Key points
■ The primary aim of the neurological examination is to localise the lesion.
■ The neurological examination assesses behaviour and arousal, sensory systems, motor function, cranial nerve function, spinal reflexes and, particularly in companion animals spinal hyperpathia (spinal pain).
Methods of examination have to be adjusted according to the species being examined.In veterinary medicine the primary aims of the clinical neurological examination are to establish whether a neurological disease exists and, if it does, to localise the lesion.
Localising the lesion is done by assessing the results of the neurological examination. Lesion localisation is essential as diseases are often region-specific and determining which region(s) is involved permits the clinician to establish a list of possible causes and then pursue appropriate diagnostic tests.
For example, a different region of their nervous system will need to be evaluated diagnostically in an animal that has proprioceptive deficits, paresis and normal cranial nerve function, compared with one that has proprioceptive deficits, no paresis, but has vision deficits in one eye. The former is probably a spinal cord lesion and the latter is probably a forebrain lesion. To localise the lesion, it is just as important to identify the neural functions that are NORMAL as well as those neural functions that are ABNORMAL.
To localise the lesion, the clinician observes the animal closely and performs specific, neurological tests that evaluate the function of different neural systems.
Note that a full physical examination including assessment of the ocular fundus must be performed for the clinician to diagnose and treat appropriately the animal’s condition. Many neurological conditions are associated with diseases elsewhere in the body. Tumours (multicentric or metastatic), metabolic and nutritional diseases, trauma, intoxications and vascular conditions are just some of the examples of systemic diseases that can cause neurological signs.
The following describes the neurological examination in a domestic cat or dog but the general principles are similar for large animals. Specific comments are given to modify the examination for large animals. This chapter represents the culmination of all the functional neuroanatomy described in chapters 1-12. Please see specific chapters for further details of structure and function.
During the examination, tests are performed that evaluate the following neural functions:
1. Behaviour and arousal;
2. Ascending sensory systems - tactile, proprioception and nociception;
3. Motor function;
4. Cranial nerve function;
5. Spinal reflexes;
6. Spinal hyperpathia (spinal sensitivity or pain).
From the results of the tests, the clinician determines:
(a) Whether the animal has neurological deficits;
(b) Which parts of the nervous system are functioning normally;
(c) Which parts are functioning abnormally.
Using their knowledge of where those neural functions are situated in the CNS and PNS, the clinician should then be able to localise the lesion. Only when the lesion is localised can the clinician devise a sensible list of differential diagnoses and plan appropriate diagnostic tests. All this has to be done before appropriate treatment can be prescribed. Note: sometimes it can be quite difficult to localise a lesion and the neurological examination may need to be repeated several times to confirm results.
For example, if an animal is dysmetric and ataxic but is alert with good motor strength and cranial nerve function, then the lesion is unlikely to be in the spinal cord (i.e. no paresis), the forebrain or brainstem (normal arousal and cranial nerve function). However, a cerebellar lesion would account for the dysmetria and ataxia (incoordination) with preservation of the other neural functions.
It matters little where a lesion is located on a pathway (origin, midway along the pathway, or termination), it will still produce similar signs of dysfunction.
This is analogous to a battery (origin), connecting wire (the pathway) and a light (end of pathway). Dysfunction in any one of those sections will cause the same outcome (clinical sign), that is, the light will not work. Most regions of the nervous system are associated with a number of functions either because a neural pathway begins or ends in that region, or is passing through it. The key to localising the lesion is based on having knowledge about which neural functions are associated with that region, and, conversely, which functions are not.If a lesion is in a particular region, then it could damage pathways in that region and cause signs of dysfunction. However if a pathway does not pass through that region, then it will not be affected. Identifying the neural pathways that are functioning normally indicates to the examiner that the lesion is NOT located in the region that those systems occupy.
For example, if the lesion is in the thoracolumbar spinal cord, then pathways passing through that part of the cord may be damaged (see Fig. 13.15), such as proprioception and UMN tracts to the pelvic limbs causing proprioceptive deficits (conscious and subconscious) and either paraparesis or paralysis. But the lesion will not affect the cranial nerves, arousal or the function of the thoracic limbs, as those neural systems are not associated with the thoracolumbar spinal cord (Fig. 13.1).
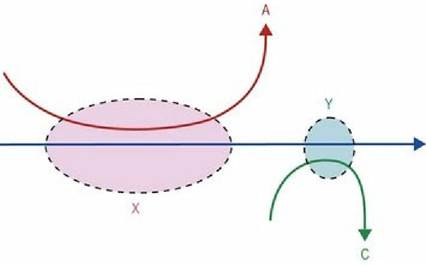
Fig. 13.1 Consider an animal that presents with clinical signs referable to damage to pathway B. Pathway B is a long pathway, so to determine where the lesion affecting pathway B might be located, the examiner would assess the function of other neural pathways such as A and C. If the animal also has signs referable to damage to pathway C, but not A, then that would suggest that the lesion localises to region Y, not X.
An applied example of this diagram would be the animal that has conscious proprioception deficits on the right side of the body and blindness in the right eye (see Fig. 4.10). The conscious proprioceptive pathway (e.g. ‘B’ in Fig. 13.1) begins in the sensory receptors in the forepaw, travels via spinal nerves into the spinal cord, travels cranially in the ipsilateral cervical spinal cord, into the brainstem, crosses over and passes rostrally on the contralateral side to the somatosensory cortex. The lesion could be anywhere along that long pathway. ‘A’ represents the cranial nerves that attach to the brainstem (III-XII) and the UMN centres in the brainstem and ‘C’ represents the visual pathway. As there are no other cranial nerve deficits, or paresis, then the lesion is unlikely to be in region ‘X’. But both the right-side visual pathway (C) and right side proprioception are associated with the left side of the forebrain. Thus the lesion is in region ‘Y’.