End-Diastolic Ventricular Volume Is Determined by Ventricular Preload, Ventricular Compliance, and Diastolic Filling Time
Ventricular preload is the pressure within a ventricle during diastolic filling. Because ventricular pressure changes throughout filling (see Figure 21-1), the value of ventricular pressure at the end of diastole is usually accepted as a singular measure of preload.
Normal values of preload (end-diastolic ventricular pressure) are about 3 mm Hg for the right ventricle and 5 mm Hg for the left ventricle. In a normal heart, ventricular pressure at the end of diastole is essentially equal to atrial pressure because the AV valves are open widely up until the end of diastole. Also, because there are no valves between the veins and the atria, the atrial pressure is almost identical to the pressure within the nearby veins. Thus, pulmonary venous pressure, left atrial pressure, and left ventricular end-diastolic pressure are all essentially equivalent measures of left ventricular preload. Similarly, right ventricular end-diastolic pressure, right atrial pressure, and vena caval pressure are all essentially equivalent measures of right ventricular preload. In the clinic, right ventricular preload is measured by introducing a catheter into a peripheral vein (e.g., the jugular vein) and advancing it into the cranial vena cava (precava) or right atrium. Such a catheter is called a central venous catheter, and the pressure measured at its tip is called central venous pressure. Left ventricular preload is more difficult to measure clinically because there is no easy way to place a catheter tip into the left atrium or pulmonary veins.Figure 21-3, B, shows that increases in preload are associated with increases in end-diastolic ventricular volume. The graph depicts a left ventricle that has a natural volume of 30 mL in a relaxed, nonpressurized state (i.e., when the preload equals 0 mm Hg). Increases in preload distend and fill the ventricle.
A preload of 5 mm Hg brings about the normal left ventricular end-diastolic volume of 60 mL. However, an elastic limit is reached when the ventricular volume approaches 90 mL. Further increases in the preload do not cause much additional ventricular filling.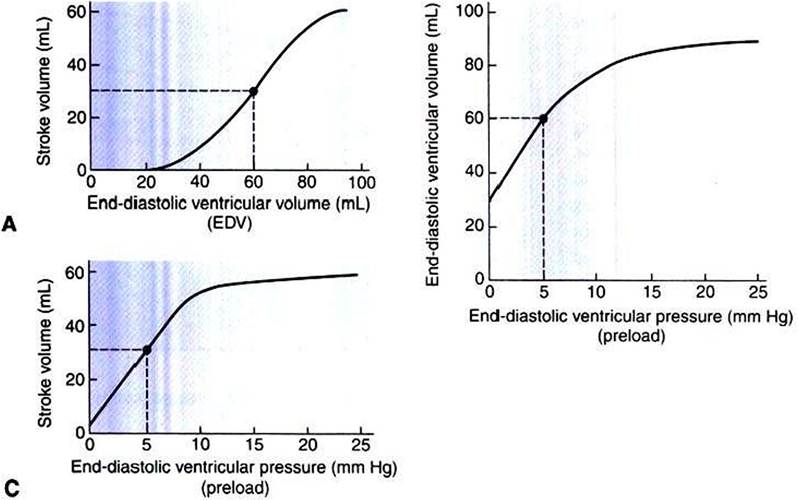
FIGURE 21-3 A, Increase in end-diastolic ventricular volume causes increased stroke volume. B, Increase in end-diastolic ventricular pressure (preload) causes increased end-diastolic ventricular volume. Cr Combines the relationships of A and B to show that an increase in ventricular preload causes increased stroke volume. An upper limit is reached in each relationship (A to O primarily because, at high levels of
B end-diastolic ventricular volume, the ventricular walls become stretched to their elastic limit.The numerical data are for the left ventricle of a large dog.The points and dashed lines indicate normal values for the resting state.
Increases in ventricular preload cause increases in end- diastolic volume (Figure 21-3, B), and increases in end-diastolic volume cause increases in stroke volume (Figure 21-3, A). Therefore, it follows that increases in preload cause increases in stroke volume (Figure 21-3, C). Each of these relationships reaches an upper limit. Several factors are involved, but the main one (already mentioned) is that the ventricular walls become stretched to their elastic limit at high levels of end- diastolic ventricular volume. In a resting dog the normal values of ventricular preload, end-diastolic volume, and stroke volume are about midway between their minimum and maximum values (Figure 21-3). Therefore a decrease below normal in preload will cause a decrease in both end-diastolic ventricular volume and stroke volume. This happens, for example, in response to hemorrhage (see Chapter 26).
The relationships among ventricular preload, end-diastolic volume, and stroke volume were first studied in detail by Ernest Henry Starling.
The observation that changes in preload cause corresponding changes in end-diastolic ventricular volume and stroke volume is called Starlings law of the heart. The Starling mechanism is critical for moment-to-moment adjustments of stroke volume. For example, if the right ventricle begins, for any reason, to pump an increased stroke volume, the resulting additional pulmonary blood flow causes an increase in the pulmonary venous pressure, which increases left atrial pressure, which in turn increases left ventricular preload, which, furthermore, increases the filling of the left ventricle during diastole. The resulting increase in left ventricular end-diastolic volume leads to a greater stroke volume from the left ventricle. Thus an increase in right ventricular stroke volume quickly results in a corresponding increase in left ventricular stroke volume. The reverse is also true.The sequence just described has a potential for developing into a vicious circle, with runaway increases in stroke volume. Other control mechanisms prevent this from happening, as discussed in Chapter 25. The point here is that the Starling mechanism keeps the stroke volumes of the left and right ventricles balanced. If this equality were not maintained (and one ventricle pumped more blood than the other for several minutes), a large part of the body’s blood volume would accumulate either in the lungs or in the systemic circulation.
An alternate name for Starling’s law of the heart is heterometric autoregulation. This name implies self-control (autoregulation) of stroke volume as a result of different (hetero) initial volumes (metric); that is, Iieteronietric refers to different end-diastolic volumes.
End-diastolic ventricular volume is determined not only by preload but also by ventricular compliance. Compliance is a measure of the ease with which the ventricular walls stretch to accommodate incoming blood during diastole. A compliant ventricle is one that yields easily to preload pressure and readily fills with blood during diastole.
Compliance is more rigorously defined as the change in volume divided by the change in pressure. Ventricular compliance therefore corresponds to the slope of a ventricular volume versus pressure curve, such as the one shown in Figure 21-3, B. This figure shows that a normal ventricle is quite compliant over the range of ventricular volumes up to and including the normal end-diastolic ventricular volume. Within this range, small changes in preload result in substantial changes in end-diastolic ventricular volume. At preloads higher than about 10 mm Hg, however, the ventricle becomes less compliant (stiffer). Inelastic connective tissue in the ventricular walls prevents increases in ventricular volume above about 90 mL.Myocardial ischemia, certain cardiac diseases, or mere advancing age can cause the ventricular walls to become stiff and noncompliant even at normal preloads. Figure 21-4 shows a comparison of volume versus pressure curves for a normal ventricle and for a noncompliant ventricle. In the noncompliant ventricle, there is a smaller increase in ventricular volume for any given increase in ventricular preload. As a consequence, a larger-than-normal preload is needed to obtain a normal end-diastolic ventricular volume and to achieve a normal stroke volume. An elevated preload necessitates elevated atrial and venous pressure, which leads to edema (detailed in Chapters 23 and 26). Thus, stiffening of the left ventricle leads to elevated pressure in pulmonary veins and pulmonary edema; stiffening of the right ventricle leads to elevated pressure in the systemic veins and systemic edema.
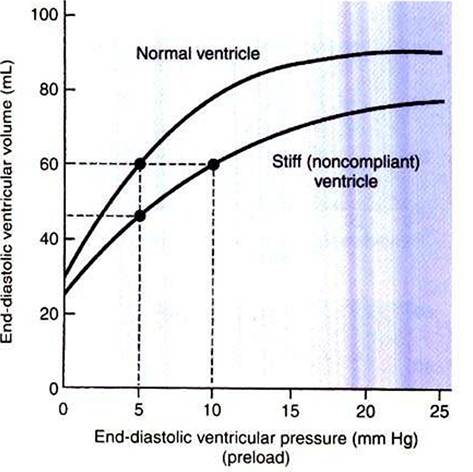
FIGURE 21-4 Stiff, noncompliant ventricle requires a higher filling pressure (preload) to reach a normal degree of filling (end-diastolic ventricular volume).
In addition to preload and compliance, the third factor that affects ventricular end-diastolic volume is the length of time available for ventricular filling during diastole.
Heart rate is the main determinant of diastolic filling time. At a normal resting heart rate, there is ample time for ventricular filling during diastole; in fact, ventricular filling is almost complete even before atrial systole occurs. As heart rate increases, however, diastolic duration decreases. At heart rates greater than about 160 beats per minute, the shortness of diastolic filling time precludes achievement of normal end-diastolic ventricular volume. This limitation on ventricular filling would dramatically reduce stroke volume when heart rate is high if not for an additional, compensating influence brought about by the sympathetic nervous system, as discussed later.Figure 21-2 (left side) provides a useful summary of the preceding discussion. End-diastolic ventricular volume is determined by ventricular preload, ventricular compliance, and diastolic filling time. An elevated preload increases ventricular filling. Decreased ventricular compliance or decreased diastolic filling time can limit ventricular filling.