Increases in Ventricular Contractility Cause Decreases in Ventricular End-Systolic Volume
Contractility refers to the pumping ability of a ventricle. With increased contractility, there is a more complete emptying of the ventricle during systole and therefore a decreased end-
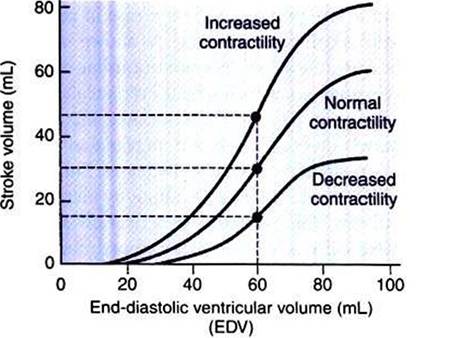
FIGURE 21-5 Increase in cardiac contractility is identifiable graphically as a leftward and upward shift of the ventricular function curve.
Increase in contractility means that there will be a larger stroke volume for any given end-diastolic volume. Conversely, decrease in contractility (rightward and downward shift) means that there will be a smaller stroke volume for any given end-diastolic volume. With normal contractility and a normal end-diastolic volume of 60 mL, the end-systolic volume is 30 mL, and so the stroke volume is 30 mL (middle dot). An increased contractility with no change in end-diastolic volume results in more systolic emptying. For example, if the end-systolic volume is reduced to 15 mL, the stroke volume increases to 45 m L (upper dot).systolic volume (see Figure 21-2, middle). An increase in contractility brings about an increase in stroke volume without requiring an increase in end-diastolic volume. Figure 21-5 shows graphically that increased contractility results in an increased stroke volume for any given end-diastolic volume.
Sympathetic nerve activity increases ventricular contractility through the action of the neurotransmitter norepinephrine, which activates β-adrenergic receptors on ventricular muscle cells. As discussed in Chapter 19, activation of β-adrenergic receptors leads to an increased influx of extracellular Ca2+ into cardiac cells during an action potential (and to several other effects); the overall result is that cardiac contractions are stronger, quicker to develop, and shorter. Epinephrine and norepinephrine released from the adrenal medulla and circulating in the blood can likewise activate β-adrenergic receptors and increase contractility, as can β-adrenergic agonist drugs (e.g., epinephrine, isoproterenol).
The cardiac glycosides (e.g., digitalis) are another class of drugs that increases cardiac contractility, again by increasing the cytosolic Ca2+ concentration during an action potential.If cardiac contractility becomes depressed, there is Iess- than-normal ventricular emptying during systole. End-systolic volume increases, and stroke volume decreases, as shown in Figure 21 - 5. A decrease in sympathetic activity causes a decrease in cardiac contractility, as do β-adrenergic antagonist drugs, which block the β-adrenergic receptors on cardiac muscle cells. Propranolol and atenolol are the β-adrenergic antagonists used most often to decrease cardiac contractility. As with β- adrenergic antagonists, calcium channel-blocking drugs also decrease cardiac contractility by making less Ca2+ available for the activation of the contractile proteins. Barbiturates, opioids, and some general anesthetics depress cardiac contractility as well; this must be kept in mind, particularly when administering such drugs to a patient who may already have compromised cardiac function. A decrease in cardiac contractility causes a decrease in stroke volume and therefore cardiac output. Consequently, the patient s blood pressure may fall to dangerously low levels.
A decreased cardiac contractility is the hallmark of the general clinical condition called heart failure (myocardial failure). Although there are many forms of heart failure, they share one characteristic: a decrease in pumping ability of one or both ventricles. Heart failure can result from coronary artery disease, myocardial ischemia, myocardial infarction, myocarditis, toxins, or electrolyte imbalances.
Although ventricular contractility is usually the predominant factor affecting ventricular end-systolic volume, the effect of arterial blood pressure must also be considered. A substantial increase in arterial blood pressure impairs ventricular ejection because the left ventricular pressure during systole must exceed aortic pressure before ejection of blood from the ventricle can occur.
Arterial pressure is called the cardiac afterload; this is the pressure against which the ventricle must pump in order to eject blood. The higher the afterload, the more difficult it is for the ventricle to eject blood. If arterial pressure is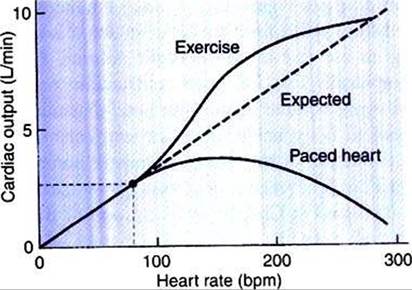
FIGURE 21-6 ■ Dashed line shows the expected increase in cardiac output in proportion to increases in heart rate (assuming stroke volume remains constant). However, if the heart is paced to higher and higher rates, the observed increase in cardiac output is less than expected because stroke volume decreases (lower solid line). In contrast, when a dog increases its own heart rate through sympathetic activation (e.g., during exercise), cardiac output increases even more than expected because stroke volume increases (upper solid line).
excessively high, ventricular ejection is impaired, end-systolic volume increases, and stroke volume decreases. This effect is minor for a normal heart and within the normal range of arterial pressure. However, high afterload can significantly limit stroke volume for a heart that is in failure.