-S3 spinal cord segments and travel via the pudendal nerve.
■ Parasympathetic innervation causes contraction of the detrusor muscle of the bladder wall and passive opening of the internal (smooth muscle) urethral sphincter. Fibres arise in the S1-S3 spinal cord segments and travel via the pelvic nerve.
■ Sympathetic innervation causes relaxation of the detrusor muscle of the bladder wall and contraction of smooth muscle in the bladder neck. Fibres arise in the L1-5 spinal cord segments and travel via the hypogastric nerve.
■ Visceral afferent fibres from the urinary bladder and sphincters travel via the pelvic nerve to the sacral spinal cord. They link to efferent fibres for reflex function and also travel to the brain for conscious awareness.
■ Reflex arcs for urination are located in the sacral and lumbar spinal cord and are influenced by UMN tracts from brainstem micturition centres, the cerebellum and the cerebrum.
■ Urinary and faecal incontinence occur after damage to either UMNs or LMNs, but the clinical signs are distinct for each type of injury.
■ Disruption of UMN tracts cranial to the sacral spinal cord can result in an ‘upper motor neuron bladder’; this is characteristically full, turgid and difficult to express.
■ Disruption of the sacral spinal cord, or the pelvic, or pudendal nerves can result in a ‘lower motor neuron bladder’; this is characteristically overdistended, flaccid and easy to express.
Receptors in the bladder wall and neck are sensitive to stretch or pressure. Afferent input is via the pelvic and pudendal nerves to the sacral spinal cord (S1-S3 segments).
Neural input from the bladder can stimulate reflex function via synapses in the sacral or lumbar (L1-4 or 5) spinal cord segments.
The input is also projected to the brain for coordination of bladder/sphincter function and for conscious perception (Fig. 12.7).1. Efferent fibres from the sacral spinal cord (S1-3). Somatic neurons that connect to the striated muscle in the urinary sphincter leave S1-S3 segments and travel via the pudendal nerve to cause contraction of the sphincter and urine retention. This is the most important sphincter for urinary continence. The pudendal nerve supplies the striated muscle of the anal sphincter, thereby forming the efferent arm of the perineal reflex; it also contributes sensory input from the perineum. Parasympathetic innervation originating in the sacral spinal cord travels via the pelvic nerve plexus to the detrusor muscle (smooth muscle) of the bladder wall for contraction. The oblique orientation of the smooth muscle at the bladder neck causes it to passively open when the detrusor contracts. Parasympathetic stimulation functions in bladder contraction and evacuation. The pelvic nerve also supplies parasympathetic fibres to the reproductive organs, rectum and descending colon. The pelvic nerve combines with the hypogastric (sympathetic) nerve to form the pelvic plexus located on either side of the rectum.
2. Lumbar cord neurons (L1-4 or 5). Sympathetic fibres leave the lumbar spinal cord segments and travel via the splanchnic nerves to the caudal mesenteric ganglion, synapse and then via the hypogastric nerve to the pelvic plexus. From there they innervate the smooth muscle of the bladder wall inducing relaxation of the detrusor muscle via β-receptors. They also innervate smooth muscle of the bladder neck where they stimulate α-receptors causing contraction. Thus sympathetic stimulation facilitates urine storage. A distinct smooth muscle sphincter in the bladder neck has not been defined anatomically.
3. Brain. Ascending fibres travel to the brain via the lateral spinothalamic tract and the fasciculus gracilis. They synapse in the following areas:
(a) Brainstem micturition centres such as the reticular formation of the pons.
Reticulospinal tracts carry UMN fibres back down the spinal cord to connect with both visceral and somatic LMNs to stimulate urine storage, or voiding, as appropriate.(b) The cerebellum; this has a mainly inhibitory effect on urination.
(c) The cerebrum, thereby informing the animal of bladder distension. The forebrain controls learned toileting behaviour and connects with the micturition centres of the pontine reticular formation for voluntary control of storage and micturition.
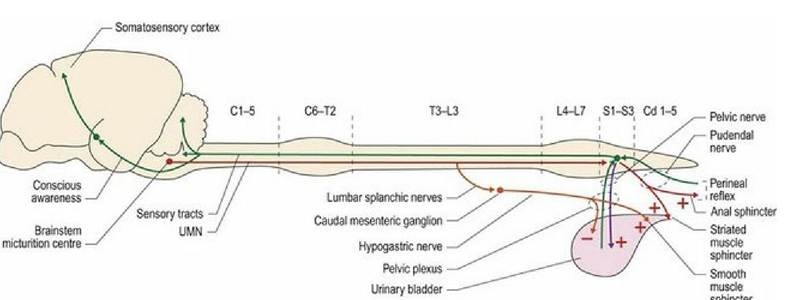
Fig. 12.7 Innervation of the urinary bladder. Sensory input to the brain travels via the dorsal and lateral funiculi, while UMN fibres travel in the lateral and ventral funiculi (see also figure 13.15).
Urinary bladder function
In the normal animal the distended bladder is located cranial to the pelvic brim and the bladder cavity sits ventral to the urethral outflow; therefore gravity aids urine retention. The position of the bladder relative to the urethra is a key component of urine storage in both the standing and recumbent animal. Changes in the animal’s posture cause abdominal compression and may result in urine surging into the neck of the bladder. The distension of the bladder neck stimulates reflex urethral contraction and hence continence. The cause of urine spurting in excited puppies may be due to increased sympathetic tone and abdominal muscle contraction causing urine to surge into the urethra. Reflex urethral contraction may not be sufficiently facilitated by learned behaviour and so the excited puppy urinates inappropriately. Coordination of bladder wall contraction and sphincter relaxation (micturition), or vice versa (storage), is mediated reflexively in the sacral spinal cord and by micturition centres in the pons. Cerebral function modulates reflex activity and toileting behaviour (Table 12.4).
Table 12.4 Nerve function during urine storage and voiding
| St0ra9∙ phase | Afferent | Parasympathetic | Somatk | Sympathetic |
| Storage and bladder filling | Increasing firing rate as bladder distends. Stimulation of brain stem and somatosensory cortex | Minimal, thus bladder wal relaxation | Reflex and voluntary stimulation of striated muscle Sphncter contraction | α-adrenerg∣c for contraction of smooth muscle sphincter β*adre∩erglc for Inhibition of bladder wall smooth musde contraction |
| Bladderemptying | Initial i∩σease in Intravesicular pressure causing stimulation then deσeased stimulation as the bladder deflates | Stirrxiatlon - Nadder wall contraction | Inhibition Stnated m?sde Sphncter relaxation | Inhibition of Ofadrenerglcfibres (relaxed smooth muscle of sphincter) Minimal β∙adrenergκ stimulation, so not opposing bladder wall contraction |
Dysfunction of innervation of the urinary bladder
Urinary incontinence includes signs of inappropriate urination and failure to urinate.
The ‘upper motor neuron bladder’ occurs when the UMN tracts (central motor neurons) cranial to the sacral spinal cord have been disrupted. Loss of UMN input results in loss of inhibition of the somatic outflow, thus striated muscle sphincter contraction is sustained. However, as the parasympathetic innervation to the detrusor muscle is intact, bladder wall tone is maintained. Hence the animal will have a full, turgid bladder that is difficult to express. Note as the overdistended bladder may reflexively trigger parasympathetic outflow and detrusor muscle contraction, urine spurting may occur. Sustained (chronic) bladder overdistension can lead to an irreversible breakdown of the detrusor smooth muscle syncytium and may ultimately lead to decreased tone in the bladder wall.
Normally, bladder distention can trigger reflex inhibition of sympathetic outflow, thereby permitting urination. Lesions between L4 and l7 can block ascending, reflex inhibition to sympathetic neurons.
Sustained sympathetic outflow facilitates contraction of the smooth muscle in the bladder neck and compounds urine retention.Spinal cord lesions may also block impulses travelling to the brain and the animal is not aware of having a full bladder; toileting behaviour is not initiated.
If the UMN lesion is chronic, then a reflex bladder may develop after several weeks. Bladder distension triggers reflex parasympathetic stimulation and inhibits somatic and sympathetic outflow (Fig. 12.8). The bladder contracts as the sphincters relax. Mild abdominal pressure may be sufficient to set off reflex micturition. However, micturition may not be complete, leaving a residual volume of urine in the bladder and predisposition to urinary tract infections.
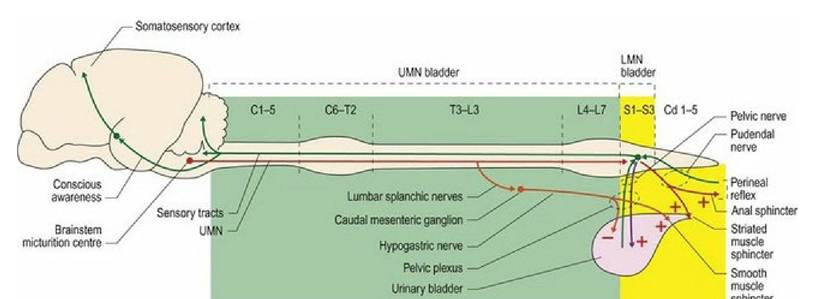
Fig. 12.8 Lesions in the aqua-highlighted area would result in an UMN bladder (turgid, difficult to express), while lesions in the yellow-highlighted area would result in a LMN bladder (large, flaccid, easy to express).
The ‘lower motor neuron bladder’ occurs with disease affecting the sacral spinal cord, sacral nerve roots, pudendal and/or pelvic nerve. Loss of LMN (peripheral motor neuron) function results in the loss of parasympathetic stimulation of detrusor muscle contraction, reduced tone in the bladder wall and overdistension of the bladder. Striated muscle sphincter tone is lost due to damage to the somatic LMNs. The LMN bladder is large, flaccid and easy to express manually. The animal may dribble urine as it moves around due to changing abdominal pressure on the bladder. The bladder is full and there is overflow incontinence, but voiding is not sustained as detrusor muscle contraction is lost. A relaxed urinary sphincter may predispose the animal to ascending urinary tract infections. Sympathetic innervation to the smooth muscle of the bladder neck may lead to partial closure of the urethra but is insufficient to keep the urethra fully closed.
The animal may also have a dilated anus as the pudendal nerve also supplies the anal sphincter. This may result in faecal incontinence and loss of the perineal reflex.Like any LMN lesion, reflex activity is compromised so reflex micturition will not occur. The lesion is also likely to damage afferent input, further compromising reflex function and conscious awareness of bladder distension.
Other sites of dysfunction
Damage to just the pelvic nerve will leave the anal and urinary sphincters intact, but the bladder will be atonic and distended and there will be no perception of filling.
Brainstem lesions may result in similar signs to UMN bladder.
Cerebellar lesions may result in pollakiuria or increased frequency of urination. This is because the cerebellum usually has an inhibitory effect of urination. Other, more obvious cerebellar signs are likely to dominate the pollakiuria.
Cerebral lesions may result in loss of learned, toileting behaviour, but storage and micturition still occur.
Defaecation
Key points
■ Innervation of the rectum is similar to that of the urinary bladder, with visceral afferent and parasympathetic fibres travelling in the pelvic nerve. Somatic afferent (from the anal sphincter and perineum) and efferent fibres to the anal sphincter travel in the pudendal nerve. The sacral spinal cord is the origin of both nerves.
■ UMN and LMN faecal incontinence are differentiated based on tone of the anal sphincter and activity of the perineal reflex.
■ Defecation will still occur with either UMN or LMN disease due to the activity of local neural networks in the bowel/rectal wall causing colonic contraction.
The innervation of the rectum and anal sphincter is similar to that of the urinary bladder. Sympathetic input from L1-L4 or 5 spinal cord segments, via the hypogastric nerves, innervates the descending colon, rectum and internal smooth muscle sphincter of the anus. Originating in the sacral spinal cord, parasympathetic fibres innervate the descending colon and rectum via the pelvic nerve. Somatic fibres from the sacral cord innervate the striated muscle of the well-defined external anal sphincter via the pudendal nerve. The sympathetic innervation inhibits colonic and rectal activity and stimulates contraction of the smooth muscle sphincter, while the parasympathetic innervation stimulates colonic and rectal motility. The somatic innervation is critical for faecal continence by causing contraction of the striated muscle in the anal sphincter. Afferent fibres from the rectal wall, sphincters and perineum ascend in the dorsal and lateral funiculi to the brainstem centres for UMN regulation and to the cerebral cortex for conscious perception.
Defecation involves coordinated activity in the parasympathetic, somatic and sympathetic nervous systems. However, as it also involves reflex activity utilising local neural networks in the bowel/rectal wall, contraction of the colonic and rectal walls can still occur in the absence of sacral spinal cord input. Thus defecation may occur in animals with LMN lesions; that is involving LMNs in the sacral spinal cord, pelvic and pudendal nerves. The animal is unlikely to be aware of it due to loss of visceral and somatic afferent input. Damage to LMNs supplying the pudendal nerve would lead to a dilated anus and loss of the perineal reflex (Fig. 12.9).
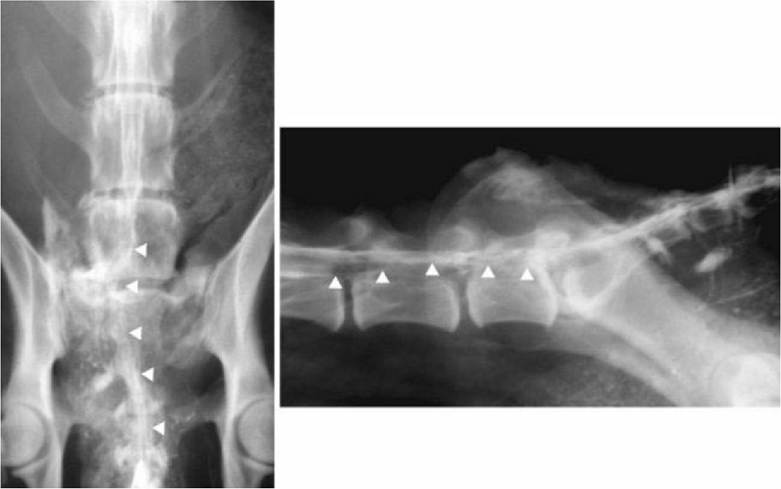
Fig. 12.9 Radiographs from a dog with LMN signs to the urinary bladder and rectum caused by a tumour affecting the sacral spinal cord and nerve roots. Myelogram-epidurograms, taken from the ventrodorsal and lateral aspects. Arrowheads highlight the deviation of the sacral and caudal spinal cord segments due to the presence of the tumour. At presentation, this dog dribbled urine and had 2 litres of urine in its bladder. It also had no anal tone and was faecally incontinent.
In animals with lesions cranial to the sacral spinal cord (UMN lesions), then defecation still occurs, due to local reflex activity involving the spinal cord; again the animal may be unaware of the process. Small lesions affecting the dorsal funiculus may affect conscious perception of rectal distension and lead to loss of voluntary defecation with minimal effect on pelvic limb gait.